
Abstract
Introduction:
Triple D score was recently developed for prediction of extracorporeal shockwave lithotripsy (SWL) outcomes. However, it has not been validated. SWL in elderly patients results in lower success and higher complication rates. We aimed at externally validating Triple D score in a population ≥65 years of age.
Patients and Methods:
We retrospectively analyzed the data of 182 patients ≥65 years of age who underwent SWL for renal or ureteral stones and were evaluated with non-contrast computed tomography before SWL. Stone volume (SV), skin-to-stone distance (SSD), and stone density were measured, and cutoff values were determined with receiver operator characteristic analysis. Triple D scores were calculated, and success rates were determined for each score.
Results:
Mean SV, SSD, and stone density values were significantly higher in patients with failed outcomes compared with those with successful outcomes in both renal and ureteral cases. Cutoff values of 187.5 mm3, 10.5 cm, and 675 HU for renal stones and of 185 mm3, 11.5 cm, and 785 HU for ureteral stones were detected. Success rates of 95.5% and 95% were detected for patients with a Triple D score of 3 in the renal and ureteral stone groups, respectively. Success rates of patients with a Triple D score of 0 were 20% and 25% in the renal and ureteral stone groups, respectively.
Conclusions:
Triple D score correlated well with SWL outcomes in patients ≥65 years of age, and it is externally validated. Various factors may deal with cutoff levels of involved parameters. Therefore, we suggest that each institution determines its unique cutoff levels for SV, SSD, and stone density parameters and calculates the Triple D score for its patients with respect to these cutoff levels to predict the success after SWL and aid in decision making.
Introduction
E
Highly variable treatment outcomes have been suggested to be possible reasons for the decreasing interest in SWL (32%–90% for renal stones). 5 Besides technical problems and variations in reporting of outcomes, inappropriate patient selection is one of the most prominent reasons for this diversity in success rates. Prediction of SWL outcomes with clinical parameters and information from non-contrast enhanced computed tomography (NCCT) has been of interest in a number of studies, 6 –10 and nomograms have also been developed for this particular purpose. 11 –13 Recently, Tran et al. described a simple scoring system “Triple D” by evaluating the stone volume (SV), skin-to-stone distance (SSD), and stone density from NCCT studies and concluded that this scoring system may increase the success rates of SWL. 14 The main advantage of Triple D score is that it can be involved in routine radiology reports and does not need complex calculations. However, Triple D score is not yet externally validated.
Increasing age has been shown to be negatively correlated with SWL outcomes in renal stone patients. 15,16 Additionally, risk of complications after SWL has been shown to be higher in the elderly population. 17 Therefore, proper patient selection for SWL is of utmost importance in patients with advanced age to establish higher treatment success with avoidance of complications, and the current literature lacks nomograms or scoring systems that are developed for this population. Triple D score can be a candidate to fill this gap, and the objective of this study was to perform external validation of Triple D score in a patient population ≥65 years of age with renal and ureteral stones separately.
Patients and Methods
Data of 216 consecutive patients ≥65 years of age and who underwent SWL for stones ≥5 mm between January 2009 and January 2016 in our department were evaluated retrospectively. From this cohort, 25 patients without an NCCT evaluation before SWL and 9 patients who were lost to follow-up were excluded, and the data of 182 patients were evaluated.
All of the patients were evaluated with NCCT before the SWL procedure; all of the scans were evaluated; and desired parameters were determined by a single radiologist (B.G.) who was specialized in urinary system imaging and blinded to the SWL outcomes. Imaging after SWL was performed with an abdominal X-ray and/or urinary system ultrasonography in all patients, and NCCT was performed in 128 (70.3%) patients depending on the preferences of the consulting physician. Success was defined as stone-free status or residual fragments <4 mm. According to our institutional policy, all patients underwent a maximum of three sessions of SWL with at least 1 week apart between each session, and the efficacy of SWL was evaluated at least 1 week after each session. The recorded imaging to evaluate success of the procedure was done at least 12 weeks after the last session of SWL in case of unsuccessful outcomes in the early imaging after SWL.
Age, gender, stone laterality, and stone location were recorded. The parameters recorded from the NCCT were ellipsoid SV, SSD, and stone density, and they were measured through HU. SV was calculated by applying the formula: SV = π/6 × (Anteroposterior × Transverse × Cranio-caudal diameters of the stone in mm), and it was represented as mm3. SSD was calculated as described by Pareek et al. 8 Triple D score was calculated as described by Tran et al. 14
SWL technique
SWL was performed with the ELMED Multimed Classic lithotripter (ELMED, Ankara, Turkey) electrohydraulic system in the supine position. The SWL procedure began with an initial voltage of 7 kV energy level, and power ramping was applied to increase it to the level of 21 kV. Shockwave frequency of 60- to -90 waves per minute was used, and 2500– to -3000 shockwaves were applied in each SWL session.
Statistical analysis
Statistical analysis was performed with IBM SPSS Statistics for Windows, Version 20.0. (IBM Corp., Armonk, NY). Descriptive statistics for the parameters were provided for the entire cohort. Continuous variables were reported as mean and SD, and categorical variables were reported as percentages. Student's t-test or Mann–Whitney U test was used for the comparison of the continuous variables, and Chi-Square test or Fisher's exact test was used for the comparison of the categorical variables in the renal and ureteral stone patient groups with respect to SWL success. Receiver operator characteristic (ROC) curves were generated to determine cutoff values for the SV, SSD, and stone density and area under the curve (AUC) values for each parameter were provided. Patients were scored with respect to these cutoff values. A further comparison of the Triple D score groups for success rates was performed with the Chi-Square test.
Results
The mean age of the population was 69.7 ± 4.9 years; 126 (69.2%) of the patients were men, and 56 (30.8%) of the patients were women. Mean SV, SSD, and stone density values of the entire population were 198 ± 80 mm3, 11.2 ± 1.1 cm, and 669 ± 223 HU, respectively. Treatment success was established in 130 of the 182 (71.4%) patients after as much as three SWL sessions, and success rate after the first SWL session was 53.3%. SWL was performed in 133 (73.1%) patients and 49 (26.9%) patients for renal and ureteral stones, respectively.
Characteristics of the renal and ureteral stone patients with respect to treatment success is summarized in Table 1. Age, gender, stone laterality, number of SWL sessions, and presence of ureteral stents were found to be similar for patients with successful and unsuccessful outcomes in both renal and ureteral stone cases. Mean SV, SSD, and stone density values were found to be significantly higher in patients with unsuccessful outcomes compared with the patients with successful outcomes in both renal and ureteral stone cases (all p < 0.001). Stone location was also shown to be significantly different in renal stone patients, with a higher incidence of lower pole stones in patients with an unsuccessful outcome (15.2% vs 31.7%, p = 0.02), but the distribution of stones through ureteral segments did not show a significant difference in the ureteral stone cases (p = 0.8).
Comparison was performed with independent samples median test.
SSD = stone-to-skin distance; SWL = extracorporeal shockwave lithotripsy.
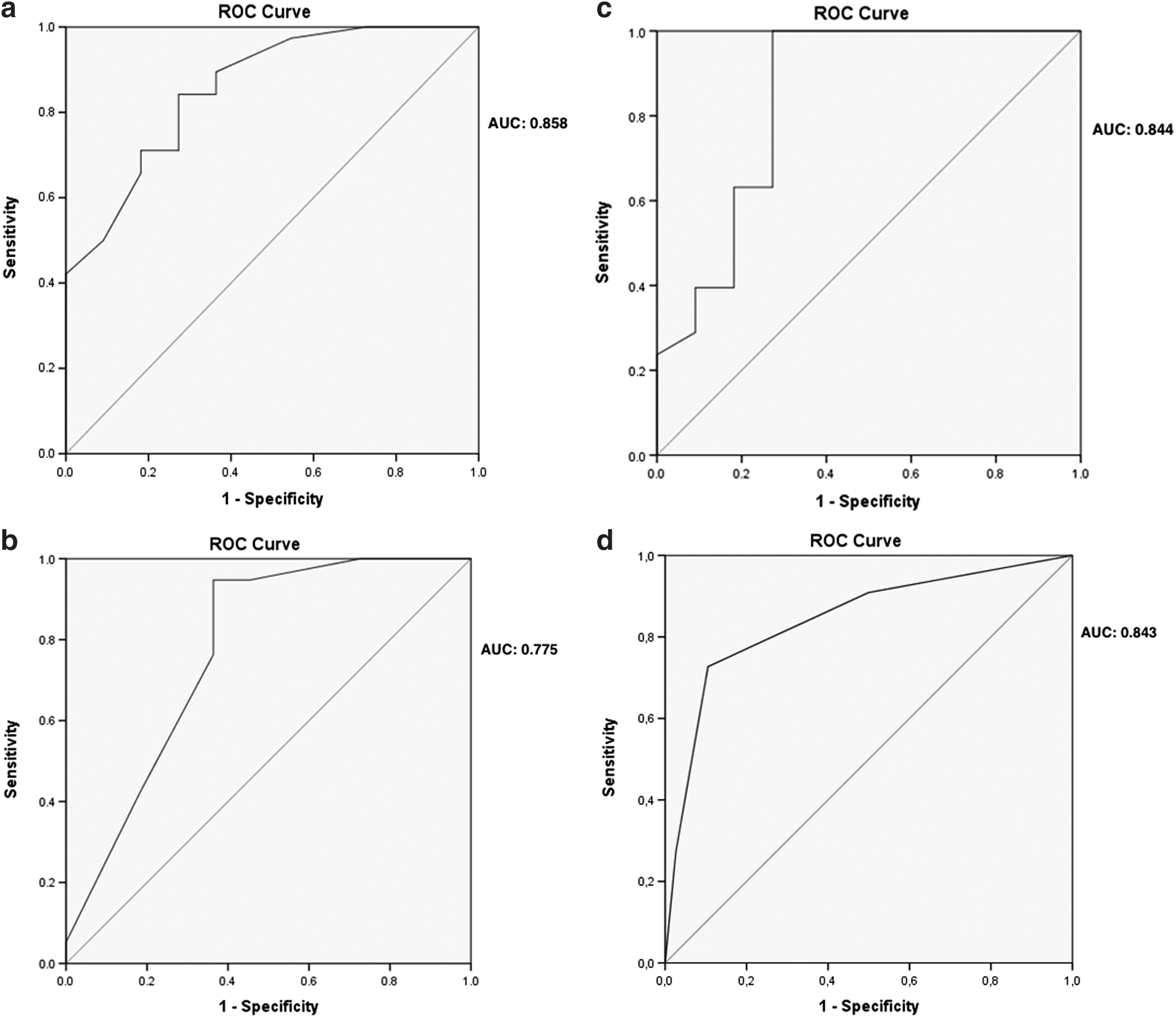
ROC curves were generated for SV, SSD, and stone density parameters for the renal and ureteral stone cases separately, and cutoff points were determined with respect to the greatest sensitivity and specificity values. Significant AUC values were detected for all of the parameters in both renal and ureteral cases. AUC values of the Triple D sore were 0.854 and 0.843 for the renal and ureteral stone cases, respectively. The AUC value of the Triple D score was higher than the AUC values of each of the SV, SSD, and stone density parameters for the renal stone cases. The results of AUC and cutoff levels with sensitivity and specificity values are summarized in Table 2, and ROC curves are given for renal and ureteral stone cases in Figures 1a–d and 2a–d, respectively.

ROC curves for the SV, SSD, and stone density in kidney stone patients.
ROC curves for the SV, SSD, and stone density in ureteral stone patients.
AUC = area under the curve; HU = Hounsfield Unit.
Patients were grouped with respect to the defined cutoff values, and Triple D scores were calculated. Success rates of the Triple D score groups were compared for the renal and ureteral stone patients separately. Triple D score was found to show a good correlation with success rates, and 95.5% and 95% of the patients with a Triple D score of 3 were found to have successful outcomes in the renal and ureteral stone groups, respectively. On the other hand, the success rates of patients with a Triple D score of 0 were 20% and 25% in the renal and ureteral stone groups, respectively. The results are summarized in Table 3. A separate analysis was performed by using the cutoff values defined by Tran et al. 14 to compare the success rates of the Triple D score groups. This analysis would be valuable, as some institutions may not have the chance to define their own cutoff values. A good correlation between the Triple D score and success rates was detected for both renal and ureteral stone cases, although the level of correlation diminished somehow compared with results established with the cutoff values in the current study. The success rates of the groups according to the cutoff values defined by Tran et al. 14 for renal and ureteral stone cases are summarized in Table 4.
Besides success rates, the number of SWL sessions to establish success is also an important parameter. In both the renal and ureteral stone cases, the median numbers of SWL sessions to reach success were 1, 1, 2, and 2 for the Triple D scores of 3, 2, 1, and 0, respectively (p = 0.12). In this elderly population, after SWL treatment, perirenal hematoma was observed in two (1%) cases, both of whom were managed conservatively without need for transfusion or any intervention. Ureteral stenting was needed in 10 (5.5%) patients, and urinary tract infections requiring antibiotic treatment were observed in 3 (1.6%) cases.
Discussion
Recently, Triple D score was described by Tran et al. to predict the stone-free rates of SWL procedures and to enhance cost-effectiveness. 14 The main advantage of the Triple D score is that it is easy to calculate and can be placed in routine radiology reports to aid clinicians in the decision-making process of treatment of renal and ureteral stones. In the present study, we aimed at externally validating the Triple D score in an elderly population, and our results suggest that it is effective in the prediction of successful SWL outcomes in both renal and ureteral stones in this particular population.
Several parameters have been identified to predict the success rates of the SWL procedures. 15,18 These factors can be listed as stone composition, stone density, stone size, calix anatomy, patients' body habitus, and body mass index. Most of these parameters can be evaluated with NCCT studies and nomograms to predict SWL outcomes that have been developed by several groups. 11 –13 However, these nomograms are not widely accepted and routinely used, although they provide valuable information. A possible explanation for this situation is that clinicians do not spare time to put their patients' information on these nomograms. Triple D score combines three parameters that can be easily obtained from NCCT studies and are involved in routine radiology reports. Although we did not perform any time recordings during the study for establishing the Triple D score, it was observed that it takes about 5 extra minutes to make the necessary measurements on the NCCT images. Therefore, it has the potential to be included in routine radiology reports and is used in daily practice.
In their study, Tran et al. evaluated the significance of the SV, SSD, and stone density with ROC curves and the corresponding AUC values were 0.7745, 0.6224, and 0.7752, respectively. 14 In our study, we also established the ROC curves for each parameter in the renal and ureteral stone cases separately, and each parameter was shown to have a significant correlation with success rates. Tran et al. detected an overall 57.1% stone-free rate, and this rate is lower than the success rate of 73.1% in our study. This difference may be related to the definition of success (we accepted residual fragments <4 mm as successful outcomes), and we also reported success after three consecutive sessions of SWL, instead of a single session, which was the case in the study of Tran et al. 14 Additionally, stone location showed some difference between the two studies. The rate of lower pole stones among the renal stone cases was 20.3% in our study, and this was lower than the rate of 56.3% in the study of Tran et al. This difference possibly resulted from our institutional policy on patient selection for SWL, that we prefer endourology procedures in case of a lower pole stone with a steep infundibulum-pelvis angle.
Stone size has been shown to be inversely correlated with SWL success rates and for evaluation of stone size, the longest diameter, stone surface area, or SV can be used. SV was shown to be a better predictor of stone-free rates compared with axial stone diameter in a multivariate model. 19 However in this study, SV was estimated by a special software and this limits the generalized application of the method. To overcome this, Tran et al. calculated the SV by a formula including the three different axial measurements and SV was found to be a significant predictor of stone-free status after SWL. The cutoff value for SV was found to be 150 mm3, which is somehow lower compared with our cutoff values of 187.5 and 185 mm3 for the renal and ureteral stones, respectively. 14 The difference can be attributed to the number of SWL sessions and the definition of success.
SSD was first evaluated as a predictor of successful SWL by Pareek et al. In their study, the authors found that the mean SSD value was significantly higher in patients with a failed SWL (11.5 cm) compared with those with a successful outcome (8.12 cm). They also identified SSD as an independent predictor of SWL outcome in logistic regression analysis. 8 Later on in another study, Perks et al. also evaluated the role of SSD together with stone attenuation to define risk groups for failed SWL and they identified SSD <9 cm as a factor that was associated with SWL success. 20 Patel et al. compared SSD values in patients with failed and successful SWL outcomes and identified SSD as an independent predictor of stone-free status after a single session of SWL. 9 Wiesenthal et al. also analyzed SSD to find out a cutoff value for the prediction of success, which was described as residual fragments ≤4 mm. The authors reported a cutoff level of 11 cm. 21 This cutoff value was lower than the 12 cm cutoff value identified by Tran et al., 14 but it was in between our cutoff values of 10.5 and 11.5 cm for renal and ureteral stones, respectively. From the results of all of the studies mentioned earlier, SSD is identified as an important parameter for the prediction of success after SWL. However, there are differences with respect to cutoff levels that may be attributed to differences in SWL device and technique, the definition of success, and the number of applied SWL sessions.
Stone density evaluation through measurement of HU in NCCT studies has been the subject of a number of studies, and some of these studies proposed cutoff values. 7,14,21,22 Wang et al. compared the stone density levels of patients with failed and successful SWL outcomes and found a significant difference (809 HU vs 654 HU, p = 0.02). They also performed ROC curves, and the AUC for stone density was 0.768. The proposed cutoff value was 900 HU, with a sensitivity of 0.763 and a specificity of 0.667. 22 Similarly, Wiesenthal et al. also proposed the cutoff level of 900 HU for the prediction of success after SWL. The authors did not perform an ROC analysis but compared the mean stone density levels of failed and successful cases and detected a significant difference (862 HU vs 766 HU, p = 0.02). A cutoff value of 900 HU resulted in an adjusted odds ratio of 0.49 (95% CI 0.33, 0.75). 21 In a more recent study, Ouzaid et al. prospectively enrolled patients to detect the effect of stone density on SWL success that was defined as the presence of residual fragments <4 mm. A cutoff value of 970 HU with a sensitivity of 100% and a specificity of 81% was detected. Also, an AUC of 0.94 was established in the ROC curve (0.94). 7 Tran et al. identified stone density as the most prominent parameter to determine stone-free status among all parameters included in the Triple D score with an AUC of 0.7749. The defined cutoff value was 600 HU, which was lower compared with cutoff levels in the previous studies. 14 In our study, the cutoff levels of stone density for renal and ureteral stones were 675 and 785 HU, respectively. These cutoff levels are higher than the level identified by Tran et al., 14 but they are still lower than those in the previous studies. 7,21,22
Patient age has been identified as an important parameter for success and complication rates of the SWL procedures. 15 –17 Abdel-Khalek et al. attempted to define factors associated with successful SWL outcomes and identified older patient age as a predictor of failure. Similarly, Ng et al. evaluated the effect of age on SWL outcomes in a multivariable model. Patient's age >60 years was found to have 0.643 (0.506–0.818; p < 0.001) odds of having stone-free status compared with age ≤40 in renal stone cases. 16 Safety of SWL is another important issue, and sub-capsular hematoma is one of the most important complications of SWL. Dhar et al. reported a 4.1% rate of sub-capsular hematoma in their series, and the probability of hematoma was estimated to be 1.67 times greater for each 10-year incremental group in patient age. 17 Taking into account the effect of patient age on SWL outcomes, we believe that appropriate patient selection is quite important for the elderly population; therefore, we aimed at validating the Triple D score in this particular population, and the outcomes were remarkable.
Tran et al. reported stone-free rates of 96.1%, 78.7%, 41.3%, and 21.4% for Triple D scores of 3, 2, 1, and 0, respectively. 14 Our results for the success rates of 95.5%, 85.4%, 36.4%, and 20% for the renal stone cases and of 95%, 88.2%, 37.5%, and 25% for the corresponding Triple D scores were quite similar to the results of Tran et al. The Triple D score was able to predict the success rates in this independent cohort. In our study, AUC values of the Triple D score were found to be 0.854 and 0.843 for the renal and ureteral stone cases, respectively, and these values were slightly higher than the AUC value of 0.784 in the study by Tran et al. 14 Therefore, we believe that the Triple D score is externally validated, can be used for the prediction of success rates of SWL, and can aid in appropriate patient selection with its advantage of being convenient. However, each center should define its cutoff levels for the involved parameters, as they would depend on the SWL device, SWL technique (shockwave frequency, power ramping, coupling method, etc.), and the definition of success. These cutoffs may be shared with the radiology departments to provide scores in the routine radiology reports to be used in daily practice.
The choice of treatment in the elderly population is determined not only by the success rates of the treatment alternatives but also with other patient-related parameters such as patient preferences, comorbidities, and convenience with general anesthesia. Therefore, SWL would be the choice of treatment for certain patients despite their having a Triple D score of 0 or 1. However, even in these cases, the Triple D score may benefit in informing the patients that the success rates would be low and they would need multiple treatment sessions.
The most important drawback of our study is that the cohort does not exactly match the cohort of the original study for the SWL technique, patient age, number of SWL sessions, and the definition of success. However, this would be the case for every nomogram or scoring system that is used to predict SWL outcomes. Also, the number of patients with ureteral stones was quite low compared with the renal stone cases but still, it was possible to establish significant AUC and cutoff values. Advanced age was shown to be associated with a delay in clearance of residual fragments. 23 We evaluated the success rates 12 weeks after the last session in case of failed SWL in the early imaging, and this time interval would be insufficient for expulsion of residual fragments in the elderly population.
Conclusions
Triple D score correlated well with SWL outcomes for both ureteral and renal stones in a population of patients ≥65 years of age, and it is externally validated. SWL device, technique, patient selection criteria, and the definition of success may vary between institutions. Therefore, we suggest that each institution determines its unique cutoff levels for SV, SSD, and stone density parameters and calculates the Triple D score for its patients with respect to these cutoff levels to predict the success after SWL and aid in decision making.
Footnotes
Author Disclosure Statement
No competing financial interests exist.