
Abstract
Background:
Residual retroperitoneal masses in NSGCT need postchemotherapy retroperitoneal lymph-node dissection (PC-RPLND). Open (O) PC-RPLND is a standardized procedure, but morbidity is not negligible and mostly attributable to laparotomy. Laparoscopic (L) PC-RPLND may improve tolerability profile. We evaluated viability, toxicity, and short to medium-term oncologic outcome of L-PC-RPLND following well-defined selection criteria.
Patients and Methods:
Since February 2011, consecutive patients with a unilateral residual mass (≥1 cm or growing), normalized markers, and limited encasement of inferior vena cava and/or aorta were candidate to unilateral L-PC-RPLND. Surgical performances, histology, hospital stay, complications within 30 days, and survival were recorded. Patients were regularly followed up. Adjuvant chemotherapy was not provided.
Results:
Sixty-seven patients (stage IIA = 14; IIB = 41; IIC = 7; III = 5), representing 29% of all those candidate to PC-RPLND in this time frame, underwent L-PC-RPLND up to August 2015. Median size of the mass was 27 mm (interquartile range [IQR] 15–31). Median operative time was 234 minutes (IQR 184–250). Three procedures were converted to open surgery. Mean hospital stay was 3 days (IQR 2–4). Out of three (4.5%), one grade III (lymphocele requiring drainage) complication occurred. Sixty-six (98.5%) patients maintained antegrade ejaculation. Histology revealed teratoma in 76%, fibronecrotic tissue in 21%, and viable cancer in 3% patients. All patients are alive and event free after a median follow-up of 21 months (IQR 10–30).
Conclusions:
In a referral center, L-PC-RPLND is a transferable option for a proportion of patients with a residual mass. Tolerability is acceptable, and current oncologic outcome is consistent with a safe oncologic profile.
Introduction
T
Following completion of first line cisplatin-based chemotherapy and normalization of serum tumor markers, a residual retroperitoneal mass is present in at least 50% of patients with metastatic nonseminomatous GCT (NSGCT). As a rule, postchemotherapy retroperitoneal lymph-node dissection (PC-RPLND) is indicated in case of incomplete radiologic remission (i.e., a residual mass of 1 cm or greater) and normalized serum markers. 2 –4 In these patients, RPLND reveals necrotic debris and fibrosis, teratoma elements, or viable tumor in ∼40% to 50%, 30% to 40%, and 6% to 20% of patients, respectively. 5 Unfortunately, CT or MRI does not accurately predict histology, and fluorodeoxyglucose positron emission tomography (FDG-PET) does not improve accuracy of conventional staging. 6
RPLND is traditionally performed using an open approach. Open (O)-PC-RPLND is associated with precise morbidity, especially in terms of hospital stay, analgesics need, prolonged ileus, and time to full recovery. In addition, it requires a large incision that is cosmetically unfavorable in these mostly young patients. Laparoscopic RPLND was introduced as an alternative approach for stage I disease. Subsequently, it has been applied as a therapeutic approach in higher stage patients in the postchemotherapy setting. 7
In this study, we present our experience with laparoscopic (L)-PC-RPLND in selected NSGCT patients with a clinically relevant residual mass, to evaluate systematic feasibility, safety, and efficacy.
Patients and Method
Study approval
This study was approved by the local ethics committee (INT 60/16).
Patient selection
Starting in February 2011, we standardized the use of L-PC-RPLND in selected patients following chemotherapy for metastatic NSGCT. Criteria for L-PC-RPLND included the following: no previous retroperitoneal surgery (excluding biopsy), unilateral disease since the beginning, a residual lesion between 10 and 50 mm at cross-sectional CT imaging, markers normalization following completion of chemotherapy, and encasement of the residual mass in respect of inferior vena cava (IVC) and/or aorta, not exceeding 30% of their circumferences. In case of cystic lesions, suggestive of containing prevalent teratomatous elements, residual masses larger than 50 mm could be considered.
Surgical technique
Patients are placed in a semiflank position (45°) on the side of the disease. Following pneumoperitoneum creation through an open technique, intra-abdominal CO2 pressure is maintained at 13 mmHg. A four-port diamond-shaped transperitoneal approach is performed (one port placed paraumbilical for the camera; two pararectal trocars—subcostal and iliac—, and one trocar, along the anterior axillary in the same line of optical trocar). For right dissection, a fifth 5-mm trocar is sometimes placed in the epigastrium to permit elevation of the liver through the use of a divaricator or a grasper (Fig. 1). The colon is extensively mobilized to expose the great vessels. The semiflank position and the operating table tilt allow viscera to fall down. Once the retroperitoneum is exposed, the residual mass and its relations are verified. Dissection starts at the arterial iliac bifurcation and goes upward to the renal artery. Dissection (Fig. 2) duplicates the open approach and includes interaortocaval, preaortic, retroparacaval, and common iliac nodes for right RPLND and paraaortic, preaortic, retroaortic, and common iliac nodes for left RPLND, as reported by Donohue 8 and Pizzocaro. 9 Usually, nerve sparing is achieved through exclusion of contralateral sympathetic fibers. Spermatic vessels and funicular stump are removed. Preparation is performed with unipolar scissors and bipolar forceps. Dissections are performed with ultrasonic energy platform (Ethicon Ultracision Harmonic Scalpel ® , Johnson & Johnson) or with ultrasonic and advanced bipolar energy platform (Thunderbeat ® , Olympus) and through cold scissor cut. Lymphatic ligation is assured with Weck ® Hem-o-lok ® clips. The specimen is retrieved with an endoscopic bag. A drain tube is left in retroperitoneal space until secretion reduces (<100 mL/day).
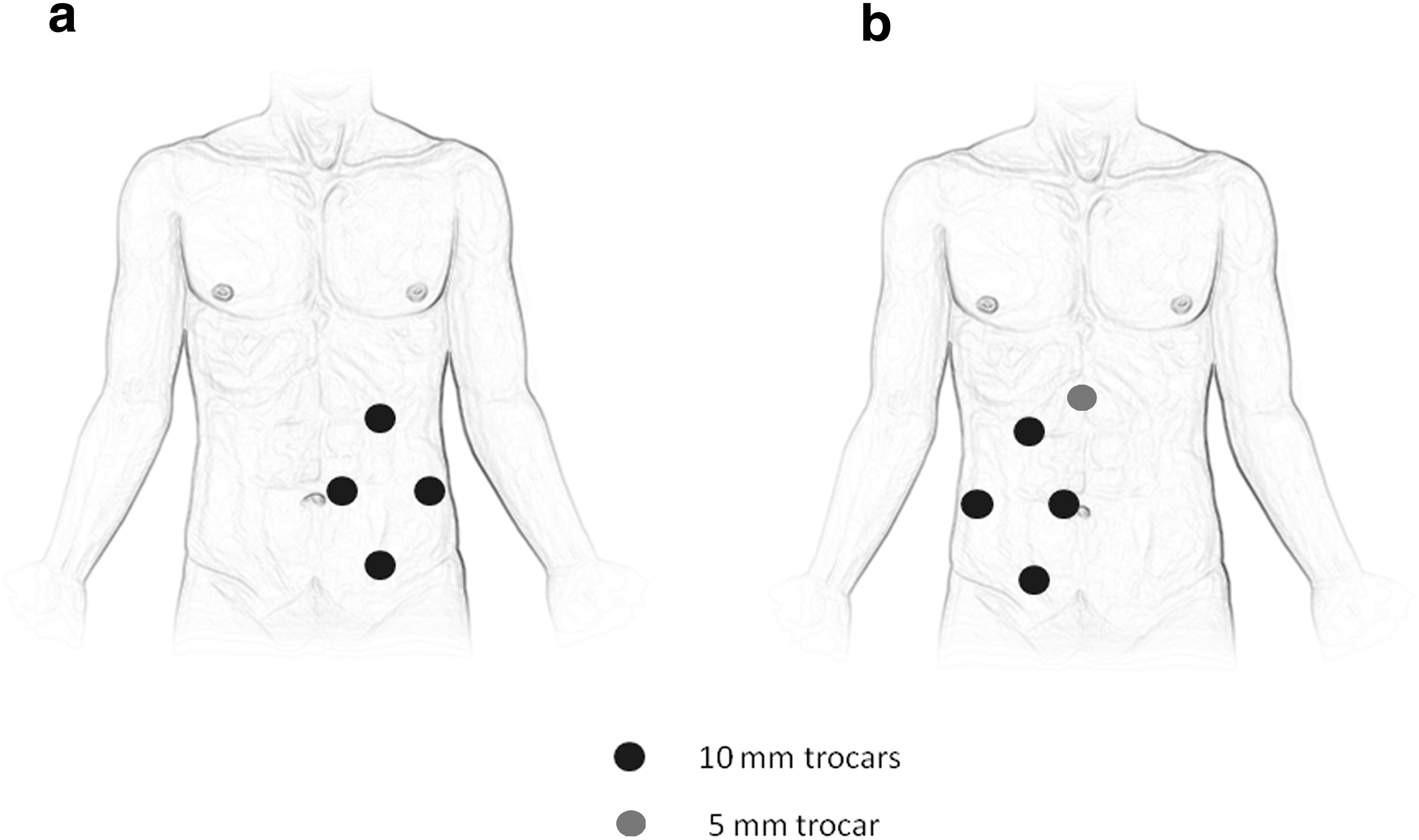
Trocar positioning in left

Laparoscopic vision of right retroperitoneal dissection.
Postoperative management
Nasogastric tube is removed at the end of the procedure. Oral fluid and solid intake started on the first day after surgery, and patients are mobilized as soon as possible (usually in day 1). Bladder catheter is removed in day 1 or 2. No adjuvant therapy was provided in case of viable cancer at definitive pathology.
Follow-up
Patients were regularly followed every 3 months and interviewed concerning maintenance of ejaculation.
Data collection and analyses
A prospective database has been created to include patients undergoing L-PC-RPLND. The data set contains the following: patient name, hospital identification code, age, prognostic category, and stage before chemotherapy according to the International Germ Cell Consensus Classification (IGCCC), 10 type of chemotherapy and number of courses, size of residual disease measured at cross-sectional CT scans, marker status before surgery, surgery date, extent of surgery, surgeon, operation time, intraoperative complications as described in the surgical report, histology of the residual mass, hospital stay, postoperative complications within 30 days since the discharge, and follow-up schedule with status of the patients at the last visit, including information about antegrade ejaculation.
Size of the disease before chemotherapy was added subsequently, and it is not available in all cases.
As a standard of our surgical theatre records, blood loss was not quantified if it does not exceed 100 cc.
Complications have been classified according to the Clavien–Dindo classification. 11
Survivals were descriptively reported.
Results
Between February 2011 and August 2015, out of a total of 233 PC-RPLND performed for a residual retroperitoneal mass only (subjects who needed additional procedures were excluded), 67 (28.8%) patients with a mean age of 27.5 years (range: 17–45 year) underwent L-PC-RPLND, by two surgeons (one performing the vast majority of procedures). Table 1 depicts the general characteristics of the study population. Of interest, the vast majority (62%) belonged to IGCCC good risk category, left dissections were more frequent (43 vs 24), 12 (17.9%) patients had bulky (stage IIC-III) disease, and the median size of the residual mass was as large as 27 mm (interquartile range [IQR] 15–31) while the prechemotherapy median diameter was 30 mm (IQR 20–35 mm), in 53 (79.1%) patients where this parameter was assessable.
Available in 53 patients.
IGCCC = International Germ Cell Consensus Classification; IQR = interquartile range; RPLND = retroperitoneal lymph-node dissection.
Operative and postoperative parameters are reported in Table 2A and 2B, respectively. Median operative time was 15% longer for right dissections. Three conversions occurred (all had stage IIB disease): one due to a renal vein injury and two were decided because of extended desmoplastic encasement of the residual mass to aorta and IVC, respectively, and they were judged not be safe to continue through laparoscopy. Median postoperative hospital stay was 3 days (IQR 2–4). Postoperative complications (Table 2B) were as follows: a grade II event consisting in a blood loss (800 mL) requiring transfusions of two units of packed red blood cells following the renal vein injury, and a grade IIIa event consisting in a postoperative lymphocele formation, requiring a percutaneous drainage. Antegrade ejaculation was maintained in 66 (98.5%) patients: the one who reported loss of antegrade ejaculation had undergone a dissection at iliac bifurcation.
IVC = inferior vena cava; LAE = lack of antegrade ejaculation.
Table 2C reports on histologic findings and oncologic outcomes. It is relevant that about three quarters of these patients had teratoma.
No patient relapsed following a median follow-up of 21 months (IQR 10–30).
Discussion
PC-RPLND is indicated after primary chemotherapy in case of a residual mass ≥10 mm, even if the mass has shrunk and markers normalized. 12 PC-RPLND remains a highly complex procedure, where complications are more frequent and more severe than in clinical stage I. 13
Mini-invasive surgery of the retroperitoneum has been advocated, aiming to reduce morbidity in these young patients. Nonetheless, L-PC-RPLND can be standardized once it can be demonstrated that (1) an important proportion of patients with a clinically relevant residual mass (i.e., of at least 1 cm) may be effectively treated with mini-invasive approach, (2) safety and tolerability of the procedure improve in respect of open surgery, and (3) oncologic outcomes are comparable with open counterpart. 14 –16 We are confident that our series may represent a contribution in favor of L-PC-RPLND, mainly for the first and partially for the second issue, and the results are consistent with the principles of oncologic safety.
Patients undergoing L-PC-RPLND represent about one third of those candidate to standard PC-RPLND and have been recruited in a relatively short period, apparently shorter than those reported in the recent literature. In other words, in our practice, L-PC-RPLND is not a special performance, but a systematic slot in the flowchart of testis cancer management. We believe that this is of paramount importance, as it demonstrates the standardization of L-PC-RPLND in our work.
The effective size of residual masses is another important issue to further support the opinion to include L-PC-RPLND within the indication of surgery in testis cancer management. In our experience, the median size is 27 mm. This datum can be favorably compared with four of the series reported in Table 3, while other authors, although they have important numbers, included many patients with residual masses below 10 mm. 15,17 –22 Actually, we submitted to L-PC-RPLND those patients who would be incontrovertibly candidate to postchemotherapy surgery. We had only one patient presenting a mass of 8 mm: he had a late relapse of postpubertal teratoma after complete remission.
Extent of dissection: unilateral vs bilateral dissection (as reported by the authors).
Diameter of nodal mass before chemotherapy.
Diameter of nodal mass before RPLND.
One patient had primary retroperitoneal disease.
Ca = viable cancer; FN = fibronecrotic tissue;
One frequent limitation of laparoscopic RPLND, compared with open counterpart, is bilateral dissection. A laparoscopic bilateral dissection usually requires patient repositioning during the operation with a longer operative time. Just considering the series where both unilateral and bilateral dissections were performed, bilateral dissections were from 50 minutes 21 to 100 minutes 15 longer than unilateral ones. Recent experiences with robot-assisted laparoscopy showed that the time needed for repositioning could be spared, leading to a reduced operative time. 22
Our indications to unilateral dissection do not change according to approach, if laparoscopic or open, and are in line with recommendations stated by the European consensus 12 and by the recent EAU guidelines. 2
O-PC-RPLND is associated with considerable morbidity, typically in terms of hospital stay and time to full recovery as a consequence of laparotomy. It has been shown that the complication rate of O-PC-RPLND remains considerable (up to 51.9%), even in experienced hands. 23
In general, the most known advantages of laparoscopy include reduced blood loss, shorter hospitalization, a faster convalescence, a better cosmetic result, and a lower need of postoperative analgesics. 14 –16 In comparative analysis between L-RPLND and O-RPLND in stage I NSGCT, L-RPLND resulted to be superior in terms of complication rate, hospital stay, with no apparent worse outcome in terms of need of subsequent chemotherapy. 24 Another small series compared L-RPLND vs O-RPLND in stage I NSGCT and found better QoL performances following L-RPLND. 25 A particular favorable tolerability profile with L-RPLND in the prechemotherapy setting has been recently shown. 26
However, the postchemotherapy setting differs from stage I for many aspects, but high-level comparative studies are not available. One small study reported significant shorter durations both of drainage tube and hospital stay in patients undergoing L-PC-RPLND when compared with those undergoing O-PC-RPLND. 27 In our experience, the mean hospital stay is 5 days longer following O-PC-RPLND. Nonetheless, a reliable comparative analysis between open and L-PC-RPLND is hard to plan, due to potentially confounding factors, which include indications and extent of disease.
Most of the complications we recorded were minor (Clavien–Dindo ≤2) (Table 2B). A feared intraoperative complication is major vessel injury, which may lead to rapid open conversion. Open conversions remain however infrequent, grossly under 5% in recent series (Table 4), where experience of surgeons plays a fundamental role. The risk management for intraoperative significant bleeding requires a multistep approach that includes accurate selection of patients, intraoperative evaluation of the risk of an uncontrollable bleeding, rapid interpretation of the severity of the damage, adequate laparoscopic expertise in vascular suturing, and prompt and safe conversion to open surgery when it is necessary. Actually, out of the three conversions we had, two were decided when no accident had occurred, as we judged that the risk of a bleeding would have been difficult to manage, due to the extreme adhesion of the mass with IVC and aorta. Nonetheless, cautious dissection of masses infiltrating or adhering gross vessels is possible in selected cases, as reported by Aufderklamm 28 and experienced in our series.
The postoperative complications of L-RPLND differ from those of open surgery. Wound infection and ileus are exceptional in the laparoscopic setting, while chilous acites, complicated lymphoceles and prolonged secretion are more frequent. These events were reported, 17 and could be severe. 15 We had no chylous ascites, but we recorded a lymphocele formation requiring subsequent drainage in one patient. We are confident that meticulous ligation with clips (we currently use the Hem-o-Lock ® clips) remains the best way in preventing prolonged secretion, lymphocele formation, and ultimately ascites.
The oncologic outcome following L-PC-RPLND is still imperfectly defined, due to the paucity of data. The proportion of recurrences is low, but this still depends on (1) the favorable characteristics of these patients, as the vast majority of patients show small- or medium-size unilateral masses and good prognosis disease, (2) the insufficient length of follow-up, which does not permit to figure out the efficacy in the long term.
Available data basically demonstrate that mini-invasive RPLND is capable of inducing the disease-free status in this particularly favorable setting of patients, with no excess of early recurrences attributable to incomplete resection (Table 3). Nevertheless, retroperitoneal and in-field relapses have been reported. 21 Eventually, retroaortic and mainly retrocaval dissections were not done in some centers at the beginning of their experiences, 19 which may explain some of these recurrences. Data from stage I disease seem to reassure that there is not an excess of in-field recurrences in pN0 patients, leading to consider that unstaged nodes do not remain in the retroperitoneum. 24,26 Numbers and observation periods, however, are now sufficiently comfortable to be confident in continuing recruitment of patients for this less aggressive surgery, waiting for a sufficiently long follow-up to support its equivalence with open surgery.
We are aware that L-PC-RPLND cannot replace open surgery in all the patients with a residual mass. In the frame of our study, L-PC-RPLND was 28.8% of all PC-RPLND. Large residual masses, those extensively infiltrating or encasing gross vessels and those situations where a complex adjunctive surgical procedure is needed, are not currently suitable for mini-invasive surgery. Selection criteria may affect the results: actually, the majority of patients in our series had residual teratoma. This figure exceeds the expected figure of 50% and reflects the adoption of specific criteria.
On the other hand, any criteria for L-PC-RPLND cannot be thought as definitive and un-negotiable, as technology and surgeon skill evolve and will allow new frontiers of application, exactly as it has taken place in these years. The limit of unilateral dissection is probably one that may be overcome. Bilateral dissections are possible through laparoscopy, as documented by different experiences. The issue is how to improve the approach of bilateral dissection, by reducing operative time, essentially due to patient repositioning. Robotic-assisted RPLND may represent one answer. Unfortunately, we have not yet substantial and convincing data on robotic PC-RPLND, as the few available articles essentially address primary RPLND, 28,29 while a recent series was not able to individuate any advantage of robot-assisted PC-L-RPLND in comparison with the pure laparoscopic approach. 30
Conclusions
L-PC-RPLND requires experienced surgeons, but represents a systematic alternative to open surgery in selected patients. This approach permits advantages in terms of postoperative morbidity. Current oncologic results allow in proceeding with L-PC-RPLND, but confirmative long-term data are needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.