
Abstract
Objectives:
The most common pathologies of the seminal tract are persistent hematospermia, seminal vesicle stones, and seminal duct obstruction. Endoscopic diagnostic work-up of the seminal tract is impeded by complex anatomy and lack of technical equipment. To date, there is no standardized endoscopic approach. The purpose of this study was to investigate the applicability and feasibility of a flexible microoptical device for atraumatic endoscopy of the seminal tract in a male human cadaver.
Materials and Methods:
The transurethral endoscopic examination was performed on a male cadaver. No premortal interventions or diseases of the genitourinary tract had been reported. The seminal orifice was identified via cystoscopy and accessed by the Seldinger technique using a hydrophilic guidewire and ureteral catheter. Retrograde endoscopic inspection of the distal seminal tract was performed using a miniaturized flexible endoscope. An antegrade endoscopic inspection of the seminal tract was carried out via high scrotal access to the vas deferens.
Results:
Structures of the seminal tract, such as the ejaculatory duct, seminal vesicles, and distal portion of the ductus deferentes, were visualized using the miniaturized endoscope. Image quality allowed identification of anatomical structures and characterization of tissue properties. The technical limitations we observed involved the system's maneuverability.
Conclusions:
Initial results of this novel endoscopic approach to the seminal tract using a flexible microoptical system are encouraging. However, considerable anatomical limitations of the targeted organs necessitate further refinements of the technical equipment. This approach might improve diagnostics and treatment of genitourinary diseases. Future surgical techniques may include intraseminal laser therapy or endoocclusion to monitor fertility in men.
Introduction
T
These articles primarily describe techniques of forced transutrical insertion of ureteroscopic devices to visualize the seminal tract's endoluminal anatomy, primarily focusing on the seminal vesicles. 1,9 –11 However, this approach is problematic because of the potential negative long-term effects and as paracollicular scarring may obstruct the iatrogenic peripheral ejaculatory duct. Conclusive follow-up data of these investigations, including semen analysis, are usually not collected. Short- and long-term adverse events have not been explored and published so far.
Since the anatomy of the ejaculatory duct has been studied extensively, we know that its orifice is located lateral to the verumontanum and not in the cavum utriculi of the colliculus seminalis. 12,13 Anatomically speaking, any transutricular endoscopy of the seminal tract must be considered traumatic and potentially risky to the patient. It would therefore be desirable to have an atraumatic minimally invasive option for inspecting the human seminal tract structures for diagnostic and therapeutic purposes.
Rapid development of medical instruments in terms of their miniaturization and further evolution of flexible endoscopy systems might provide new technical possibilities for accessing male internal genital organs. In this study, we investigated the applicability and feasibility of a novel flexible microoptical endoscopic device for atraumatic vesiculovasoscopy (flexible vesiculovasoscopy [FVV]) of the seminal tract in a male human cadaver model.
Materials and Methods
The endoscopic procedure was conducted via transurethral access on a male nonformalin-fixed cadaver. No premortal interventions or pathologies were reported in the genitourinary tract. The cadaver was examined in supine position. The urethra was lubricated by applying 10 mL Instillagel® (Farco-Pharma®, Cologne, Germany). Initially, a urethroscopy was performed using a standard cystoscope (CH 22; Storz®, Tuttlingen, Germany). The prostatic utricle was intubated using a semirigid ureteroscope (7.5F; Richard Wolf, Knittlingen, Germany). As we were unable to accurately identify the ejaculatory duct orifice at the seminal colliculus initially, a high scrotal incision of about 1 cm was made and the vas deferens (VD) isolated microsurgically. After carefully cannulating the VD with a 23-gauge needle, methylene blue solution was injected antegradely. Once the lateral wall of the colliculus revealed bluish discoloration, the seminal orifice could be cystoscopically identified and intubated using a ureteral catheter (5F). A hydrophilic nitinol core guidewire (HiWire™; Cook®, Bloomington, IN) was inserted into the ejaculatory duct, and the ureteral catheter was advanced into the duct via the Seldinger technique.
After removing the guidewire, the seminal tract was inspected endoscopically using a specially made miniaturized flexible endoscope (Schölly® Fiberoptic GmbH, Denzlingen, Germany). The outer diameter of the endoscope measured 0.35 mm (1.05F). Working length was 500 mm, and the optical resolution was 3,000 pixels (Fig. 1). The endoscope was connected to a compact endourology video camera unit (CMOS Full HD Camera, PV 470; Aesculap AG, Tuttlingen, Germany) and a light source with a common light cable (Power LED 175 SCB; Storz). A supportive irrigation system with a double-ended Luer lock adapter (Cook) was connected to the ureteral catheter and a conventional Luer lock 20-mL syringe. We also carried out antegrade vasoscopy from the high scrotal isolation of the VD. The entire examination was videorecorded (see Supplementary Video 1; Supplementary Data are available online at
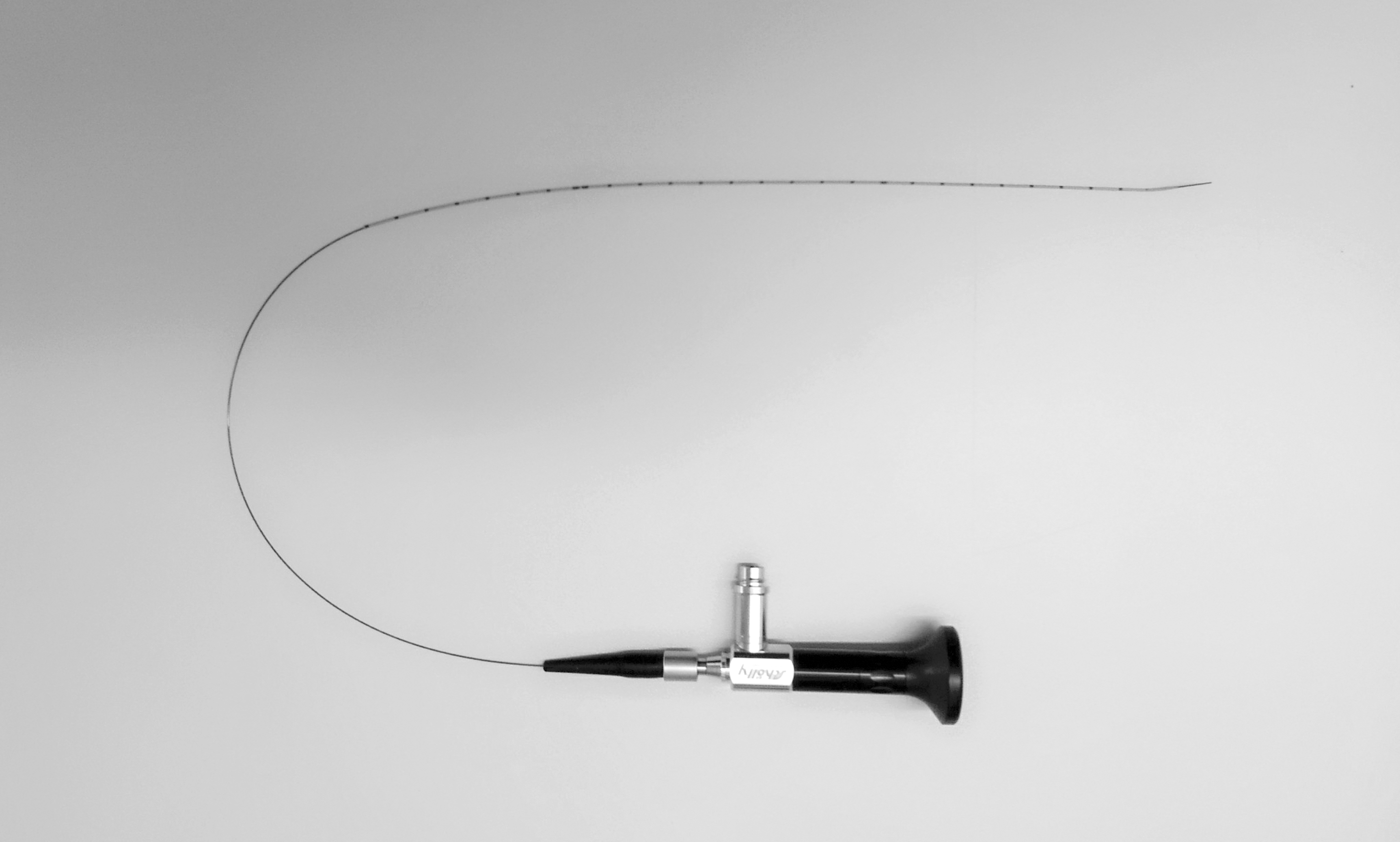
Miniaturized flexible endoscope 0.35 mm (1.05F) with ureteral catheter (5F). Working length 500 mm and optical resolution 3,000 pixels.
Results
Routine urethroscopy revealed no signs of urethral pathology. The ejaculatory duct's opening was not initially visible during conventional urethroscopy of the prostatic urethra. The orifice of the ejaculatory ducts could not be identified until methylene blue had been injected into the VD. The seminal tract's anatomical location was lateral to the seminal colliculus flanking the prostatic utricle. Its opening into the urethra was lined by two longitudinal lip-shaped structures. After methylene blue was injected into the proximal deferent duct via the high scrotal access, these structures opened, releasing the fluid into the urethra. Intubation of the ejaculatory ducts with the hydrophilic guidewire was only possible once we had visualized the orifice.
Before that, an initial attempt to microoptically visualize the deferent duct was made anterograde from the high scrotal approach. Irrigation with physiological saline was necessary to dilate the duct and advance the endoscope atraumatically. Extensive long-segment anterograde inspection into the VD was hampered by tissue adhesions, most probably because of postmortal alterations in the cadaver model. Image quality was sufficient for identifying the anatomical structures and for the endoluminal characterization of tissue properties, although image resolution was restricted to 3000 pixels.
After antegrade visualization of the deferent duct, methylene blue was injected, and the orifice of the ejaculatory duct into the urethra was retrogradely intubated cystoscopically. Following intubation with a ureteral catheter, the microoptical endoscopy system was advanced into the ejaculatory duct (Fig. 2). We were able to differentiate the ejaculatory duct, the intersection with the seminal vesicles, and transition into the deferent duct. We observed no iatrogenic tissue lesions while retracting the microoptic fiber. In the last step, we intubated the prostatic utricle using a semirigid ureterorenoscope. Inspection revealed a blind-ending saccule, not leading to any other anatomical structure. No physiological connection to the ejaculatory duct could be identified. Access to the ejaculatory ducts and seminal vesicles was only possible by blunt forced penetration of the prostatic utricle's lateral wall (Fig. 3).
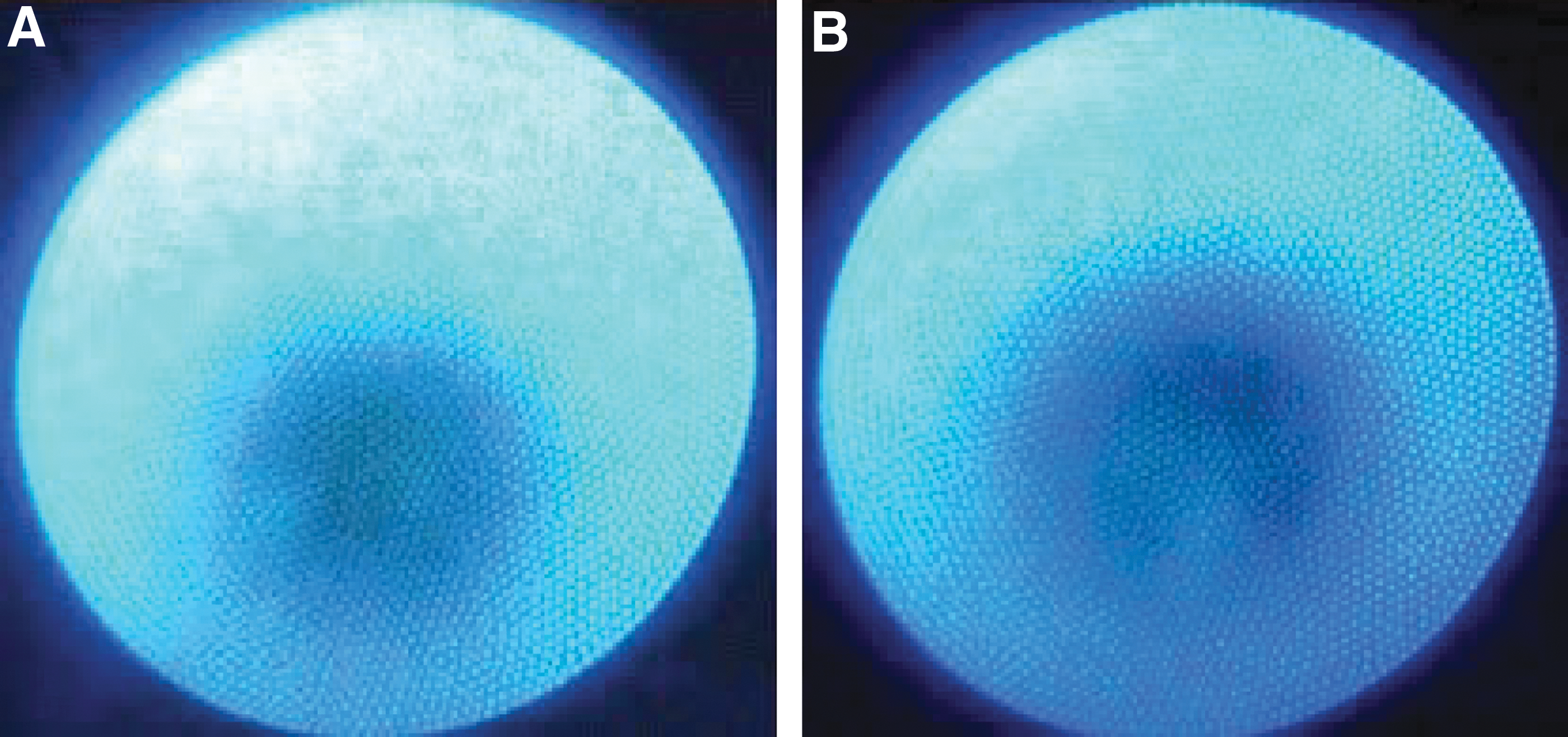

Intraluminal frame sequences using the ureteroscope.
Discussion
To the best of our knowledge, this is the first endoscopic characterization of the seminal tract using a specialized miniaturized flexible optical system. Since the first in vivo reported endoscopy of the distal seminal tract in 2002, 11 several studies have been published focusing on transurethral seminal vesiculoscopy for diagnosis and treatment purposes targeting ejaculatory duct obstruction and recurrent hematospermia. 1,4,6 –8 Although their results appear encouraging, transurethral seminal vesiculoscopy has not become established in the clinical routine so far for reasons that are multifactorial. The male internal genitourinary tract's complex anatomy makes accessing the ejaculatory duct challenging and potentially harmful to the patient. The latest endourologic instruments, for example, various cystoscopes und ureteroscopes, seem particularly unsuitable for this application. Nevertheless, common cystoscopic or ureteroscopic equipment was used in most of the published studies: forced blind insertion of the endoscope through the prostatic utricle or exposure of the ejaculatory ducts after transurethral resection of the seminal colliculus has been reported. 1,5,9,11 This access strategy carries the high risk of iatrogenic injury to the surrounding tissue resulting in scarring and raises the risk of secondary ejaculatory duct occlusion, followed by azoospermia or persistent hematospermia. Hence, a physiological approach via the ejaculatory duct's orifice would minimize intervention-associated complications and make this access preferable as the standard endoscopic approach. We used a microoptical system in this investigation to take an atraumatic retrograde approach through the physiological opening of the ejaculatory duct. Interestingly, since its dorsolateral location is so difficult to discern, the orifice could only be visualized after a methylene blue injection, that is also what made retrograde intubation so initially challenging.
Insertion of the instrument via the Seldinger technique was only possible by making use of a hydrophilic guidewire. This may be because the lip-shaped structures lining the orifice seal the ducts, physiologically functioning as a valve mechanism. This complex valve mechanism prevents the duct from opening adequately when the verumontanum is relaxed, thereby causing the ejaculatory ducts to collapse. Physiologically, this mechanism prevents urine from leaking into the ejaculatory ducts during micturition and seals the urethra during ejaculation to prevent retrograde ejaculation. 12 Furthermore, the absence of endothelial turgor and the cadaver's considerable postmortal rigor (resulting in greater tissue rigidity) most likely additionally hampered the intubation of the ejaculatory structures. In vivo experiments may not be compromised by such conditions; atraumatic access may be facilitated, and the valve mechanism overcomes simply due to the surrounding structures' increased elasticity.
Once these limitations are overcome, an atraumatic approach may also offer new diagnostic options for common seminal pathologies. Current clinical routine imaging options for diagnosing seminal tract diseases, including common ultrasound and TRUS, 14 have proven to be insufficient in terms of spatial resolution or functional contrast and thus not able to yield reliable information since by their nature ultrasound modalities rely on indirect findings. 10 CT and especially MRI are increasingly used for prostate and testicular imaging. Nevertheless, the lack of sufficient resolution may be the key debilitating factor for diagnostic work-up in male infertility and hematospermia. With the latest advances in endoscopy and optical imaging technologies, such as miniaturized flexible microoptical devices and digital video processing, the atraumatic inspection of the seminal tract might come significantly closer to being clinically implemented. Endoscopy of the internal male genital system would therefore gain importance as an effective and reliable tool for direct on-site diagnostics and therapy. Nevertheless, using an atraumatic tool for FVV may also cause other clinical complications. Retrograde vasoscopy may possibly increase the risk for serious iatrogenic infection of the male adnexa. Hence, an additional antibiotic treatment must possibly be discussed, preventing prostatitis, epididymitis, or even sepsis. Furthermore, also atraumatic retrograde endoscopy may result in intraoperative lesions with consecutive secondary scarring maximizing trauma to the seminal tract. Having in mind the possible clinical challenges, we strongly believe that this new technology offers an overall benefit for patients with conceivable new applications in endosurgical therapy in andrology, for example, obstructive azoospermia therapy by laser tissue vaporization and hematospermia diagnosed and treated via direct endoscopic modalities. 5,9 With the atraumatic benefits associated with microoptic fibers, vasoscopy might eventually enable us to obtain histological probes from the seminal duct for pathological or microbiological investigation. Moreover, selective embolism of the VD during vasoscopy may become an alternative treatment strategy for male fertility control, competing with conventional surgical vasectomy. Using a removable plug or novel intelligent materials, even reversible endoocclusion of the VD is imaginable. 15 –17 However, translating this new technology to clinical routine depends strongly on its clinical implications, handling, and affordability. Our experimental setup is focusing on an atraumatic access to the human ejaculatory duct offering a sufficient image quality. This study is limited by its design since the experiments were performed on a single cadaver model. Although no premortal urogenital interventions had been reported, potential postmortal changes in the genitourinary tract anatomy and morphology, that is, tissue adhesion and rigor, as well as technical limitations in system maneuverability, may have compromised our results substantially. Further technical developments, and especially in vivo clinical tests of feasibility, and functional characterization of the above-described system are therefore required.
Conclusions
The initial results of atraumatic microoptical flexible endoscopy of the male seminal tract in a cadaver model are encouraging. Image quality and spatial resolution are sufficient for routine clinical use. Nevertheless, complex anatomical and technical limitations reveal the need for further refinements of this concept for routine clinical implementation. Moreover, in vivo examinations still need to be conducted. The presented technique might contribute to the improvement of diagnostics and the treatment of different genitourinary diseases in the future.
Footnotes
Acknowledgments
We would like to thank Schölly Fiberoptic GmbH (Denzlingen, Germany) for providing the instruments and technical support for this study. The cadaver (body donor) has been provided by the Institute for Anatomy, Medical Faculty, Justus-Liebig-University (Giessen, Germany).
Authors' Contributions
D.S.: data analysis and article writing/editing. M.M.: data collection, data analysis, and article editing. S.H.: article editing and figure editing. F.A.: article editing. M.S.: article editing. T.D.: protocol/project development and article editing. W.W.: protocol/project development and article editing. A.M.: protocol/project development, data collection, data analysis, article writing/editing, and supervision.
Author Disclosure Statement
M.S.: consultant contract with Schöelly Fiberoptic GmbH (Denzlingen, Germany) and NeoTract, Inc. (Pleasanton, CA). T.D.: Lilly Deutschland GmbH (stocks/stock options, employee: via family member), Pfizer (speaker honorarium), Takeda Pharma GmbH (speaker honorarium), AMS Deutschland (speaker honorarium), Jenapharm GmbH (speaker honorarium), Glenwood (speaker honorarium), Cheplapharm Arzneimittel GmbH (consultant), Marpinion GmbH (advisory board member and consultant), Advance Medical S.A., Barcelona (ESP) (consultant and reviewer). A.M.: consultant contract with Schöelly Fiberoptic GmbH (Denzlingen, Germany). All other authors declare that no competing financial interests exist.
Ethical Standard
The study design was approved by the Institutional Ethics Committee of the University of Freiburg Germany (296/13) and performed in accordance with the ethical standards defined by the Declaration of Helsinki. Leading ethics committee: Ethics Commission of Albert-Ludwigs University Freiburg.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.