
Abstract
Introduction:
Laparoscopic partial nephrectomy (LPN) remains challenging in endophytic and complex kidney tumors as the clear understanding of tumor location and spreading depends on a precise analysis of available imaging. The purpose of this study was to investigate navigated kidney surgery using intraoperative cone-beam computed tomography (CBCT) images in conjunction with a previously proposed method for augmented reality (AR) guidance for safe LPN.
Materials and Methods:
The concept proposed is based on using an intraoperative CBCT scan for (1) marker-based AR guidance for fast and reliable tumor access and (2) enhancement of real-time fluoroscopy images for accurate tumor resection. Workflow and accuracy of the system were assessed using a porcine kidney model. Ten patients with complex or endophytic tumor localization and R.E.N.A.L. Nephrometry Score of at least nine scheduled for LPN were included in this study. Patients received an intraoperative CBCT after marker placement. Defining the resection line was assisted by AR. In addition, fluoroscopy imaging for depth perception was used for assistance during dissection. Feasibility and performance were assessed by histopathological results, peri- and postoperative data.
Results:
Surgery was performed successfully and negative margins were found in all cases. Segmental branches of the renal artery shifted as much as 10 mm in the vertical and 11 mm in the sagittal axis intraoperatively compared to preoperative imaging. Fluoroscopy to intraoperative computed tomography image fusion enabled enhanced depth perception during dissection in all cases. Radiation dose area product was 4.8 mGym2.
Conclusions:
The application of the navigation system is feasible and allows for safe and direct access to complex or endophytic renal masses. Radiation limits the application to selected indications.
Introduction
L
Therefore, different concepts of image-guided surgery have been introduced during the last decade. 5,6 Most concepts provide additional assistance by enhanced visual information during surgery, commonly based on preoperative cross-sectional imaging. While these approaches considerably enhance surgical vision, two challenges remain to be addressed. 7 First, they were not able to superimpose the imaging accurately during organ deformation. Second, augmented reality (AR) could only be used as a surface template, but was not able to improve vision underneath the surface. Therefore, we address these two issues by presenting a novel concept for navigated laparoscopic interventions based on intraoperative cone-beam computed tomography (CBCT) images. Our concept combines the advantages of marker-based AR guidance with a new strategy for enhanced depth perception based on fusion of intraoperative three-dimensional (3D) CBCT images with continuously acquired fluoroscopic data.
Herein, we present the first in-vivo experience in laparoscopic partial nephrectomy (LPN) for endophytic kidney tumors with intraoperative CBCT and fluoroscopy fusion combined with AR.
Materials and Methods
The following sections describe our approach to CBCT-guided navigated renal surgery, the experiments performed to assess the accuracy of the method proposed, as well as an in vivo application of the system in 10 patients.
Navigation concept
The proposed workflow of CBCT-guided renal surgery comprised the following steps: (1) Preparation: To prepare the later steps the renal surface had to be uncovered from the surrounding tissue to guarantee a clear view to the organ. (2) Marker insertion: Custom designed radiopaque needle-shaped fiducials, as described in Baumhauer et al.,
7
were placed on the surface of the organ. The placement needed to be done in a way to enable constant detection of all markers within the field of view during resection. A minimum distance between the makers of at least 1 cm is needed. (3) Intraoperative CBCT acquisition: To generate a current virtual 3D model containing anatomical structures and markers, a CBCT scan was performed. A multiaxis robotic C-arm system (Artis zeego, Siemens Healthcare, Germany) was used in a hybrid operating room. It consisted of a robotic arm that is able to position and move the mounted C-arm within the operation theatre (Fig. 1). For segmentation, the open-source Medical Imaging Interaction Toolkit (MITK)
8
was used. (4) AR guidance for tumor access: The intraoperative CBCT image was continuously fused with the endoscopic video data using the marker-based navigation approach (Fig. 2) described in detail in Refs.
7,9,10
Note that in contrast to previous work, intraoperative tomographic data were used to estimate the location of subsurface structures (Fig. 3). The accuracy of the marker-based AR method has already been validated in an ex-vivo model. The target registration error (TRE) was calculated as 0.5 mm.
7
(5) Real-time CBCT fluoroscopy for tumor resection: Fluoroscopic images acquired with the CBCT scanner during tumor resection were enhanced by previously extracted anatomical structures (see step (3)) as shown in Figure 4. By moving the C-arm, the fluoroscopic ray pathway changes and enables depth perception during resection process.

Intraoperative imaging with the cone-beam computed tomography—schematic illustration of the floor-fixed, robotic-driven C-Arm, rotating around the patient intraoperatively.
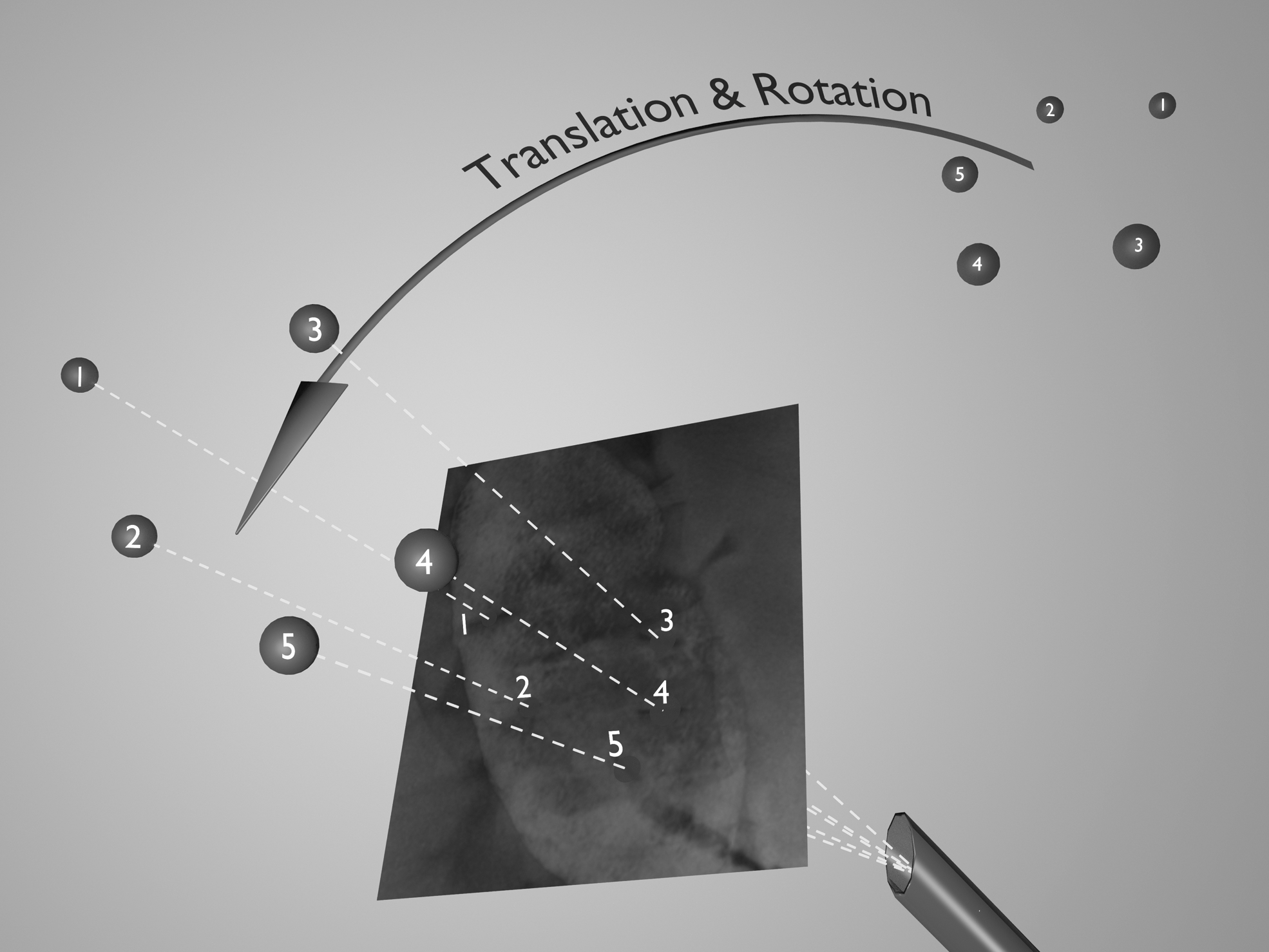
Principle of inside-out tracking: An algorithm searches for each marker (five spheres) in every endoscopic video frame and calculates the position of the endoscopic camera in relation to the fiducials. The changes of angles and distances of the markers to each other, in each image frame, can be calculated and related to previously measured parameters of the endoscope.

Illustration of selected computed tomography (CT) slices showing high-resolution imaging even of segmental vessels intraoperatively.
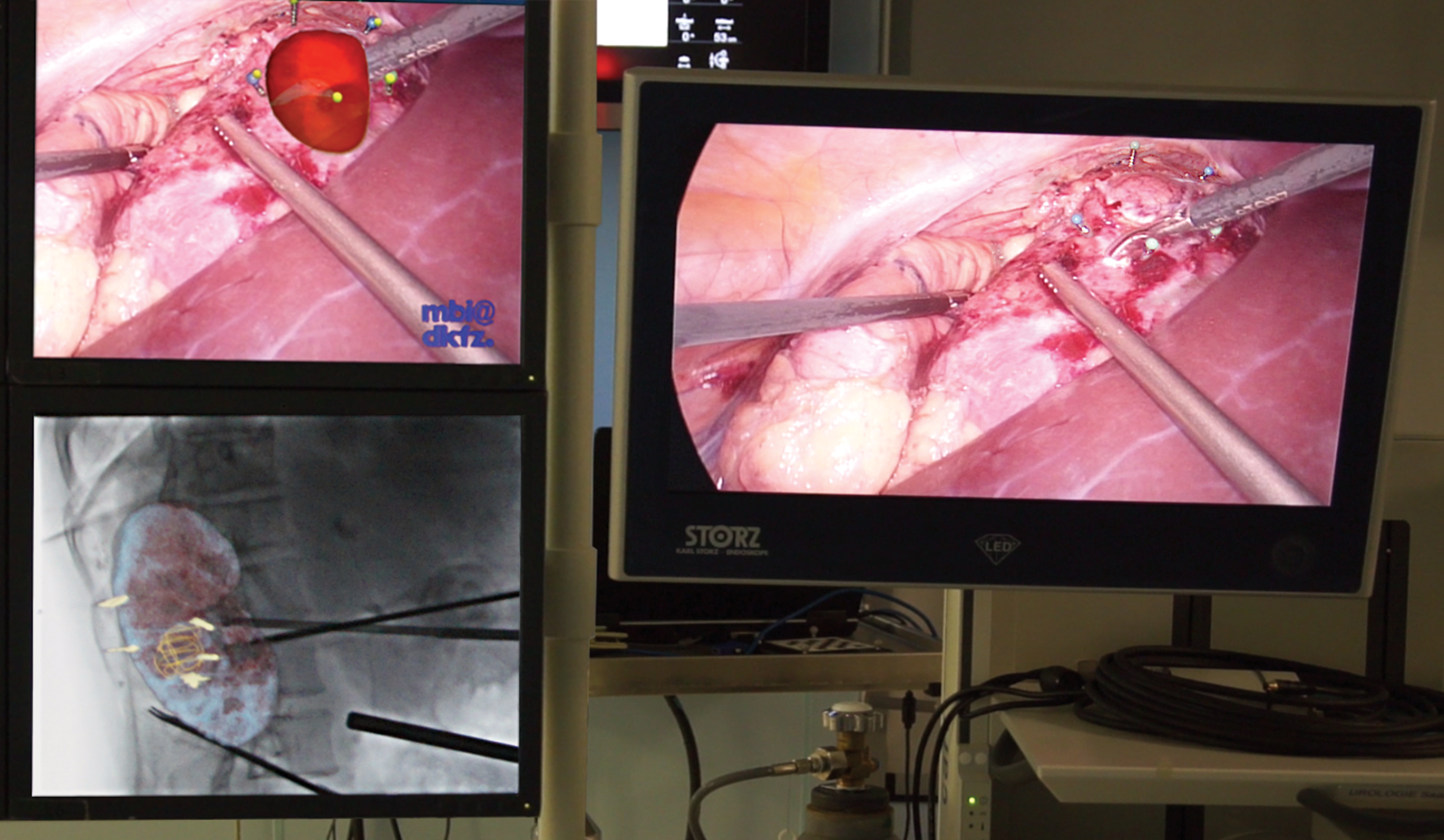
Surgeons view on three screens simultaneously: The augmented reality (AR) video (upper left screen) showing the overlaid three-dimensional model of the tumor (red). The AR fluoroscopy image (bottom left screen) showing real-time fluoroscopy and determining spatial relationship of surgical instruments and tumor (yellow mesh). The conventional laparoscopic image (right screen) represents the image reference.
Clinical application
To assess the feasibility in the clinical routine, 10 patients with suspicious renal masses were selected due to tumor complexity or localization according to R.E.N.A.L. Nephrometry Score (Table 1). 11 Following good clinical practice, the patients were thoroughly informed, regarding all details of the planned procedure, especially the aspect of radiation exposure. Written informed consent was obtained. Table 2 shows patients' characteristics.
R = radius; E = exophytic/endophytic properties; N = nearness of tumor to the collecting system or sinus; A = Anterior/posterior; L = location relative to polar lines.
Data are presented as median (range).
ASA = American Society of Anesthesiologists Classification; BMI = body mass index; CBCT = cone-beam computed tomography; MDRD eGFR = estimated glomerular filtration rate using modification of diet in renal disease formula.
The surgical workflow followed the described steps and consisted of (1) a laterocolic incision, hilum identification, and controlling of the blood vessels, (2) marker placement (Aesculap, Germany), (3) intraoperative CBCT imaging, (4) segmental artery preparation, marker-based AR navigation for defining the resection line, and (5) fluoroscopy-assisted tumor dissection. Following our standard, a laparoscopic ultrasound device (Hitachi Medical Systems, Switzerland) was used to validate the correct resection lines. Patients were placed in a hyperextended flank position (Fig. 1), allowing a full rotation of the CBCT arm. Laparoscopic access was transperitoneal and four ports were used. 12,13 Before inducing ischemia, a total of 15 g of mannitol in 100 mL sterile water was given. If possible, selective ischemia was performed by placing bulldog clamps, depending on favorable tumor localization and the presence of pole arteries, or early divisions of segmental arteries.
CBCT imaging
During CBCT imaging, the system acquired projection images on a 200° circular trajectory around the patient. A contrast enhanced CBCT acquisition protocol with a slice thickness of 1 mm was used for marking and segmenting the tumor and risk structures (Fig. 3). For this purpose, a bolus of 100 mL contrast agent (Accupack 350 mg/100 mL; GE Healthcare, Germany) was injected intravenously.
Rigid point-to-point registration of anatomical landmarks (ribs, vertebra) in pre- and intraoperative cross-sectional images was performed to quantify the deformation (shifting) of tumor location and vascular structures.
AR-enhanced laparoscopy
As an additional tool, the intraoperative-performed computed tomography (CT) image was superimposed to the current laparoscopic view. Therefore, the acquired CBCT 3D data set was transferred to a standard laptop to create a 3D model using MITK. By semiautomatic segmentation and volume visualization, kidney, tumor, blood vessels, and markers were reconstructed. After calibration of the laparoscopic camera, the system created a real-time AR overlay on the laparoscopic video image, using inside-out tracking (Fig. 4). The resection line was defined by placing coagulation marks around the tumor's border using the AR video.
Fluoroscopy fusion
By fusion of the real-time two-dimensional fluoroscopy image with the intraoperative CT images, the surgeon was enabled to understand spatial relations between instruments' tips and tumor margins (Fig. 4). For this purpose, an additional software tool was used on the postprocessing workstation (syngo iPilot; Siemens Healthcare, Germany). Any change of position of the C-arm system resulted in an automatic adaption of the overlaid 3D information. The real-time AR image was displayed next to the laparoscopic video screen (Fig. 4). Fluoroscopy was controlled by the surgeon by a foot pedal. The images were acquired with 4 frames/seconds and a system dose of 45 nGy/frame. The angle of fluoroscopy varied, so the course of x-ray beams was vertical to renal surface and laparoscopic instruments. The chosen angles were 0° in craniocaudal axis and −15° to 75° in right–left axis.
Statistics
The findings were analyzed with descriptive statistics using the statistical computing environment R (The R Foundation for Statistical Computing, Austria).
Results
Surgery was performed successfully in all cases. The median operation time was 110 minutes (95–160 minutes). Median selective warm ischemia time was 11 minutes (8–20 minutes). The prolongation of the intervention caused by intraoperative imaging and registration was 15.5 minutes (9–20 minutes). Renal function decreased from a preoperatively median estimated glomerular filtration rate of 78.5 mL/min/1.73 m2 (55–127 mL/min/1.73 m2) to 74.5 mL/min/1.73 m2 (35–89 mL/min/1.73 m2) postoperatively. Negative surgical margins were found in all cases. Follow-up (10–24 month) showed no evidence of local recurrence.
Fully automated initial image acquisition took 40 ms (25 frames/seconds). Median Radiation exposure was 16 seconds during CBCT and 120 seconds (90–180 seconds) during fluoroscopy. This resulted in a received median radiation dose area product (DAP) of 4.5 mGym2 (2–9 mGym2) caused by CBCT and 0.2 mGym2 (0.15–0.3 mGym2) caused by fluoroscopy.
After placing the patient in the flank position, the segmental branches of the renal artery shifted as much as 10 mm (4.5–13.5 mm) in the vertical and 11 mm (6–12.5 mm) in the sagittal axis compared to preoperative imaging (Fig. 5). With intraoperative imaging, the position of segmental arteries could be identified easily.
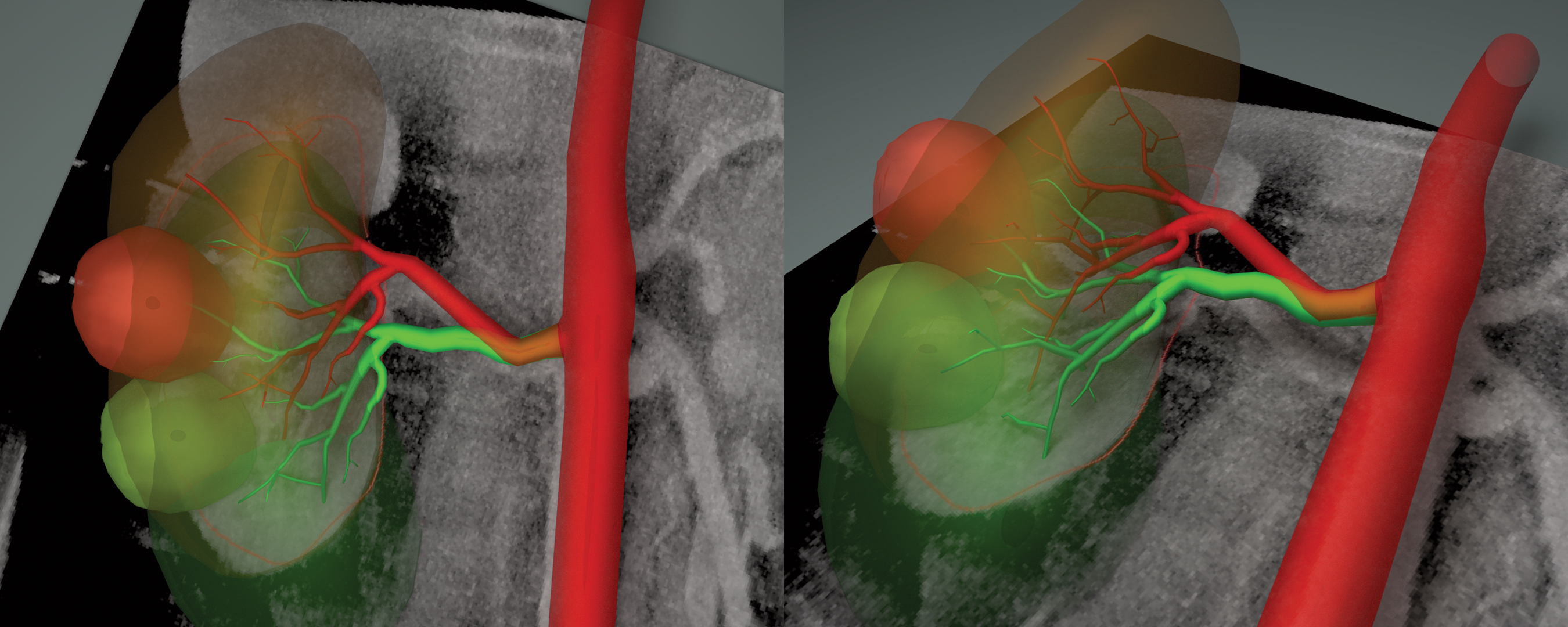
Image overlay comparing pre- and intraoperative CT scans: Significant vessel shift and deformation preoperative (green vessel tree) and intraoperative (red vessel tree). Relevant fusion error probability for AR by relying on preoperative imaging only.
Intraoperative CT with high-resolution images could be applied successfully in all cases. Especially in cases of sticky fat tissue, the early projection of the tumor could avoid decapsulation of the kidney and enabled an accurate preparation, while the fat tissue was spared. Fluoroscopy fusion enabled enhanced depth perception during resection in all cases. The fluoroscopic to CT scan image fusion was only possible between an angle of 70° to 110° in right–left axis and 15° to 30° in craniocaudal axis to reach a rigid fusion error below 2 mm.
Discussion
The use of intraoperative CBCT is well established in vascular surgery as it enables complex minimal invasive endovascular treatment with reduced perioperative morbidity. 14 In several publications, vascular and cardiac surgeons could demonstrate more precise visualization of difficult anatomy during endovascular procedures. 15,16
In PN, different attempts for image guidance have been published. 9,17 In all approaches, preoperative CT imaging was used to reconstruct 3D models. However, all groups suffered from soft tissue deformation and movement due to respiration, surgical manipulation, and patient positioning. Intraoperative CBCT imaging has the advantage of representing the current position of the anatomy during surgery. Especially in endophytic tumors or high R.E.N.A.L. Score patients, the accurate understanding of risk structures (bowel, vessels) in relation to target structures is essential. This relationship changes significantly due to insufflation and surgical manipulation from the preoperative to the intraoperative setting. Schneider et al. demonstrated that just changing the patient position from supine to flank causes a caudal organ shift of 46.5 mm and a rotation of 25°. 18 In concordance to that, we could demonstrate that due to flank position, the segmental branches of the renal artery shift as much as 10 mm (4.5–13.5 mm) in the vertical and 11 mm (6–12.5 mm) in the sagittal plane compared to preoperative imaging. Therefore, intraoperative imaging enables a more precise superimposition of risk structures.
Furthermore, Shekhar et al. demonstrated that “live AR” by means of continuous multislice CT scans with an update rate of one per second, could clearly reduce the TRE from 3.63 mm (utilizing preoperative CT scan) to 1.45 mm. 19 However, they repeatedly performed CT scans with a conventional CT scanner, which does not allow real-time segmentation and interrupts surgery. To overcome these limitations, we used fluoroscopy fusion in our study. It offers real-time imaging during dissection and a spatial understanding of the intraparenchymal resection line, without performing repeat CT scans like in other CT-guided interventions.
AR, even with accurate superimposition of the tumor structures, enhances perception as mentioned above, but does not give good depth perception during the resection process. The standard use of intraoperative ultrasound does only help in determining resection lines before starting the procedure. Its feasibility during the resection process itself is limited due to the necessity to place the ultrasound device directly in the surgical site. However, our study was not designed to provide objective evidence showing a superiority of intraoperative fluoroscopy to ultrasound. In contrast to intraoperative ultrasound, simultaneous fluoroscopy showed its major benefit within this study, as the automatic fusion of the segmented intraoperative CT image with real-time fluoroscopy during resection allowed a correct 3D perception of the resection process. Moreover, it has the potential benefit to project each available data set (vessels, risk structures, or tumor borders) of the CT scan onto the surgical field simultaneously. The accuracy of this fusion depended on the applied angles between kidney's sagittal axis and the fluoroscopic axis. We could demonstrate the best accuracy within a range of 40° (70°–110° to table position). This experience is in concordance to Kenngott et al., who demonstrated that in liver resection, the surgical targeting accuracy depended on the applied angles of fluoroscopy. 20 Rotation and inclination of the C-Arm beyond that range represent a technical limitation, but where not necessary in this study. Best estimation of the resection line marked previous to resection was achieved while the fluoroscopy axis was almost rectangular to camera axis or rather to the kidney's surface.
Different nephrometry scoring systems are used to quantify tumor anatomy and complexity objectively. 21 The patients in our study were characterized by a high R.E.N.A.L. Score. Especially, the endophytic character might be of major importance in demonstrating the advantage of our technique. Leslie et al. introduced the renal tumor contact surface area as a clinically more relevant parameter in predicting surgical complexity. 22 They showed that, the larger the surface area between tumor and its surrounding renal parenchyma, the greater the amount of kidney tissue excised, therefore, requiring a more extent renorrhaphy during PN surgery. One explanation for this might be that the surgeon has no image guidance during the dissection process, especially in endophytic tumors. Even the often used intraoperative ultrasound is only applicable before and not during the resection process. Surgeons have to determine the resection line by the parenchymal impression of benign or malignant tissue. AR combined with fluoroscopic fusion, as shown in this study, facilitated a revalidation of spatial relationship between instrument tip and parenchymal resection line and lead to negative margins in all cases.
One drawback of using CBCT imaging is the radiation dose received by patient and the operating team. However, the overall DAP generated in this study is slightly smaller than the one of the soft tissue protocol published by Rassweiler et al. used during endourologic surgery (4.7 vs 5.07 mGym2). 23 They estimated the effective dose to be 7.76 mSv by applying 129 thermoluminescense dosimeters within a phantom model. Due to the restriction of only one possible C-arm rotation of the CBCT at once, the represented volume as well as the radiation-exposed volume is smaller compared to regular CT scanners. As the effective dose of regular noncontrast-enhanced CT (NCCT) and contrast-enhanced CTs is stated as 4.5–5 and 25–35 mSv, respectively, 24 the assumed effective doses in our study is slightly above a NCCT, but below a conventional contrast-enhanced CT of the abdomen. Furthermore, the effective dose is comparable to interventional renal stone surgery. Lipkin et al. detected an effective dose within percutaneous nephrolithotomy of a left- and right-sided kidney as 7.63 and 8.11 mSv, respectively. 25 Compared to this widely accepted radiation exposure during stone treatment, an even reduced exposure in LPN in selected cases might be justified to facilitate nephron-sparing surgery. As in our study contrast enhanced protocols were used, a negative effect to renal function cannot be excluded. However, no renal failure or relevant deprivation of renal function was seen in our series. Even with the combination of selective ischemia and contrast media, a relevant decrease of renal function could not be detected.
One might argue that in the era of progressing robotic surgery, we performed conventional laparoscopy in all cases. However, Lista et al. showed an increasing positive surgical margin rate for robotic techniques when the complexity of the tumor increases. For assessment of tumor complexity, a similar nephrometry scoring system (PADUA) as in this study was used. 26 In addition, as the indication for minimal invasive surgery expands toward more complex and larger tumors, an increasing number of positive surgical margins were seen by Tabayoyong et al. 27 In this study, similar results for laparoscopic (7.2%–9.1%) and robotic (7.8%–9.1%) techniques were found. Our results revealed no positive surgical margins, although the small number of cases limits its interpretation.
Moreover, the simultaneous use of the robot would result in interference of the robots' arms and the C-arm of the CBCT. Therefore, fluoroscopy does not seem to be possible adequately in this setup. However, it might be worth to analyze new developments in robotic arm or table design to enable an easier integration of telemanipulator systems in surgical fields, because intraoperative imaging will play a more important role in the future. Right now, a full CBCT scan would only be possible after momentary disconnection of the robot.
The indication for this procedure should be reserved for patients with complex or endophytic tumors, where the early perception of correct tumor location and meticulous dissection of segmental arteries before clamping is of major importance. In addition, the understanding of the correct volumetric intrarenal tumor expansion, in relation to the instrument position during resection, is an advantage that might reduce positive margin rates, while sparing more nephrons.
Conclusions
The use of intraoperative CBCT is feasible and safe for patients during LPN. The combination of fluoroscopy and marker-based AR navigation allows for an easy access to difficult endophytic renal masses. The radiation dose limits the application to selected indications with challenging tumor locations.
Footnotes
Acknowledgments
The authors thank Martin von Roden, Siemens AG, Healthcare Sector, for excellent operation of the system during the interventions. Parts of the used methods were supported by the Research Training Group 1126 funded by the DFG (German Research Foundation).
Author Disclosure Statement
No competing financial interests exist.