
Abstract
Purpose:
To examine the impact of ambient temperature on the incidence of emergency department (ED) admissions for acute renal colic and the potential influence demographics and comorbid conditions may have on this.
Methods:
We conducted a population-based time series analysis using linked healthcare databases in Ontario, Canada, which included all residents, aged ≥19 years, who were admitted to an ED from April 2002 to December 2013. The primary outcome was daily number of renal colic emergency department admissions. A distributed lag nonlinear model with 21 days of lag was applied to estimate the cumulative effect of temperature on colic admissions. We estimated risks for cold and heat, defined as temperatures below and above the optimal temperature, which corresponded to the point with minimum risk of colic admissions. We conducted stratified analyses using selected demographics and comorbidities.
Results:
During the study period, 423,396 patients presented to an ED with colic. There was a significantly increased risk of colic as ambient temperature increased (rate ratio [RR] = 1.30, 95% confidence interval [CI]: 1.20, 1.42). Subgroup analysis demonstrated an increased risk associated with heat for both genders; however, this risk was more pronounced in males with extreme heat (RR = 1.64 vs 1.22, p = 0.006). In contrast to other age groups, there was an increased risk for those in their 40s (RR = 1.42), 50s (RR = 1.54), and 60s (RR = 1.31) (p = 0.02).
Conclusion:
Increasing ambient temperature was associated with increased risk of ED visits for colic, particularly in males and those aged 40 to 69 years.
Introduction
N
The body of evidence supporting the link between ambient temperature and nephrolithiasis includes observed seasonal and geographic differences in nephrolithiasis rates 8 –10 and urinary calcium and oxalate excretion. 11 Several recent studies have also suggested that high temperatures are associated with short-term increases in the risk of nephrolithiasis 6,7,12 ; however, no previous studies have assessed whether certain subgroups of the population would be at a greater risk of nephrolithiasis as a result of exposure to ambient temperature. Given that climate change is projected to increase the intensity and frequency of daily high temperature around the world, such information is vitally important for developing public health preventative strategies to reduce the burden of nephrolithiasis and renal colic associated with this ubiquitous environmental factor.
Accordingly, we conducted a population-based study to investigate the impact of ambient temperature on the incidence of emergency department (ED) admissions for acute renal colic and to examine the extent to which the association may differ according to important demographic and comorbid characteristics.
Methods
Design and setting
We conducted a provincial population-based time series analysis using Ontario's linked healthcare databases held at the Institute for Clinical Evaluative Sciences. The province of Ontario, Canada, currently has a population of ∼13 million residents. Because of universal access to hospital care and physician services, these healthcare databases include all residents of Ontario. The study was approved by the Research Ethics Board at the University of Toronto, Ontario, Canada.
Data sources
Four main administrative data sources were utilized to ascertain baseline characteristics, covariate information, and outcome data. The Ontario Health Insurance Plan (OHIP) database contains information on inpatient, outpatient, and laboratory services based on billing claims from Ontario physicians. The Canadian Institute for Health Information Discharge Abstract Database (CIHI-DAD) and the National Ambulatory Care Reporting System (NACRS) database have demographic, diagnostic, and procedural information for all inpatient and ED visits, respectively. The Registered Persons Database (RPDB) contains demographic information on all Ontario residents, including their sex, date of birth, postal code, and vital status. All of these databases have been used extensively to research health outcomes. 13
Study population
The study population consisted of residents of Ontario, aged ≥19 years, who were admitted to an ED between April 1, 2002, and December 31, 2013. The daily numbers of ED visits were identified through the NACRS database. We calculated daily counts of renal colic admissions to the ED, determined by International Classification of Diseases 10th Revision [ICD-10] codes (Table 1), which occurred in each of the 14 health regions in Ontario (Supplementary Fig. S1; Supplementary Data are available online at
CHF = congestive heart failure.
Health outcome and comorbid conditions
The primary outcome was trends in the number of renal colic admissions to the ED relative to ambient temperature. These trends were examined across all patients and within numerous subgroups of the population, including by demographics such as age, gender, and socioeconomic status (income quintile—five categories representing average neighborhood income determined by postal code), and by selected comorbid conditions, including hypertension, diabetes mellitus (DM), congestive heart failure (CHF), and chronic kidney disease (CKD). To identify individuals with any previous diagnosis of hypertension, diabetes, and heart failure, we linked the study population to three validated Ontario databases of all residents diagnosed with these conditions. 15 –17 To ascertain whether individuals had any history of CKD, we examined their records of hospitalization and ED visits for all diagnostic codes for this condition within 2 years before the ED admission date for colic. 18 All demographic data were obtained from the RPDB.
Weather data
Hourly meteorological data on mean, minimum and maximum temperatures, and relative humidity at all weather monitoring stations across Ontario during the study period were provided by Environment Canada. We computed daily means of each meteorological variable for each station, and then averaged daily data across all weather stations within each health region to derive region-specific mean daily estimates, which were then assigned to study subjects using their residence at time of admission.
Statistical analysis
We conducted a two-stage analysis to investigate the associations between temperature and renal colic admissions to the ED. In the first stage, the regional associations between daily mean ambient temperature and renal colic admissions were analyzed using a distributed lag nonlinear model methodology. 19 This accounts for a delay between temperature extremes causing stone formation and symptomatic presentation. To capture the nonlinearity, daily temperature was transformed by a natural cubic spline with 5 degrees of freedom (df), placing four internal knots at temperature percentile scale equally (20th [lower temperature], 40th, 60th, and 80th [higher temperature]). To capture the lagged effect, temperature was assumed with the lag as much as 21 days (based on previous research 6 ) and modeled by a natural spline with 3 df, placing knots at equally spaced log scale of lag. The model adjusted for seasonal and long-term effects using a natural cubic spline function of time with 7 df/year. In addition, we adjusted for daily mean relative humidity, a categorical variable for the day of the week, and an indicator variable for statutory holidays to control for potential holiday effects. Model selection was based on a quasi-Akaike information criterion value to select the degree of freedom of spline functions for temperature variable and lagged effect. In the second stage, we pooled health region-specific estimates across Ontario using a multivariate meta-analysis 20 to obtain overall association of temperature and renal colic admissions.
The temperature–renal colic admission curve was represented by the provincial overall cumulative relative risk of admissions across 21 days against the percentile scale of daily mean ambient temperature. The percentile of temperature with the minimum overall cumulative relative risk was selected as the minimum morbidity temperature (MMT) percentile that can represent the optimal temperature for individuals. Consistent with previous studies of temperature health effects, 21 the relative risk of the 1st percentile temperature vs MMT of temperature was calculated to represent cold effect; while the relative risk of 90th percentile temperature vs MMT of temperature was calculated to represent heat effect. We also evaluated the risk associated with extreme heat represented as the 99th percentile temperature vs MMT.
To identify potentially vulnerable subpopulations, we conducted stratified analyses for each health region by age, sex, income, and region of residence and history of hypertension, CHF, DM, and CKD. A multivariate Wald test was used to assess the statistical significance of effect modification for each selected characteristic (p < 0.05 considered significant).
Results
During our study period, 423,396 patients presented to an ED in Ontario with renal colic. Baseline demographics can be found in Table 1. As would be expected from a population of kidney stone patients, the median age was 47 (IQR 37–57) and there was a greater percentage of men (62%). The descriptive statistics of daily mean temperature in each of 14 health regions are reported in Supplementary Table S1. The temperatures were warmer in the southern health region and Central Ontario relative to those in the north.
Examining the entire cohort, there was a significantly increased risk of renal colic requiring an ED visit with increased daily ambient temperature (rate ratio [RR] = 1.30, 95% confidence interval [CI]: 1.20, 1.42). This risk was further increased with extreme heat (RR = 1.48, 95% CI: 1.33, 1.64) (Fig. 1). In contrast, there was no evidence of cold effect (RR = 1.01, 95% CI: 0.92, 1.11). We noted that daily mean temperatures at the 10th percentile exhibited the minimum risk for renal colic in Ontario.

Graph of the relative risk of emergency department visit for renal colic by temperature percentile in Ontario, Canada. The highest temperature percentiles represent warmer ambient temperature.
Subgroup analysis by age category demonstrated a significantly increased risk of renal colic with increased ambient temperature for the age categories spanning 40 to 69 years of age (p = 0.02) (Table 2 and Supplementary Fig. S2). For those in the age 19 to 39 category, increased risk was only apparent for extremely high ambient temperatures (RR = 1.32, 95% CI: 1.08, 1.60) and no increased risk was seen in those >70 years of age (Table 2 and Supplementary Fig. S2).
p-Value assesses statistical heterogeneity for each of the stratified variables. A p-value <0.05 is interpreted as a significant statistical interaction between the variable and the ambient temperature.
Both genders demonstrated an increased risk of colic with increasing ambient temperature (males: RR = 1.36, 95% CI: 1.22, 1.52; females: RR = 1.20, 95% CI: 1.05, 1.38) (Table 2 and Fig. 2); however, extremely high ambient temperature was associated with a significantly greater risk in males compared with females (RR = 1.64, 95% CI: 1.43, 1.88 vs RR = 1.22, 95% CI: 1.04, 1.44; p = 0.006 for gender effect modification) (Table 2).
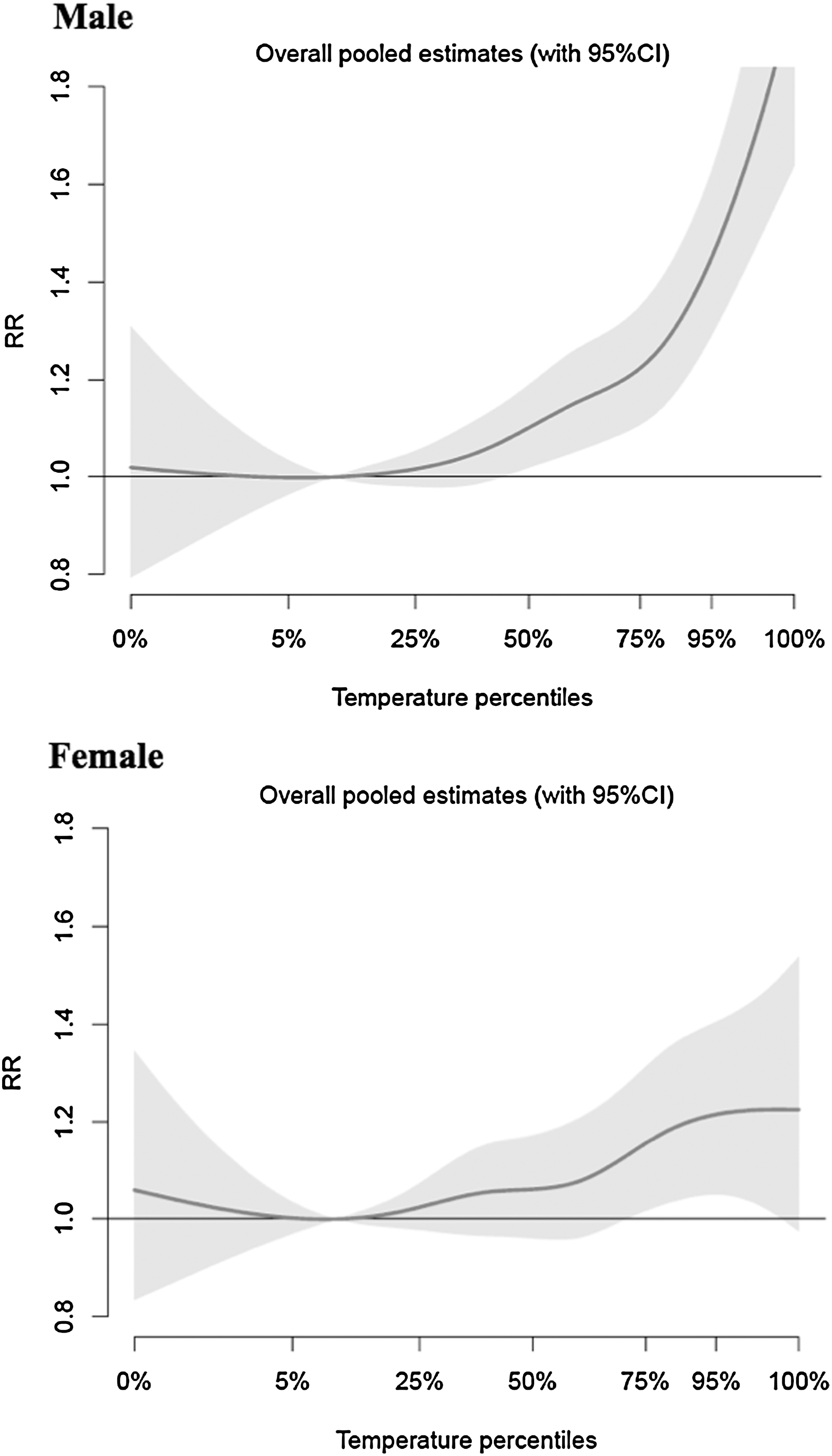
Graph of the relative risk of emergency department visit for renal colic by temperature percentile stratified by gender in Ontario, Canada.
Income did not significantly influence the risk for colic, although the RRs suggest potentially a greater risk in the third and fourth income quintiles with no increased risk in the highest and two lowest income quintiles (Table 2 and Supplementary Fig. S3).
Region of residence (urban vs rural) also did not significantly modify the risk for colic with increasing ambient temperature (Supplementary Fig. S4).
In terms of comorbid conditions, hypertension trended toward a significant modifying effect on the increased risk of renal colic with increasing temperature (RR = 2.02, 95% CI: 1.27, 3.22 vs RR = 1.28, 95% CI: 1.17, 1.40; p = 0.06) (Table 2 and Supplementary Fig. S5). This potential modifying effect was accentuated with extremely high ambient temperatures (RR = 2.37, 95% CI: 1.35, 4.14 vs RR = 1.45, 95% CI: 1.31, 1.61; p = 0.09). No increased risk was demonstrated for DM (Table 2). Due to the relatively small number of stone formers with a history of CHF or CKD, we were unable to obtain meaningful risk estimates for these subgroups.
Discussion
We conducted this study to determine if there was an increased risk of renal colic requiring presentation to an ED with increasing ambient temperature and if certain characteristics modified this risk. Our results add weight to a small but growing body of literature demonstrating an increased risk of colic with increasing temperature. 6 –8 In addition, our study found that males and those aged 40 to 69 were at higher risk with hotter temperatures as well as a potential modifying effect of hypertension.
To our knowledge, this is the first report assessing the risk among demographic subgroups and comorbid subpopulations for renal colic with increasing ambient temperature. These findings are important given the continued threat of climate change; it is estimated in the next century that average global temperatures will increase by 1°C to 4.5°C due to increases in greenhouse gas emissions. 22 The most at-risk subpopulations identified in the present study will help inform physicians about specific patients who should be counseled about behavioral changes (such as avoiding outdoor temperature extremes or increasing fluid intake during the summer) during periods of high ambient temperatures.
In the present study, both genders demonstrated an increased risk of renal colic with increasing temperature; however, the effect was more pronounced in males at higher temperatures. There are a couple of potential explanations for this difference. First, it might be related to work environment and access to water. 8 Men more commonly work outdoors and they might be more susceptible to the effect of ambient temperature, specifically perspiring more and having limited access to water, resulting in lower urine volumes. A study examining gender differences in seasonal variation of stone risk factors supports this as it demonstrated that men, but not women, had lower urine volumes in summer, with higher calcium oxalate supersaturation, as well as lower urine pH contributing to a difference in the risk of uric acid stones. 23 In addition, working outdoors likely results in men having greater exposure to sunlight, which may result in sunlight-induced increases in vitamin D. Second, differences in stone composition might also play a small role. 8 Females are more commonly afflicted with struvite stones compared with men (3:1 females to male ratio). 24 As struvite stones are related to infection, not low urinary volume or supersaturation of calcium or uric acid, they are less likely associated with ambient temperature.
Those aged 40 to 69 years also demonstrated an increased risk of renal colic, while the youngest age stratum only showed an increased risk with extreme ambient temperature and the oldest age stratum showed no increased risk. This might be explained by a differing effect of heat on urine chemistries and volume by age and also by differing exposure to ambient temperature. The oldest age strata most likely spend the greatest amount of time indoors in a controlled environment and are therefore less likely to be exposed to the effect of increased ambient temperature. Conversely, the youngest age strata (although likely exposed to the effect of the ambient temperature) might be less sensitive to this in terms of urine volume and supersaturation of calcium salts; however, data supporting this hypothesis are unavailable.
Considering socioeconomic status, previous studies have suggested that a population has to reach a moderate to high standard of living before ambient temperature plays a role in stone formation 25,26 ; however, in the present study, income did not appear to affect the risk for colic in association with heat.
Similarly, region of residence (urban vs rural) did not significantly affect the risk for colic in association with high ambient temperatures in the present study, contrary to the suggestion of a prior study. 27
Hypertension did not demonstrate a significant modifying effect on the risk for renal colic due to high daily temperature, but did represent the highest RR of all subgroups. A couple of prior studies support a physiologic mechanism whereby people with hypertension may have an increased risk of colic with increasing ambient temperature, 28,29 but our study did not convincingly show this.
Our results must be interpreted within the limitations of our study. First, we did not have data on the stone composition, sunlight exposure, or whether individuals worked outdoors and so we can only postulate that these variables might help explain the trends that were demonstrated for age and gender. Second, we relied on fixed-site monitoring stations for daily weather rather than measuring individual exposures, which may have led to exposure error because of variability at individual residences and daily activity patterns. However, previous studies using both monitoring data and spatial models to predict temperature at residence found similar risk estimates. 30 Given that exposure errors are likely to be random, our assessment of our primary exposure was likely subject to nondifferential misclassification that would attenuate our estimates.
Conclusion
Our study demonstrated that increasing ambient temperature in Ontario was associated with increased risk of ED visits for renal colic, particularly for certain demographic subgroups. The results from this study provide evidence to guide public health preventative measures to help reduce the impact of increased daily temperatures on the burden of renal colic and nephrolithiasis.
Footnotes
Acknowledgments
This work was conducted at the Institute for Clinical Evaluative Sciences (ICES). ICES is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care. The opinions, results, and conclusions reported in this article are those of the authors and are independent of the funding sources. Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions, and statements expressed herein are those of the author, and not necessarily those of CIHI. The authors thank Richard Burnett (Health Canada, Ottawa) for advice and suggestions on the conception and design of this study. This study was supported by a contract from Health Canada (Contract No. 4500302837).
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.