
Abstract
Purpose:
Saving warm ischemia time (WIT) in laparoscopic partial nephrectomy (LPN) is important. We have designed a new device, a remotely activated bulldog clamp, to facilitate LPN. In present study, the effectiveness, convenience, and safety of the new design device were compared with that of standard bulldog vascular clamp in a pig model.
Materials and Methods:
Fifteen cases of LPN were bilaterally operated on upper or lower pole of kidneys in five pigs. As the test group, eight cases involved the remotely activated bulldog clamp, whereas the remaining seven cases, as the control group, involved the common standard vascular bulldog clamp. The mean operative time, blood lost, and mean WIT were compared between the two groups.
Results:
The mean operative time and blood lost were not significantly different between the groups (p < 0.05). Continuous artery clamping was used in the two groups. With on-demand clamping, the mean WIT in the test group was 19.0 ± 3.42 minutes, which was significantly less compared with the control group (31.54 ± 5.23 minutes, p < 0.05).
Conclusions:
The newly designed device can remotely control the renal artery, which made clamping and unclamping much easier. It is effective and safe in LPN.
Introduction
N
The contemporary vascular bulldog clamps, such as the Satinsky clamp, Aesculap laparoscopic clamp, Klein laparoscopic clamp, and Klein robotic clamp, 6 are always manipulated by the operators during LPN. As the clamping and unclamping is not easy during an operation, the renal artery tends to be clamped before LPN starts. After the tumor is removed and the last stitching completed, the renal artery is unclamped. With the contemporary vascular bulldog clamps, warm ischemia would occur throughout the LPN. Much more ischemia time than necessary should be saved by new technology. In addition, existing vascular bulldog clamps have constant clamping force and pressure. Some of them, such as the Klein robotic clamp, produce significantly less clamping force and, thus, allow more flow across the clamped segment. This may translate into poorer hemostasis intraoperatively. 6
Because of this, we have designed a new device, a remotely activated bulldog clamp (C-clamp), to facilitate LPN. The device can control the renal artery on demand from outside the body. The clamping pressure can be modified and monitored at any time. More important, the C-clamp is manipulated by the assistant. The operator does not need to interrupt his operation. The C-clamp can be activated and released without changing exposure to the partial nephrectomy excision site. This procedure is time consuming in LPN when using common bulldog. We tested the device in a pig model and the results indicated that it could significantly reduce the WIT without excessive bleeding.
Materials and Methods
The structure and mechanisms of the device
The remotely activated bulldog clamp consists of a C-shape clamp with a built-in balloon. A capillary tube is connected to the built-in balloon at its proximal end (Fig. 1A). The distal end of the capillary tube is connected to a removable guide needle. A hand-operated pressure pump with a gauge can be connected to the distal end of the capillary tube after the guide needle is removed. The shape of the clamp is “C”-shaped when it is open (Fig. 1B) and “O”-shaped when closed. When the clamp holds the artery, the hollow “O” shape allows the blood flow through (Fig. 1C). When water is injected into the balloon capillary tube through the pressure pump, the balloon built into the C-clamp (remotely activated bulldog clamp) becomes filled (Fig. 1D), and when the pressure increases to a certain level (the optimal pressure is twice atmospheric), the hollow center of the C-clamp is closed and the renal artery is then blocked. The blockage can be stopped at any time by withdrawing the water.
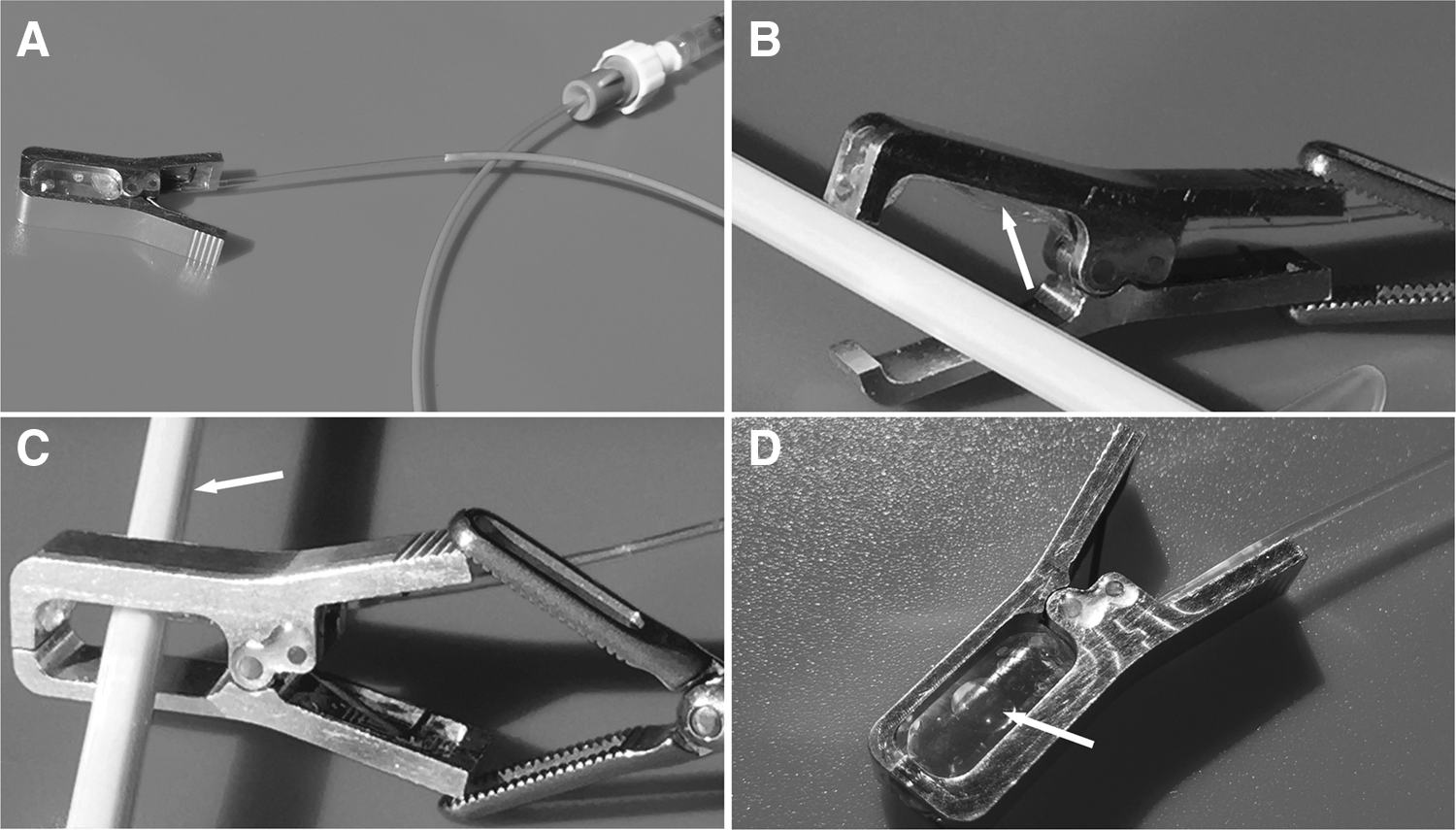
The structure and mechanisms of the device.
Test of clamping force, pressure, and reaction speed
The clamping force was tested in 10 C-clamps using a Chatillon CLC-0010 force gauge at the tip and at the middle point between the fulcrum and tip of the clamp. As the standard clamp, three JZ laparoscopic bulldog clamp (JZ-XEC-250; Shanghai Medical Instruments Ltd., Corp.) were also tested. JZ laparoscopic bulldog clamp is similar with widely applied Aesculap short-curved laparoscopic clamp in clamping force and usage. 6
We set the systolic blood pressure as 180 mm Hg and the level equal to 244.8 cm H2O.
To simulate the blood flow and renal artery, a latex pipe of 5 mm inner diameter was clamped. Water flowed through the latex pipe from a height of 245 cm. Then the built-in balloon of the C-clamp was filled, and pressure was monitored with the pressure pump gauge. When the water flows into the latex pipe stop without leakage, the pressure of the balloon is optimal. The reaction speed of the remotely activated clamp was also tested. The time from water injection by the pump to stopping of leakage is the reaction time. We also tested the response time of the clamping in pig model to verify the in vitro test. The segmental renal artery was preclamped. Reaction time was counted as the in vitro test. To test the clamping ability, the JZ laparoscopic bulldog clamp was also deployed in the in vitro and in vivo examination. (a supplemental video demonstrating this technique is available at
Laparoscopic partial nephrectomy
The study design and methods were reviewed and approved by the Animal Ethics Committee of Zhongshan Hospital Of Fudan University.
In the pig model, 15 cases of LPN were bilaterally operated on the upper and lower pole of the kidneys in 5 pigs. A random decision about the kidney to be tested and which part to excise was made before the operation. As the test group, eight cases involved the remotely activated bulldog clamp. Of them, four cases were used on the upper poles of kidney and four cases on the lower poles. The remaining seven cases involved the common standard laparoscopic clamp (JZ-XEC-250, Shanghai Medical Instruments (Group) Ltd., Corp.) as the control group. Of them, four cases were used on upper pole of kidney and three cases on the lower.
In every case, 2-cm diameter mass of renal tissue was removed from upper or lower pole of the kidney. The removed renal tissue was stored in 4% of formalin. The tissue masses were weighed after all the LPN were completed.
All the operations were performed under general anesthesia using three port technique. As in routine LPN, three trocars were inserted into the body cavity. One of them was for a camera and the other two for the operating apparatus. The renal fascia was open, and the renal artery was completely dissected. In the test group, the remotely activated clamp was placed in the operating field through one of the apparatus trocars. A needle holder was used to bring the guide needle, with the distal end of the balloon capillary tube, outside the body (Fig. 2A, B). The distal part of the capillary tube was then connected to a hand-operated pressure pump after needle removal (Fig. 2C). The time of connection of the device was noted.
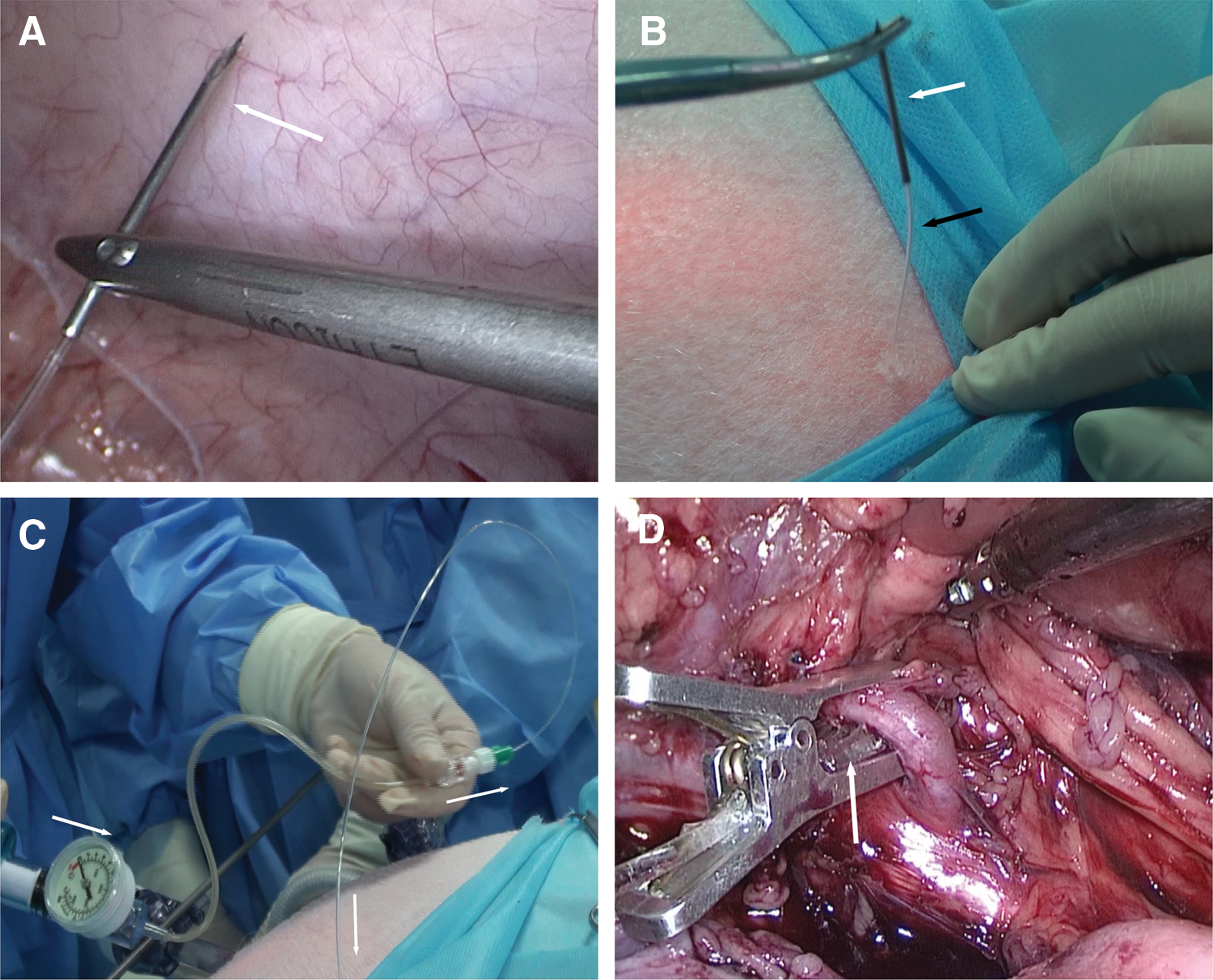
Handling the remotely activated bulldog clamp.
After connection of the device, the C-shape clamp was preheld around the renal artery. This does not affect the bloodstream in the renal artery because of its circular shape (Fig. 2D). The renal artery could be easily clamped or unclamped by injecting or withdrawing the water outside of the body.
To reduce the WIT and to avoid early bleeding, the renal tissue should be cut around the mass to be excised from the superficial to deeper layers without blocking the renal artery (Fig. 3A). Once severe bleeding occurs, the assistant can block the renal artery immediately with the device. The doctor does not have to interrupt his action during the operation (Fig. 3B). After the mass is removed and the bleeding is stopped by suture and ligation, the assistant can control the device and restart the blood flow on demand (Fig. 3C). The interruption time for blocking and unblocking renal artery during LPN was noted.
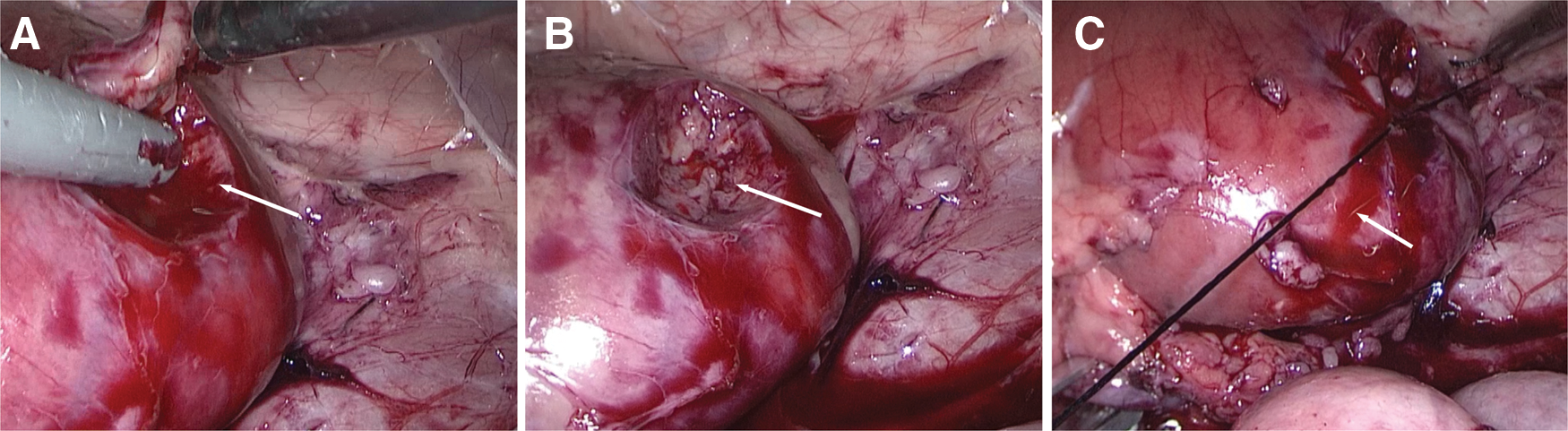
The device is used in LPN.
In the control group, after the renal fascia was opened and the renal artery was completely dissected, it was clamped with a common JZ laparoscopic bulldog clamp (JZ-XEC-250; Shanghai Medical Instruments (Group) Ltd., Corp.). After the tumor was removed and the final stitching completed, the renal artery was unclamped. The interruption times for blocking and unblocking renal artery during LPN were noted.
After each case of LPN completed, the clamp and trocars were removed and the abdominal incisions were closed. Then the pig's position was changed to receive another LPN. The alternate operation allowed the previously ischemic kidney to recover perfusion. This was also helpful to note operative time accurately.
Damage analysis from histopathologic examination
We tested the safety of the device. After 30 min of clamping with JZ laparoscopic bulldog clamp (n = 2) and the remotely activated bulldog under three atmospheres (n = 2), the renal artery was taken out for histopathologic examination and compared with the unclamped renal artery (n = 2).
Statistical methods
The mean operative time, blood volume lost, and mean WIT were compared by t-test with SPSS 19.0 statistics software. All tests were two sided with a significance level of p < 0.05.
Results
We tested the closing force of the 10 remotely activated clamps (C-clamp). The tip of the C-clamp produced a mean 0.69 ± 0.06 kilogram-force (kgf) and the middle point between the fulcrum and tip produced mean 1.02 ± 0.08 kgf.
The tip of the JZ laparoscopic clamp, respectively, produced a mean 0.46 ± 0.05 kgf (n = 3) and the middle point between the fulcrum and tip produced mean 0.61 ± 0.07 kgf (n = 3). The closing force of JZ laparoscopic clamp is similar with that of Aesculap short-curved laparoscopic clamp. It is reported that closing force at tip and middle part of Aesculap short-curved laparoscopic clamp is 0.51 and 0.62 kgf, respectively. 6
In the simulated model of flow with a pressure of 180 mm Hg, the water flow in the latex pipe was always blocked without leakage when water balloon pressure reached two atmospheres.
The reaction time of clamping was 2.47 ± 0.31 seconds (n = 10) and that of unclamping was 1.72 ± 0.26 seconds (n = 10). In the in vivo test, after water was injected into the balloon, the ischemia region of kidney appeared pale, indicating ischemia (Fig. 4A), while the kidney recovered its blood supply after the water was extracted (Fig. 4B). In the in vivo pig model, the reaction time of clamping was 3.10 ± 0.21 seconds (n = 8) and that of unclamping was 2.3 ± 0.32 seconds (n = 8). JZ laparoscopic clamp realized the blockage of artery in vitro and in vivo.
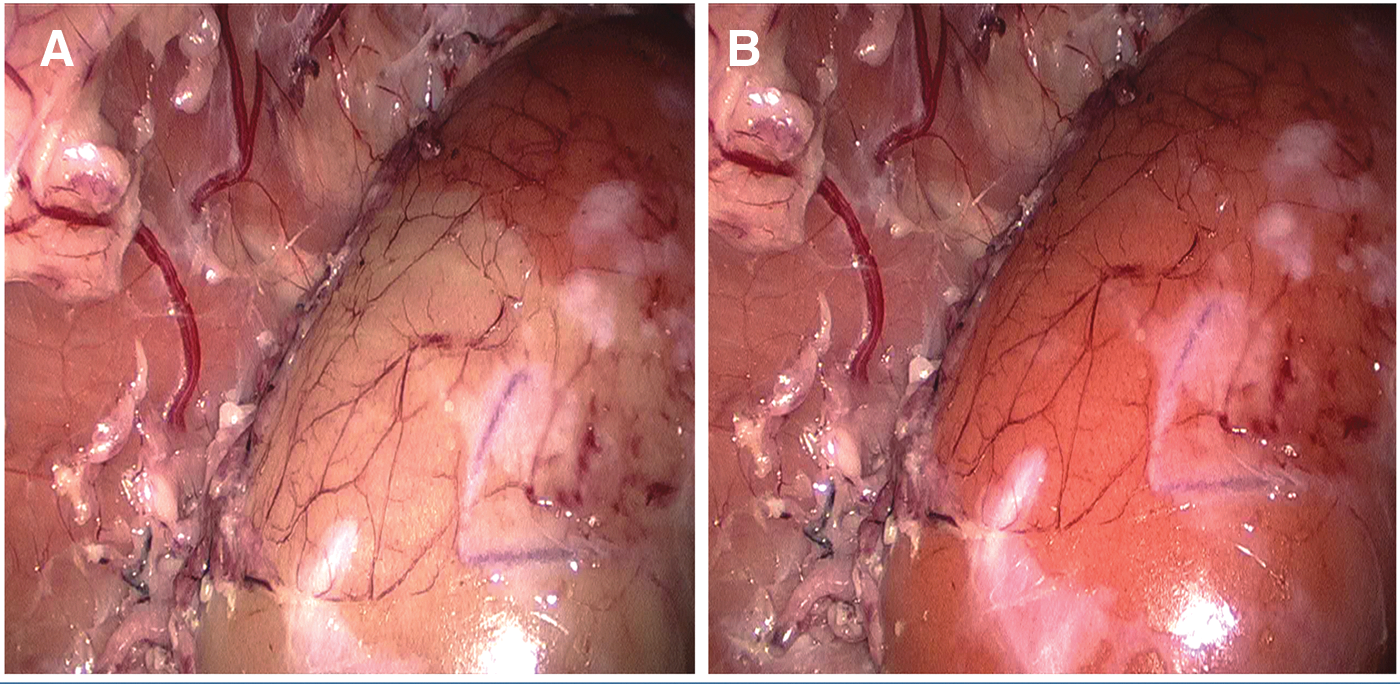
In vivo test of the work of the remotely activated clamp.
In the pig model, as the test group, eight cases involved the remotely activated bulldog clamp. The remaining seven cases involved the common standard laparoscopic clamp (JZ-XEC-250; Shanghai Medical Instruments (Group) Ltd., Corp.) as the control group. The weight of removed renal tissue in test group and control group was 5.81 ± 0.84 g (n = 8) and 5.38 ± 0.73 g (n = 7, p > 0.05), respectively. The mean operative time in the test group was 55.22 ± 6.12 min (n = 8) and in the control group was 52.57 ± 8.50 min (n = 7, p > 0.05) (Fig. 5A). The blood lost in the test group was 70.3 ± 6.59 mL (n = 8) and in the control group 67.0 ± 9.45 mL (n = 7, p > 0.05) (Fig. 5B). The weight of removed renal tissue, mean operative time, and blood lost was not significantly different between the groups (p > 0.05). The mean WIT in the test group was 19.0 ± 3.42 min (n = 8, which was significantly less compared with the control group (31.54 ± 5.23 minutes, n = 7, p < 0.05) (Fig. 5C). In the test group, the time for connection of the C-clamp was 53.6 ± 6 seconds (n = 8). Operator does not need to stop action for clamping or unclamping renal artery. So, the interruption time for blocking and unblocking renal artery during LPN was 0 (n = 8) and 0 (n = 8). It was significantly less compared with control group 58.7 ± 2 seconds (n = 7, p < 0.05) and 23.4 ± 1.9 seconds (n = 7, p < 0.05). To the pathologic investigation, after 30 min of clamping with the remotely activated bulldog clamp under 3 bar of atmosphere, the renal artery was removed for histopathologic examination (n = 2). Compared with the artery that was clamped by JZ laparoscopic clamp for 30 min (n = 2) and the unclamped renal artery (n = 2), no damage was detected on all of the artery walls (Fig. 6).
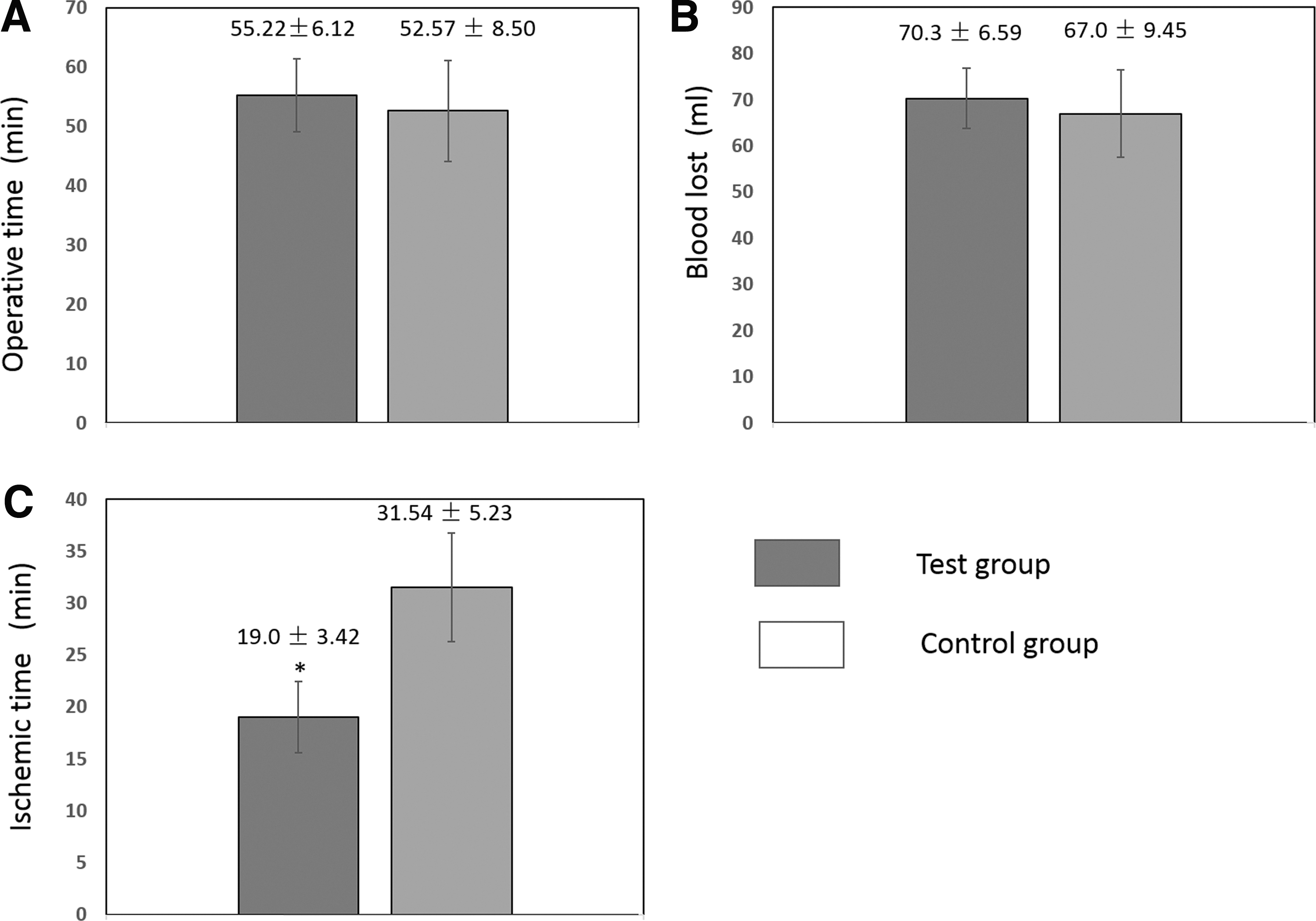
The mean operative time, blood lost, and mean ischemic time in the two groups.
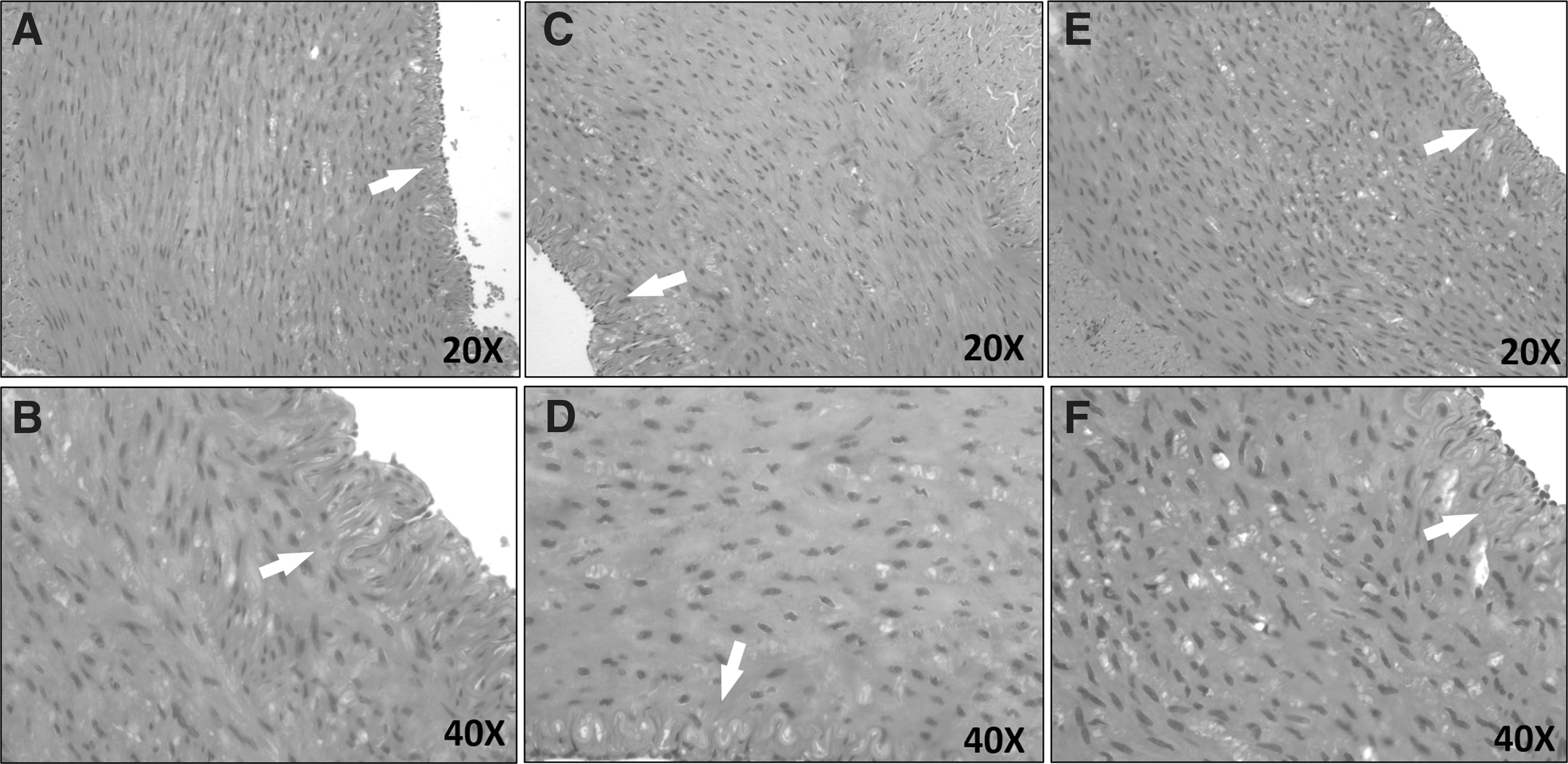
Histologic observation reveals that the renal arterial wall has not been injured after 30 min of clamping by the remotely activated bulldog clamp and standard clamp. The endothelium is indicated by the arrow.
Discussion
LPN is a standard procedure for treating small renal cancers, 1 of which exophytic renal masses <7 cm are ideal cases. 2 A bloodless field is essential for achieving the best surgical outcomes, and the conventional partial nephrectomy technique includes clamping of the renal artery. The side effect of this is renal ischemia, which can produce a certain level of ischemic damage to the kidney. It is reported that kidney damage occurs during LPN when the period of warm ischemia exceeds 30 min. This damage is only partially reversible. 3,4 Many studies have shown that each minute of ischemia is crucial in determining the extent of renal damage. 7,8 Thus it is important for urologic surgeons to introduce new techniques aimed at reducing WIT. 9,10
Clinically, to limit WIT during routine LPN, doctors should finish the operation as soon as possible. Some cases may not produce satisfactory results because of the rush.
In fact, during the first few minutes, the renal tissue is cut around the mass to be excised from the superficial without obvious bleeding. The frame of WIT is unnecessary. After the mass is removed and the severe bleeding stopped by suture and ligation, the subsequent time is for intensive suture and ligation. The frame of WIT is also unnecessary.
However, with contemporary vascular clamps, clamping and unclamping are difficult and time consuming during LPN. The renal artery must be clamped before LPN and unclamped after LPN, producing unnecessary WIT. Moreover, the existing vascular bulldog clamps have constant clamping force and pressure. 6 They cannot be applied to all cases. To avoid the above problems, we have designed a more advanced device, remotely activated bulldog clamp.
In our study, compared with the standard vascular clamp, the remotely activated bulldog clamp shows many advantages; with it is easy to clamp and unclamp, and the renal artery can be clamped and unclamped by remote activation as needed within 2 to 3 seconds. The interruption time for blocking and unblocking renal artery during LPN was zero. It means that the operator does not need to stop action for clamping or unclamping renal artery. More importantly, the device, outside of body, is controlled by an assistant without changing exposure to the partial nephrectomy excision site. So the doctor does not need to interrupt his action. This procedure is time consuming in LPN when using common standard bulldog. In our study, the clamping time and unclamping time of standard clamp are 58.7 and 23.4 seconds, respectively. This means that on demand clamping with standard bulldog clamp is impossible.
The advantage can spare all the above mentioned unnecessary WIT, as the WIT in the test group was significantly reduced. A recent study has indicated that partial nephrectomy with low ischemia times of <25 minutes had the same outcome as that of off-clamp LPN, 11 which further demonstrates the importance of reduction of WIT in LPN.
The newly-designed clamp can modify the applied pressure. The closing force at the middle part of the remotely activated clamp in our experiment was 1.02 kgf. However, the force of the remotely activated clamp does not directly act on the artery, the in-built water balloon controls the clamping and unclamping. In the present study, we set the blood pressure to 180 mm Hg, which is enough to block the renal artery of 180 mm Hg of blood pressure, when the pressure of water balloon reached two atmospheres. We also verified the in vitro test in a pig model.
According to the pathologic investigation, the remotely activated clamp has a big safety margin.
The device and study have some small limitations. The structure of kidney and renal artery of the pig are similar to those of humans and the object does a reasonably good job of modeling the real LPN. However, blood pressure and the inner diameter of renal artery are different between humans and the pig model. In the near future, we will test the optimal pressure to fit different blood pressures and modify the size of the clamp to fit different blood vessels.
Another limitation is the capillary tube. In theory, the capillary tube may get in the way of the surgery and cause pulling of the vessel. To avoid the situation, the puncture point should be far from and on the opposite side of the operative trocar. This could keep the capillary tube away from operative way and field of view.
After the test, the device showed high reliability, stability, and flexibility. WIT during LPN in pig model can be significantly reduced through using the newly designed remotely activated bulldog clamp. The novel design has obtained the National Invention Patent (No. ZL 2013 1 0572054.0). Nan tong Ecure Medical Technology Company is developing the novel product. As a kind of disposable Class II medical device, the remotely activated bulldog clamp will be inspected and issued a registration certificate by the drug regulatory agency of the government.
Footnotes
Acknowledgments
Ji-Feng Ding and Xiao-Peng Qin provided assistance in the animal experiment and production of the device. Dr. Trevor G. Cooper polished the English. The authors hereby express their thanks.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.