
Abstract
Purpose:
Scoring systems have been devised to predict outcomes of percutaneous nephrolithotomy (PCNL). CROES nephrolithometry nomogram (CNN) is the latest tool devised to predict stone-free rate (SFR). We aim to compare predictive accuracy of CNN against Guy stone score (GSS) for SFR and postoperative outcomes.
Materials and Methods:
Between January 2013 and December 2015, 313 patients undergoing PCNL were analyzed for predictive accuracy of GSS, CNN, and stone burden (SB) for SFR, complications, operation time (OT), and length of hospitalization (LOH). We further stratified patients into risk groups based on CNN and GSS.
Results:
Mean ± standard deviation (SD) SB was 298.8 ± 235.75 mm2. SB, GSS, and CNN (area under curve [AUC]: 0.662, 0.660, 0.673) were found to be predictors of SFR. However, predictability for complications was not as good (AUC: SB 0.583, GSS 0.554, CNN 0.580). Single implicated calix (Adj. OR 3.644; p = 0.027), absence of staghorn calculus (Adj. OR 3.091; p = 0.044), single stone (Adj. OR 3.855; p = 0.002), and single puncture (Adj. OR 2.309; p = 0.048) significantly predicted SFR on multivariate analysis. Charlson comorbidity index (CCI; p = 0.020) and staghorn calculus (p = 0.002) were independent predictors for complications on linear regression. SB and GSS independently predicted OT on multivariate analysis. SB and complications significantly predicted LOH, while GSS and CNN did not predict LOH. CNN offered better risk stratification for residual stones than GSS.
Conclusion:
CNN and GSS have good preoperative predictive accuracy for SFR. Number of implicated calices may affect SFR, and CCI affects complications. Studies should incorporate these factors in scoring systems and assess if predictability of PCNL outcomes improves.
Introduction
P
Materials and Methods
This was a hospital-based analysis of patients undergoing PCNL between January 2013 and December 2015 from a tertiary care referral urological center in South India performing around 150 to 160 PCNL per year. Institutional review board approval was obtained. Only those patients evaluated with preoperative CT scan and X-ray film of kidney–ureter–bladder (XRKUB) and postoperative XRKUB and ultrasound KUB for clearance were included. Patients with recurrent ipsilateral stones were included. Patients <18 years, those with preoperative ipsilateral nephrostomy or stent placement, nonradiopaque stones, second look PCNL, simultaneous bilateral PCNL, and patients with incomplete data were excluded. SB was calculated by the following formula: 0.25 × π × lengthmax × widthmax.
10
Estimated case volume per year was calculated as follows: reported cases/reported inclusion period (days) × 365 days.
11
SFR was defined as absence of any residual stone >4 mm on XRKUB and renal ultrasound.
7
Based on our institute's protocol, SFR was evaluated before the patients were discharged after PCNL. Complications encountered were recorded and classified according to the modified Clavien System for urologic patients.
12,13
Only the complication of the highest grade was analyzed. GSS, CNN scores (Supplementary Table S1; Supplementary Data are available online at
Perioperative data
Data collected included demographic data (age, comorbidities), past surgical history, stone characteristics (size, location, stone count, staghorn, implicated calices, HU, SB), intraoperative data (supracostal/infracostal entry, calices punctured, number of access tracts, tract size, operation time [OT], postoperative drainage), and postoperative outcomes (complications, blood transfusion, residual stone status, and length of hospitalization [LOH]).
Surgical technique
The procedure was performed under general anesthesia. In the lithotomy position, an open-ended 5F/70 cm ureteral catheter was placed on the side of stone through rigid cystoscope (Karl Storz Endoscopy, Tuttlingen, Germany). Patient was placed prone, and retrograde pyelography was performed. Using the bull's eye technique, appropriate calix was punctured with an 18-gauge/15 cm diamond-shaped trocar needle under fluoroscopy. A 0.032" hydrophilic guidewire was inserted, and tract dilation was done as much as the desired size. The maximum tract size was as much as 30F, and a 22F or 26F nephroscope (Karl Storz Endoscopy) was used. Lithotripsy was done by pneumatic lithotripter (Nidhi Lith Digi; Nidhi Meditech Systems, India). Postoperative drainage was based on intraoperative factors and surgeon choice.
Outcomes
The primary outcomes analyzed were predictive accuracy of GSS, CNN, and SB for SFR. The secondary outcomes assessed were predictive accuracy of these parameters for modified Clavien complications, OT and LOH. We further stratified patients into risk groups based on the CNN and the GSS for their clinical applicability and intended to identify other preoperative risk factors that could affect outcomes.
Statistical analysis
Data were tabulated, and statistical analysis was performed using SPSS version 20 (IBM Corp., Armonk, NY). Continuous variables were depicted as mean with standard deviation (SD), and categoric variables as median and interquartile range (IQR). Student's t-test (two tailed, independent) was used for metric parameters on continuous scale between two groups. Chi-square and Fisher's exact test were used to compare parameters on categoric scale between two or more groups. Binomial logistic regression analysis was used to identify independent predictors for postoperative SFR and complications. Linear regression analysis was used to identify the predictors of OT and LOH. A p-value of <0.05 was considered statistically significant. The CNN was divided in quartiles for categorization in risk groups. The area under curve (AUC) calculated by receiver operating characteristic (ROC) curve analysis was used to predict the SFR and complications for GSS, CNN, and SB.
Results
We enrolled 313 patients in our study. The mean ± SD age was 44.8 ± 13.6 years, and 204 (65.2%) were males. The mean ± SD SB was 298.8 ± 235.75 mm2, and mean ± SD stone radiodensity was 1022.4 ± 254.4 HU. Staghorn calculus was seen in 66 (21.2%) patients, and single stone was found in 149 (47.9%) patients. Majority of the PCNL was performed through a single puncture (278; 88.8%) and mostly through the inferior posterior calix (141; 45%). The mean SFR was 76%. The mean ± SD length of hospitalization (LOH) was 4.7 ± 3.1 days. Complications occurred in 84 (26.8%) patients with Clavien grade I in 18.2% patients. The mean ± SD CNN score was 251.3 ± 57.1. The median (IQR) GSS was 2 (2).
Predictors of SFR
On univariate analysis, the number of stones (p < 0.001), number of implicated calices (p = 0.032), stone location (p = 0.002), staghorn stones (p < 0.001), SB (p < 0.001), GSS (p = 0.001), CNN (p < 0.001), and number of punctures (p = 0.001) were found to be significantly associated with SFR. Past surgical history, a component of CNN, was incapable of predicting SFR in our population. SFR based on GSS and CNN is depicted in Table 2. SFR decreased with increasing GSS category and decreasing CNN values (Table 2). On multivariate analysis, single implicated calix (Adj. OR 3.644), absence of staghorn (Adj. OR 3.091), single stone (Adj. OR 3.855), and single puncture (Adj. OR 2.309) were significant predictors of SFR (Table 1). Based on ROC analysis, SB (AUC: 0.662), GSS (AUC: 0.660), and CNN (AUC: 0.673) were found to predict SFR similar to each other (Fig. 1A).
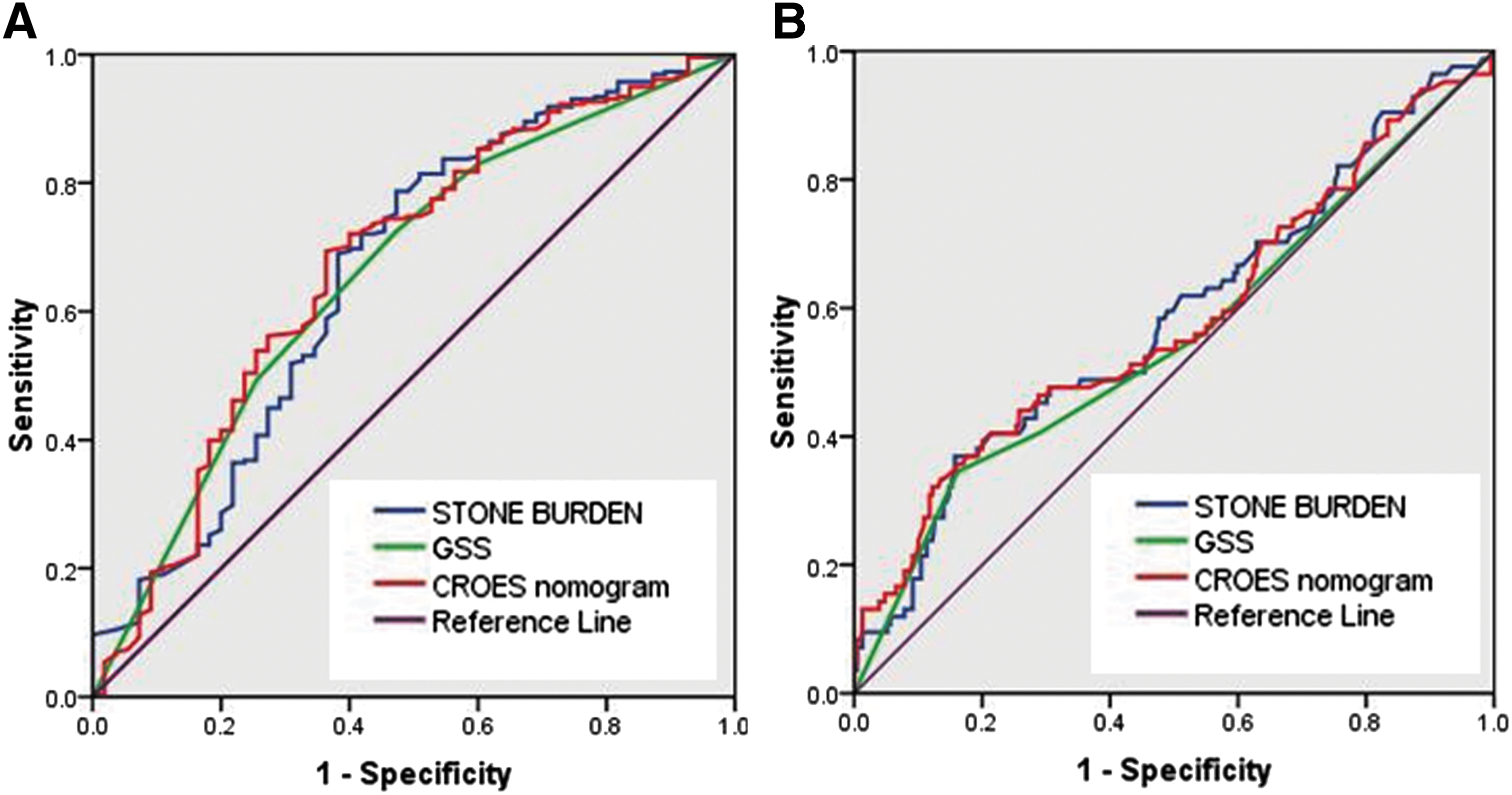
ROC curves.
Bold values indicate significant p value (p < 0.05).
Reference category.
CI = confidence interval; GSS = Guy stone score.
Predictors of complications
On univariate analysis, Charlson comorbidity index (CCI; p = 0.027), staghorn stones (p < 0.001), SB (p = 0.024), GSS (p = 0.002), and CNN (p = 0.047) were found to be significantly associated with complications. On multivariate logistic regression analysis, presence of staghorn calculus (Adj. OR 2.539, 95% CI: 1.389, 4.639; p = 0.002) and CCI (Adj. OR 2.074, 95% CI: 1.124, 3.824; p = 0.020) was found to be a significant predictor of complications. Based on ROC analysis, SB (AUC: 0.583), GSS (AUC: 0.554), and CNN (AUC: 0.580) were found to have poor predictability for complications (Fig. 1B).
OT and LOH
On univariate analysis, presence of staghorn calculus (p < 0.001), multiple stones (p = 0.002), more than one implicated calix (p = 0.001), more than one puncture (p < 0.001), GSS (p < 0.001), and CNN (p < 0.001) were significant predictors of OT. On multivariate regression analysis controlling for confounding based on GSS, SB and GSS significantly predicted operative duration (Table 3). On linear regression, after controlling for confounding, only SB independently predicted OT and CNN could not (Table 4). Univariate analysis revealed that presence of staghorn (p < 0.001), multiple stones (p = 0.006), more than one implicated calix (p = 0.027), more than one puncture (p = 0.026), GSS (p < 0.001), and CNN (p < 0.001) were significant predictors of LOH. On linear regression controlling for confounding, SB and complications significantly predicted LOH. GSS and CNN did not predict LOH (Tables 3 and 4).
Bold values indicate significant p value (p < 0.05).
LOH = length of hospitalization.
Bold values indicate significant p value (p < 0.05).
Risk stratification
In GSS, taking grade I as reference category, grade II, III, and IV had relative risk of 1.48, 1.37, and 3.03 for residual calculi, respectively. Taking a CNN value of ≥220 as reference category, patients with CNN value of 130 to 169 had a relative risk of 3.2 and 170 to 219 had a relative risk of 2.18 for residual calculi. Only one patient had a CNN value of 80 to 129, and hence, relative risk could not be calculated (Table 2).
Discussion
Predictors of PCNL success are multifactorial, including stone characteristics like SB, location, number of stones, presence of staghorn stones, case volume, and prior treatment. 7 SB is the most influential parameter to predict PCNL success. 7,14 Standardization of patient outcomes reporting in PCNL is gaining importance. 15 Based on imaging modalities, various tools have been devised to predict PCNL outcomes. The Staghorn morphometric scoring system using CT was devised to predict number of tracts and stages required to achieve treatment success, but it is not applicable to nonstaghorn stones. 16 GSS, S.T.O.N.E., and CNN scores were developed to preoperatively prognosticate PCNL outcomes. 5 –7
GSS vs CROES nomogram
GSS is based on renal stone complexity and predicts SFR but not complications. 5 GSS was externally validated. 17,18 GSS has some demerits. It is based on expert opinion. 7 Abnormal renal anatomy does not result in inferior surgical outcomes. 19 Vague definitions of partial and complete staghorn stone result in under- or overgrading cases as grades III and IV, respectively. 14 Smith and colleagues felt the necessity of a data-driven risk estimator to predict PCNL outcomes better and developed the CNN using preclinical and radiological data. They found CNN predicted SFR significantly better than the GSS. 7 Although it is a more complete scoring system, the complexity of its design limits its daily applicability in clinical practice. 8,14
Stone-free rate
We observed both GSS and CNN to have equal predictive accuracy for SFR after PCNL and it was similar to that predicted by SB as also observed by Tailly and colleagues 8 and Labadie and colleagues. 14 Sfoungaristos and colleagues found good predictive accuracy of CNN with AUC 0.715. 9 We found that number of implicated calices influenced SFR on multivariate analysis as also observed by Sfoungaristos and colleagues. 9 We observed that number of punctures also influenced SFR in our study.
Complications, OT, and LOH
None of the scoring systems has been able to predict postoperative complications. 8,20 Our results corroborate with these findings. We found that CCI and presence of staghorn stones also independently predicted complications. Bozkurt and colleagues found that CNN and GSS were predictive of estimated blood loss, OT, and overall complications. 21 However, Tailly and colleagues revealed that both these scoring systems did not independently predict OT. 8 We report that GSS and SB were independent predictors of OT. CNN failed to predict OT on linear regression. We observed that the scoring systems failed to predict LOH as also reported by Tailly and colleagues. 8 In fact, we found LOH to have a high likelihood of association with complications. Risk stratification for residual stone was better defined by the quartiles of CNN as also reported by Tailly and colleagues. 8
Limitations
Although CT KUB is the best method to assess SFR, we performed only kidney, ureter, and bladder radiograph and ultrasound KUB, which have relatively low sensitivity for diagnosing residual calculi. This was a single-center study.
Conclusion
CNN is a more complete scoring system than GSS with better risk stratification for residual stone after PCNL but it predicts complications less accurately. GSS predicts operation duration as well. The cumbersome design of CNN makes its everyday application challenging. The inclusion of number of implicated calices will improve preoperative prediction of SFR, and CCI will improve prediction of complications in PCNL.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.