
Abstract
Background:
Ureteroenteric stricture occurs in as many as 15% of patients after cystectomy with urinary diversion. First-line management is typically percutaneous nephrostomy (PCN) drainage. We sought to compare costs of a urologic approach of retrograde stenting through flexible endoscopy and an interventional radiology (IR) approach of PCN and antegrade stenting using predictive modeling. The purpose of this study is to inform best practice for initial stricture management based on existing literature regardless of the benign stricture rate following radical cystectomy. Our hypothesis is that initial management by a urologist may be superior to IR management.
Materials and Methods:
The primary outcome measure was cost based on 2015 Medicare reimbursement rates by Current Procedural Technology codes with a secondary endpoint of number of procedures a patient undergoes. We developed a simulation model to replicate the experience of stricture patients. The model describes three arms: urologic management with retrograde stent placement, sequential management by IR, and single-stage IR management. We simulated 10,000 patients through the model with the percentage of patients pursuing each treatment arm and success rates chosen based on a review of relevant literature and clinic experience.
Results:
The average cost of urologic management is $703.23 compared with the average cost of $838.09 for patients using radiologic management. Within radiologic management, the average cost is $862.98 for sequential IR management and $639.44 for single-stage IR management. Patients would undergo an average of 2.53 procedures for those patients initially sent to urology and 2.91 procedures for those sent to radiology. For sequential IR, the average is 3.02 procedures, and for single-stage IR, it is 2.03 procedures. From a cost perspective, the success rate at which retrograde stent placement becomes worth attempting is 35%. If radiologic management is attempted initially, sequential IR management represents a cost-conscious option that limits the total number of procedures.
Conclusion:
The disparity in cost between IR and urologic management of ureteral stricture provides a rationale for rural practices that may not have immediate access to IR to manage the patient.
Introduction
R
Despite improvement in endoscopy, the gold standard of stricture repair is open reanastomosis. Definitive long-term management with open stricture repair has been repeatedly shown to be more effective than endoscopic approaches, with success rates of 76% to 90% for open repair vs 5% to 51.3% for various endoscopic techniques. 11 –13 To date, there have been no studies comparing initial management of ureteroenteric stricture; the first decompressive step that prevents kidney injury secondary to obstruction. Most studies comparing definitive management of stricture currently treat percutaneous nephrostomy (PCN) and antegrade stent placement as the standard of care for the initial management of stricture, while others documented success of passing a retrograde stent through an ileal conduit. 14,15 A limited number of studies examined the success rates of retrograde stent placement through ileal conduit with success ranging from 41% to 90%. 16 –18 Msezane et al. found that 58.5% (n = 24) of patients failed initial endoscopic management and required open repair. Of the 41 total patients treated with open repair in the study, 5 patients ultimately failed ureteral reimplant. 18 Finally, studies have examined the efficacy of antegrade nephroureteral stenting (NUS) with possible ballooning as a first step. 19,20
Given this landscape of options with hugely variable patient experience, costs, and access (availability of IR department and faculty, follow-up, etc.), we sought to examine initial management strategies for ureteroeneteric stricture. Specifically, we sought to explore the feasibility of retrograde stenting through the ileal conduit as a cost-conscious method of decompression that stays within the urologists' purview and does not leave the patient with percutaneous access. We developed a simulation model to compare the cost of a urologic approach (retrograde stent placement) with a radiologic approach (PCN and antegrade stent placement). Our hypothesis is that urologic management will be a cost-effective, safe effective method for initial management that spares patients percutaneous access. We sought to determine a success threshold at which it was comparable in terms of cost to attempt the urologic approach to inform best practices for initial stricture management following radical cystectomy.
Materials and Methods
A thorough literature review was done using PubMed searching within the English language literature for studies involving the following terms: “ureteral stricture,” “ureteroenteric stricture,” “stricture complications,” “success rates of stricture management,” “interventional radiology management of ureteral stricture,” “endoscopy of ileal conduit,” “endoscopic management of ureteral stricture,” “open repair of ureteral stricture,” and “percutaneous management of ureteral stricture.” The goal of this literature search was twofold: first to capture all of the different management strategies for the initial and definitive management of ureteral stricture and second to generate inputs for a simulation model that will allow for predictive analysis of various options. For inputs without literature to reference, we used our own single-center experience. Together, these inputs were used to generate a predictive model to describe the course of initial management of ureteral enteric stricture. Figure 1 shows a photograph of endoscopic wire intubation using a flexible cystoscope.
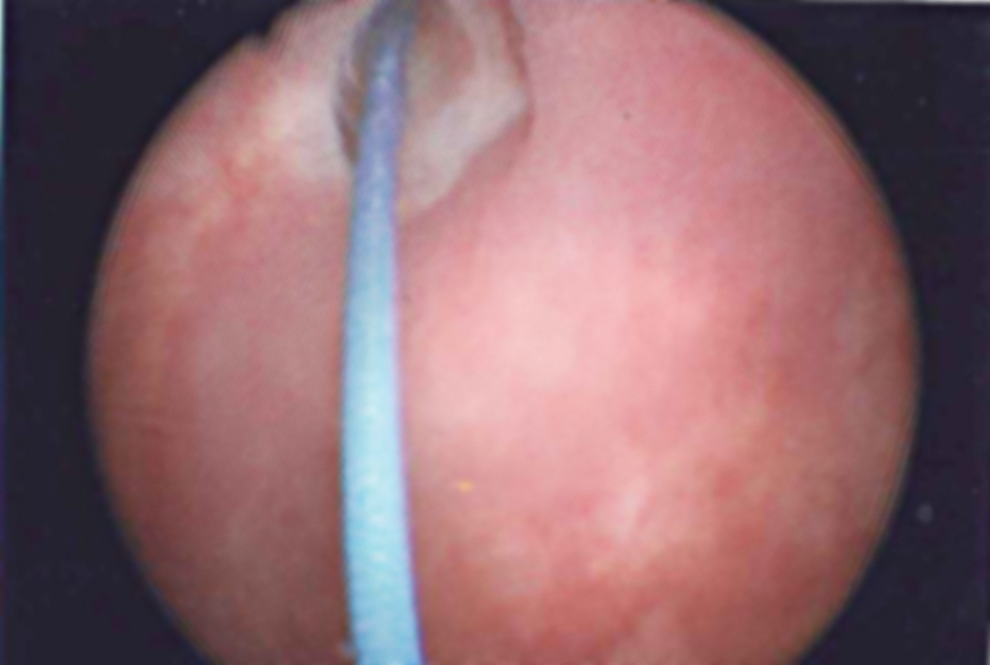
Three French wire intubations of ureteroenteric stricture by flexible cystoscopy.
Model
We developed a Monte Carlo simulation model to assess outcomes for stricture patients undergoing urology and interventional radiology (IR) management. We chose the Monte Carlo model over other predictive models due to the absence of a large database to inform outcomes for these procedures. We calibrated the model with outcome data from the literature as outlined above. We sought to provide data on an achievable endpoint to encourage the primary management of strictures by urologists. Specifically, we hoped to provide fiscal justification for attempted retrograde stenting in a minimal sedation setting with a urologist. The model was implemented using Arena Simulation Software (Rockwell Automation, Austin, TX). Ten thousand patients were simulated with 10 replications.
Figure 2 provides a diagram of the treatment paths for initial management. We define each of the three arms in the following manner: (1) urologic management with retrograde stent; (2) sequential management with IR: PCN, NUS with or without ballooning in separate encounters, and ureteral stent (henceforth sequential IR management); and (3) single-stage management with IR: initial NUS with or without ballooning and with or without coincident placement of PCN, which was eventually also converted to ureteral stenting (henceforth single-stage IR management). We modeled a practice pattern informed by assessing the body of literature in this area and used practice patterns of 10% undergoing urologic management, 80% sequential IR management, and 10% single-stage IR management. 21,22
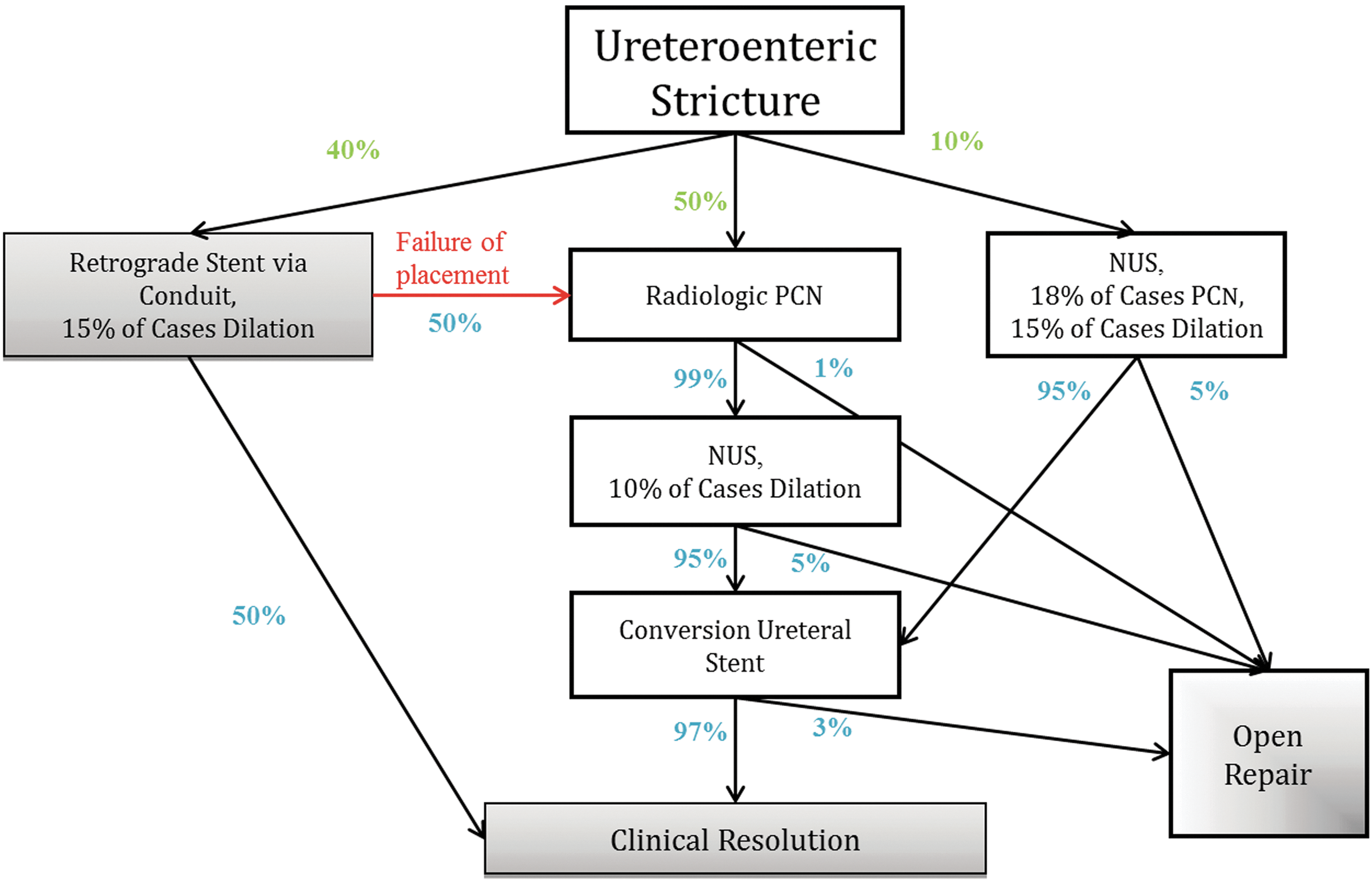
Initial management of strictures. The model describes clinical resolution (see Results and Discussions sections) as one of two possible endpoints resultant from the initial management of ureteroenteric stricture. The gray boxes represent avenues of treatment typically performed by a urologist, while the white boxes indicate procedures typically performed by radiology. Percentages drawn from literature are in blue, and the green percentages indicate the distribution of patient procedures based on our clinical practice patterns (see the Materials and Methods section). Current Procedural Technology coding is in corresponding Appendix Table 1. NUS, nephroureteral stent; PCN, percutaneous nephrostomy.
Costs
We used 2015A Medicare reimbursement rates to represent the costs of each procedure. 23 The full list of Current Procedural Technology codes used for each procedure is provided in Appendix Table 1. Costs for codes with modifier 59 were assumed to reduce unmodified costs by 25% based on institutional experience. The costs of each arm include variables such as 15% of cases in the single-stage arm receiving dilation. In other words, 85% of patients who went down this arm did not incur the additional cost of dilation, while 15% did and this increased cost for these patients was incorporated into the average per-patient cost for that arm. These additional costs are discretionary and the frequency at which we included them for each arm is depicted in Figure 2.
Probabilities
As shown in Figure 2, a patient enters the model with the development of a stricture and then proceeds down one of the three arms. The probabilities of proceeding down each arm can vary and represent the practice patterns outlined above (colored green). For the subsequent steps, the probabilities of moving to the next step (shown in blue) are derived from the literature. A full description of the percentages and their sources is shown in Table 1.
DJ = Double-J; f/u = follow-up; NUS = nephroureteral stent; s/p = status post.
Outcomes
Outcomes of interest were cost of initial management, the cost equivalence point where placement of the urologic retrograde stent was successful enough to justify its attempt, and expected number of patients who experienced severe renal decline during treatment. To find the point of cost equivalence, we varied the success of placement rate to determine how low this rate could be for it to still be optimal to initially try the urology management path. Sensitivity analysis was performed on the costs (±20%) in the model to determine if outcomes changed when these parameters were varied.
Results
A retrograde stent costs $263.35. Considering a 50% failure rate of retrograde stent placement, patients initially treated with urologic management had average costs of $703.23 (95% CI: $693.70–$712.76). Overall, patients who begin with radiologic management (sequential and single stage) incurred an average cost of $838.09 (95% CI: $836.99–$861.02). Sequential IR management generated an average cost of $862.98 (95% CI: $861.02–$864.94), while single-stage IR management generated a cost of $639.44 (95% CI: $635.33–$643.55). We also included a sensitivity analysis with a 20% variance in cost based on region and/or other factors. While the per-patient difference in expected costs between radiologic management and urologic management was $134.86 in the base case, this difference was reduced to $107.89 with 20% lower costs and was increased to $161.84 with 20% higher costs.
Given the cost differential between starting with urology management and starting with IR management, we sought to model the minimal success rate that would need to be obtained to justify trying to place a retrograde stent rather than sending the patient to get a PCN. The cost was calculated by averaging the total cost of patients who began with stenting while varying the success rate (red in Fig. 2). The cost, then, included patients who achieved clinical resolution from stent placement as well as those patients who went on to incur additional costs associated with sequential or single-stage IR procedures. As the success rate increased, the cost decreased (more patients managed by urologic stenting alone) as indicated in Figure 3. Stenting would need to be successful only 35% of the time to make management with urologic intent and radiologic management (sequential and single stage) cost equivalent. Any success over that rate (including the modeled 50%) would generate a cost gap between the urologic and radiologic management that would further favor starting with retrograde stenting.
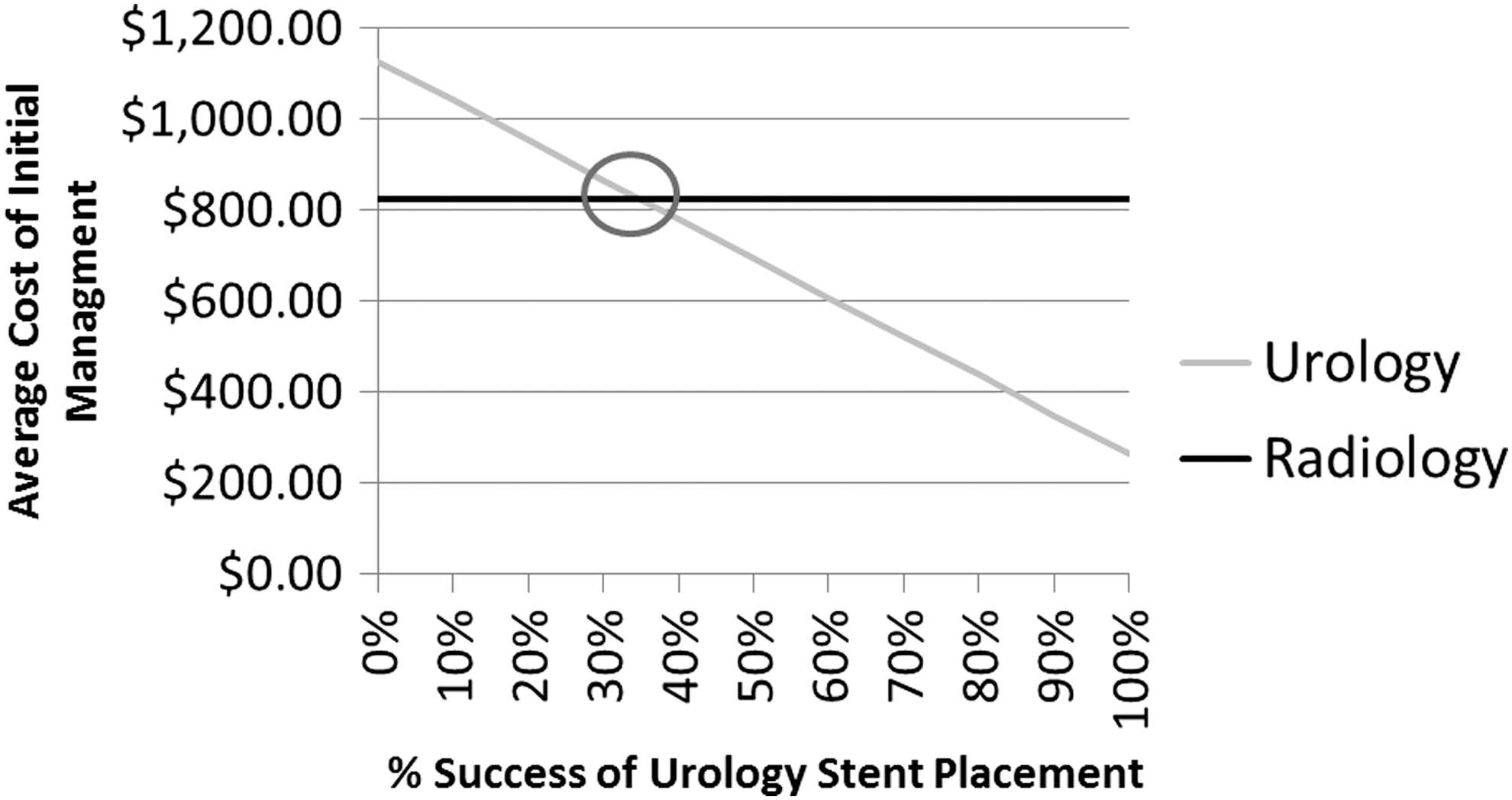
Cost as a function of success rates of urology stent placement. The solid black line indicates the cost for starting with either the sequential or single‐stage interventional radiology procedures (weighted average). The gray line indicates starting with urologic retrograde stent (urologic management), assuming various success rates of stent placement. The point of cost equivalence (circled) occurs when the success rate is 36%.
The model predicted an average of 2.53 procedures for those patients initially sent to urology and 2.91 procedures for those sent to radiology. For Sequential IR, the average is 3.02 procedures, and for single-stage IR, it is 2.03 procedures.
Discussion
Our study has several important implications. First, published literature of initial management of ureteroenteric stricture is highly variable and predominantly managed by interventional radiologists. It is important to differentiate the management literature from the more contentious literature surrounding stricture rates. 24 From the urologist's perspective, this is concerning as IR typically takes longer than urologic management and impairs the bladder cancer survivor's quality of life as the IR approach relegates the patient to having two bags. Second, the success rate required to justify retrograde stent attempt is lower than many practitioners may expect. The purpose of this study is to inform how and who should provide initial stricture management based on existing literature regardless of the benign stricture rate following radical cystectomy.
One of the concepts introduced in this article is the notion of clinical resolution following initial management of ureteroenteric stricture. We made this distinction based on two clinical conditions: relief from obstruction due to the stricture and no percutaneous access. Thus, if a patient is managed with PCN upon developing a stricture, this article considers their initial management complete when the PCN is converted to an indwelling stent and the patient no longer has nephrostomy access in their back. This distinction was made because of a focus on patient comfort and the natural clinical breakpoint that occurs when a patient no longer needs any urgent management. Such a patient with an indwelling stent now has options for definitive management and the clinical decision-making is quite different than it was when they were obstructed. Given that IR is typically done in staged procedures, this does introduce a bias toward making the initial management of strictures with IR more costly. Our data suggest that from a pure procedure cost perspective, single-staged IR management is the lowest cost. However, technically due to infection, edema, urine leak, and technical proficiency, single-staged IR management is not always an option. Patients have to undergo sequential IR management. Thus, we feel that a urologic approach is justified due to an IR approach leading to both increased cost to the patient and the increased number of procedures to achieve the same clinical endpoint.
We undertook the exercise of extrapolating our findings to a national level at the practice patterns modeled in the results as well as a practice pattern that would include a higher rate of urologic management, as seen at our own institution (40% urologic management, 50% sequential IR management, and 10% single-stage IR management). We estimated a high rate (10%) and a low rate (3%) of stricture for the 9000 cystectomies that are performed annually, assuming 90% of the management is currently PCN, which generated an annual cost of $197,905 for the low rate and $659,683 for the high rate. If trends shifted such that 40% of initial management was managed with retrograde stenting, there would be a 6.4% decrease in cost, with an estimated savings of $126,671 for low rate and $422,368 for high rate over 10 years.
One aspect of the model that we had hoped to incorporate was time to treatment. Unfortunately, there is incredible variability in timing based on availability of resources (IR and urology staff, operating rooms, procedure rooms, etc.) between different systems. One study in Greece found that there is an average of 12.5 days between diagnosis of stricture and intervention by radiology. 25 This result was drastically different from our own institution, which will place a PCN on the same day of diagnosis. There is also considerable time variation between the steps of management. For the sequential IR procedures, it was reportedly typical to have 4 to 6 weeks between steps, also a scenario familiar to us at our institution. 19 Other studies demonstrated that many patients will undergo stent replacement on a 4- to 6-month basis, with as many as 44% of patients undergoing such stent exchange until death after a 26-month follow-up. 15,20
We term our analysis cost-conscious intentionally. While we believe it is also cost-effective, a major limitation of our work is an inability to capture the concomitant cost of anesthesia, operating room versus procedure room cost, and overnight stay. At our institution, we are able to place the retrograde stent without anesthesia in our clinic fluoroscopy room or in the outpatient surgery center. PCN placement is done in a procedural IR suite and requires conscious sedation. Not only do these additional steps generate little ultimate value to the patient but they are also expensive. Additionally, the cost variability is further complicated by the jurisdiction of care. Military, academic, and community hospital settings in addition to regional differences in cost introduce variables that are not controlled for in this study. Despite this, as the costs are based on Medicare reimbursement, we believe the cost difference we generated in the model is a conservative estimate of the true cost savings that could be realized as most IR procedures will require an overnight stay, longer fluoroscopy charges, and sedation charges that would offset or supersede the OR charges associated with the urologic approach.
Urologist skill at endoscopic instrumentation is not captured fully in our simulation model. We used a 50% success rate in the base case based on both the literature and our experience. We performed sensitivity analysis on this value to account for skill leading to decreased success and found 35% to be cost equivalent. This seems a reasonable expectation for a urologist in the current endoscopic climate. Another limitation is that any quality of life benefit for the patient time is similarly not captured. There are mixed data on the patient quality of life and patient satisfaction of PCN versus indwelling stent. However, the body of literature across multiple specialties has repeatedly demonstrated that minimizing patient wait time and need for follow-up are associated with increased satisfaction. 26 In the setting of a ureteral enteric stricture, we believe that urologic management will offer fewer procedures and generally a decreased wait time.
The intent of treatment of strictures is to preserve kidney function. Bladder cancer patients usually have poor general health associated with smoking and have been exposed or have the potential to be exposed to nephrotoxic chemotherapy. One advantage of an initial urologic management is that the patient stays under the care of the physician most cognizant of these risks. In a small study, two patients of 25 patients with benign ureteral stricture ultimately had ipsilateral nephrectomy as final treatment. 27 Indeed that study largely comprised patients with stone disease who may be in better health than survivors of bladder cancer. Recent surveys indicate that 70% of radiologists are generalists, while the remaining 30% are subspecialists. Rural hospitals are more likely to support general diagnostic radiologists rather than subspecialists. 28 Instead of having the patient travel for IR care, an attempt at initial management can be made.
For the purposes of our article, we did not differentiate between success per ureter versus success of treating the patient given the low likelihood of bilateral ureteral strictures. We consider the inability to differentiate between Bricker and Wallace anastomoses as a limitation of this study, but assume that repair will be applicable to both. Another limitation is that the inputs are overwhelmingly from centers of excellence where the studied method was analyzed retrospectively. Given that management of ureteroenteric stricture is presumably being treated at high-volume centers, the quoted success rates within the model should be considered realistic.
Another limitation of this article is that our results are based on simulated outcomes rather than observed clinical outcomes. While no model is a perfect representation of reality, the model parameters are based on our current knowledge of success rates found from a thorough search of the literature.
Conclusions
Patients with an ileal conduit status postcystectomy who develop anastomotic stricture should be considered for initial urologic management with retrograde stenting if a threshold level of success (35%) can be reached. This represents potential cost savings to the system and benefits to the patient, including time and need for further interventions.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
| Procedure | Codes | Total cost |
|---|---|---|
| Retrograde stent through conduit | ||
| No dilation (85% of cases) | 44380, 52332 | $230.26 |
| Dilation (15% of cases) | 44380, 52344 | $450.87 |
| NUS | ||
| No dilation or PCN (67% of cases) | 50393, 74480 | $318.21 |
| PCN (18% of cases) | 50393, 50392–59, 74480, 74475–59 | $526.84 |
| Dilation (15% of cases) | 50393, 52344, 74480 | $699.00 |
| Radiologic PCN | 50392, 74475 | $278.17 |
| NUS | ||
| No dilation (90% of cases) | 50393, 74480 | $318.21 |
| Dilation (10% of cases) | 50393, 52344, 74480 | $699.00 |
| Conversion ureteral stent | 50387, 50389 | $158.03 |
| Open repair | 50800 | $951.08 |
Costs are based on 2015A Medicare reimbursement rates.
IR = interventional radiology; NUS = nephroureteral stent; PCN = percutaneous nephrostomy.