
Abstract
Purpose:
We developed a polyethylene sack (the PercSac) that fits over the shaft of a rigid nephroscope and is deployed into the collecting system to capture a stone and contain fragments during percutaneous nephrolithotomy (PCNL). We previously reported our results using the PercSac in a percutaneous cystolithopaxy model. In this study, we compare the efficiency of stone fragmentation with and without the PercSac in an anatomically correct in vitro PCNL model.
Materials and Methods:
The PCNL model consisted of a human collecting system model created on a 3D printer. Ten BegoStones made in spherical molds of 2.0 cm diameter, matched for weight, were fragmented in the model using a 24F rigid nephroscope and an ultrasonic lithotripter, including five with and five without the PercSac. The total times for stone fragmentation and complete stone clearance, gross assessment of the stone-free status, and need for flexible nephroscopy to achieve a stone-free state were recorded.
Results:
The median time for stone fragmentation was significantly shorter in the PercSac group compared with the control group (217 seconds [IQR = 169–255] vs 340 seconds [IQR = 310–356], [p = 0.028]). Likewise, the total time for complete stone clearance from the kidney was significantly shorter for the PercSac group (293 seconds [IQR = 244–347] vs 376 seconds [IQR = 375–480], [p = 0.047]). In one trial with the PercSac, residual dust remained in the kidney, while in all five trials without the PercSac small residual fragments remained. All trials without the PercSac required flexible nephroscopy with basket extraction to become stone free, while none of the trials with the PercSac required flexible nephroscopy for stone clearance.
Conclusions:
Ultrasonic lithotripsy using the novel PercSac stone entrapment device is more efficient and efficacious than traditional ultrasonic lithotripsy in an in vitro PCNL model. The advantage may be even more pronounced during clinical PCNL where residual fragments migrate into difficult-to-access calices. Further in vivo testing is underway.
Introduction
P
In an effort to increase the likelihood of a true stone-free outcome for PCNL and, thereby, maximize the success of the procedure, we developed a polyethylene sack (termed “PercSac”) that is used with a rigid nephroscope to entrap and contain a stone and its fragments completely during ultrasonic lithotripsy. We previously published our results on the feasibility and efficacy of the PercSac in an in vitro cystolithopaxy model. 8 PercSac deployment was easily accomplished in this less physically restrictive model, and cystolithopaxy with the device was associated with a faster stone fragmentation time and higher stone-free rate than traditional cystolithopaxy without the device. 8 In this study, we sought to evaluate the use of PercSac in an anatomically correct in vitro PCNL kidney model and assess the efficiency of stone fragmentation with and without the device.
Materials and Methods
The PercSac as previously described 8 is a polyethylene sack with an open, cinchable distal end that is secured over the shaft of a rigid nephroscope (Fig. 1). The nephroscope/PercSac assembly can then be passed through a 24 or 26F Amplatz working sheath into the collecting system. Grasping forceps passed through the working port of the nephroscope are used to draw a stone into the pouch through the open distal end, which is then cinched closed by way of a Nitinol wire threaded around the circumference of the distal end of the pouch, enabling the stone to be captured within the sack. The grasping forceps are then disengaged from the stone, and an ultrasonic lithotripter is passed through the working port of the nephroscope and onto the stone within the cinched PercSac pouch. The stone is fragmented using ultrasonic lithotripsy and the fragments generated are suction evacuated from the cinched pouch, thereby preventing migration of fragments throughout the collecting system (Fig. 2). The proximal end of the PercSac is located on the portion of the nephroscope outside the body and while it fits snugly on the scope the proximal end is open allowing for efflux of irrigation fluid and maintenance of a low-pressure space within the device. Once the majority of fragments have been evacuated from the pouch, the PercSac and its contents are removed from the kidney through the nephroscope sheath.
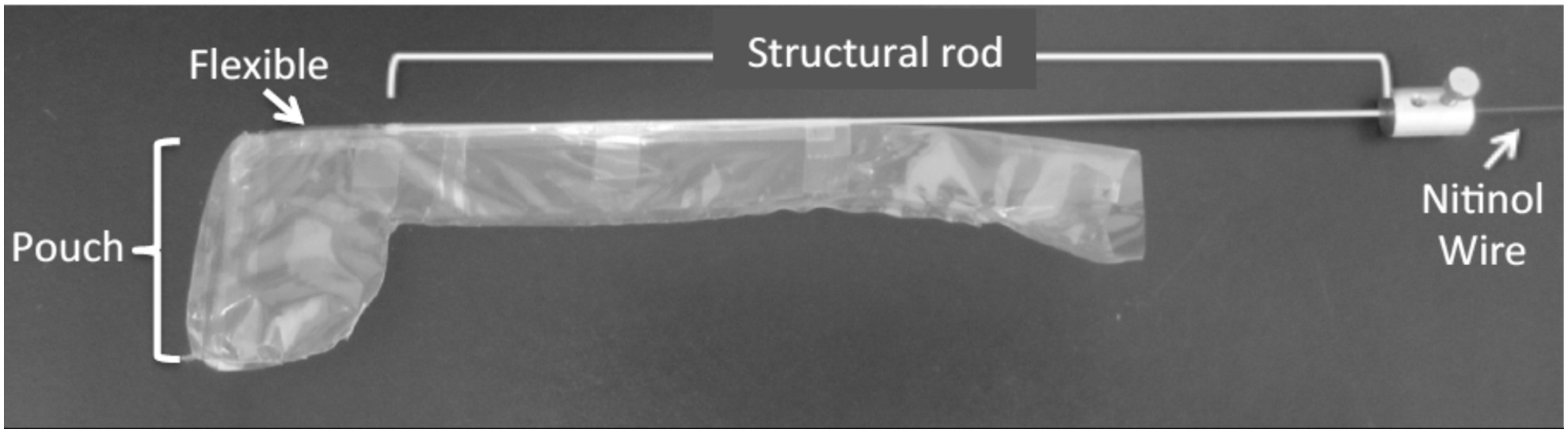
The height of the PercSac pouch is 40 mm and the diameter is 32 mm (circumference = 100 mm) allowing capture of as much as a 2.5 cm stone. Pulling on the Nitinol wire that runs through the structural rod cinches the circumference of the distal pouch closed. The stainless steel structural rod is terminated where the neck transitions into the dome-shaped pouch. A polyurethane flexible tube is attached from the distal end of the structural rod to the opening of the pouch.

The in vitro PCNL model consists of a collecting system with dimensions consistent with that of a human kidney (renal pelvis 9.0 × 5.5 cm). SolidWorks (Dassault Systemes, Waltham, MA), a 3D design, simulation, and validation software package was used to create the kidney model out of ABS filament material, and it was printed on a Stratasys Dimension BST 1200es 3D printing machine (Stratasys Dimension, Eden Prairie, MN). The upper pole calix, renal pelvis, and proximal ureter are hollow to accommodate a nephroscope, while the interpolar and lower pole calices are solid and therefore impassible with an endoscope. The upper pole calix is open to allow passage of the nephroscope into the collecting system. The kidney was fixed in place with the calices facing up and a 30F Amplatz working sheath (Boston Scientific, Marlborough, MA) secured into an upper pole calix using a 12 mm laparoscopic trocar diaphragm. An opening in the renal pelvis sealed with a rubber stopper was used as the entry point to place stones within this model (Fig. 3).
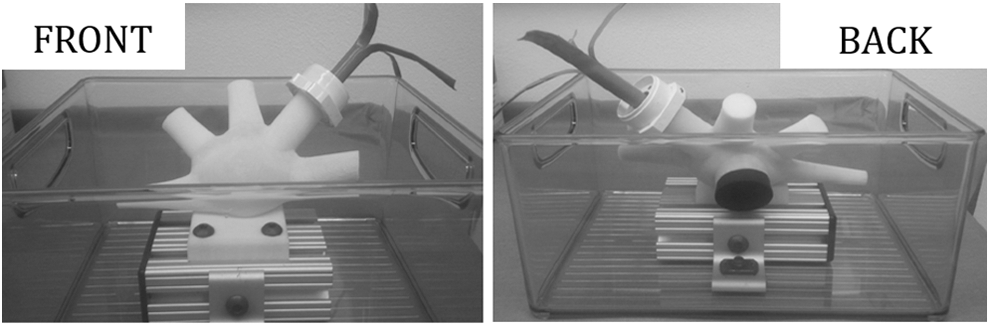
The PCNL model printed on a 3D printer using the dimensions approximating the size of a human kidney. A 30F sheath is placed through an upper pole calix. A stone can be placed into the model through the opening in the back that remains water tight with a circular rubber stopper. PCNL, percutaneous nephrolithotomy.
One stone was placed into the renal pelvis for each of five trials with and five trials without the PercSac for this pilot study. The stones were made of BegoStone Plus (BEGO USA, Lincoln, RI) in a 15:5 powder to water ratio by weight 9 and formed into 2 cm spherical rubber molds. The kidney model simulated PCNL through an upper pole access with fluid irrigation and drainage. We performed PCNL with a 24F rigid nephroscope (Karl Storz, Tuttlingen, Germany) through the 30F working sheath. In all trials, stone fragmentation was performed with the CyberWand™ dual ultrasonic lithotripter (Olympus, Center Valley, PA). In the trials with the PercSac, a three-pronged rigid grasper was used to facilitate stone capture into the pouch. Lithotripsy commenced once the bag was cinched, and the trial was complete when the contents of the bag were sufficiently fragmented to allow removal of the bag through the sheath. In the trials without the PercSac, lithotripsy was performed upon entry into the renal pelvis, and any remaining fragments not aspirated were removed with the rigid grasping forceps. Endoscopic and direct inspections of the hollow portions of the kidney model were performed after stone fragmentation and residual fragment retrieval were complete. If no fragments were present, the kidney was deemed stone free. The primary end points were time to stone fragmentation (time of ultrasonic lithotripsy), time to stone clearance (from insertion of the nephroscope into the kidney to final removal of the nephroscope from the kidney, including time for ultrasonic lithotripsy and time for grasping residual fragments), assessment of stone-free status, and need for flexible nephroscopy to achieve or assure a stone-free state. Median times for stone fragmentation and stone clearance were compared with and without the PercSac using Student's t-test. All statistical analyses were performed with SPSS® version 19 (IBM Corp., Armonk, NY).
Results
All stones were 2 cm in diameter and the mean stone weight for both groups was nearly identical at 4.76 g (PercSac SD = 0.12, no PercSac SD = 0.16). The median time for stone fragmentation with the CyberWand was significantly shorter in the PercSac group compared with the control group (217 seconds [IQR = 169–255] vs 340 seconds [IQR = 310–356], p = 0.028). Likewise, the total time from insertion of the nephroscope into the kidney model to completion of stone clearance from the kidney was significantly shorter for the PercSac group (293 seconds [IQR = 244–347]) compared to the control group (376 seconds [IQR = 375–480]) (p = 0.047). All five trials without the PercSac had small residual fragments remaining after lithotripsy was performed and, thus, required flexible nephroscopy with basket stone extraction to achieve a stone-free state. Only one trial with the PercSac device had residual dust remaining in the kidney model after lithotripsy and it was too small to retrieve with a basket. None of the trials with the PercSac required flexible nephroscopy for stone clearance. The PercSac device remained intact for all trials, including the one with dust remaining in the kidney, therefore this dust was thought to have escaped through the cinched end of the device and was too small to capture. Neither stone fragments nor the ultrasonic lithotripter have violated the integrity of the polyethylene material or Nitinol wire that comprises the PercSac. There were no failed attempts at PercSac deployment, stone capture within the device, or cinching of the device. There were no device related complications to the kidney model or other equipment during trials with the PercSac.
Discussion
The measure of success of a surgical stone procedure is the ability to render a kidney free of stones. While complete stone clearance is the ultimate goal it can be difficult, time consuming, and costly to attain. The assumption that patients undergoing SWL who were left with asymptomatic uninfected stones ≤5 mm experienced few clinical consequences led to the term CIRF. 5 However, several investigators have followed the natural history of patients with CIRF after PCNL and found that a significant number of patients experienced a negative clinical outcome as a result of the residual stones, and consequently, the use of this term has been discouraged.
Altunrende and colleagues studied the natural history of residual fragments after 430 PCNL procedures in which 22% of patients had residual fragments ≤4 mm 3 months after surgery based on kidney, ureter, and bladder radiograph. Those with residual fragments underwent immediate CT to determine the stone size and location of the fragments and then annually or when symptoms occurred. Among the 38 patients with residual fragments who had at least 24 months of follow-up, 26.3% of these patients experienced symptoms such as renal colic pain or hematuria. They identified struvite stone composition as a risk factor for residual stone growth during this time. 6
Raman and colleagues also examined the natural history of small residual fragments after PCNL and performed multivariate analysis to determine predictors of a future stone-related event, defined as growth of a residual fragment or need for emergency medical care, hospitalization, or intervention for residual fragments. Among 527 patients who underwent PCNL and had at least 6 months of radiographic follow-up, 42 patients (8%) were left with residual fragments and did not undergo second look flexible nephroscopy for stone removal. The residual stone fragments were ≤2 mm in 60% of patients and ≤5 mm in 79% of patients. At a follow-up of 41 months, 18 patients (43%) experienced a stone-related event such as emergency room visit or hospitalization and 11 of 18 or 61% required secondary surgical intervention. Independent predictors of a stone-related event included stones located in the renal pelvis or ureter (HR: 4.4, 95% CI: 1.0–13.5, p = 0.01) and stones larger than 2 mm (HR: 3.9, 95% CI: 1.3–11.5, p = 0.01). 7 This group compared the cost incurred with observation of residual fragments vs the cost of planned second look nephroscopy and found a cost advantage to second look nephroscopy over observation when the residual stone was greater than 4 mm. 10 These studies highlight the consequences of leaving behind even small residual fragments after PCNL.
Achieving a stone-free state during conventional PCNL can be challenging, often requiring a flexible nephroscope and sometimes a flexible ureteroscope, as well as disposable equipment such as Nitinol baskets, graspers, and laser fibers. These maneuvers are associated with increased direct and indirect costs from equipment processing fees, disposable inventory costs, and the cost of operating room and anesthesia time. Beyond the financial cost, there is additional risk to the patient from prolonged operative time and additional maneuvers within the kidney and/or ureter. In addition, once stone fragments are generated with lithotripsy in the collecting system, stone-free status cannot be ensured without a CT postoperatively. If residual fragments remain then the patient will typically undergo a planned second stage procedure at an additional cost to the patient and healthcare system with potentially reduced reimbursement to the surgeon for a procedure within the global period of PCNL.
Because of the morbidity and cost associated with residual fragments after PCNL, we developed a novel device that we termed the PercSac to capture and contain a stone during ultrasonic lithotripsy to decrease the likelihood of fragment migration and ultimately residual stone fragments. We first reported on the performance and utility of this device in an in vitro cystolithopaxy model in which we showed that the PercSac improved stone fragmentation rate and efficacy compared to conventional cystolithopaxy without the device. 8 While the benefits of stone containment during lithotripsy are readily apparent for the treatment of bladder stones, the containment of a stone during lithotripsy in the kidney could prove to be even more valuable as generated small fragments are at risk for migration into difficult to access calices and/or the ureter. The results of our present study demonstrate that the PercSac device can be deployed and utilized in the confines of a human kidney upper tract collecting system model. Moreover, in our in vitro PCNL model, treatment of 2 cm renal pelvis stones entrapped within the PercSac device compared to conventional PCNL technique was associated with greater speed of stone fragmentation and greater efficacy by obviating the need for flexible nephroscopy to achieve a stone-free state in any trials. These results provide support for continued investigation of the PercSac as a tool to increase the efficiency and efficacy of PCNL for individual kidney stones as much as 2.5 cm in diameter.
Several other devices have been developed to decrease the migration of stones and reduce the chance for residual fragments during ureteroscopy and/or PCNL, including the Stone Cone™ (Boston Scientific, Natick, MA), 11 Accordion™ (PercSys, Palo Alto, CA), 12 and BackStop™ Gel (Boston Scientific). While all of these devices were met with limited success for this indication, they also differ from the PercSac in that they are primarily aimed at preventing migration of fragments down the ureter, but not throughout the collecting system. Therefore, they cannot offer the same assurance of a stone-free state as the PercSac.
We feel that while the PercSac has demonstrated its effectiveness in an in vitro PCNL model, our study has several important limitations. First, the device is more efficacious when the entire stone can be entrapped within the pouch, and therefore, it is ideally suited for the treatment of individual unbranched kidney and bladder stones measuring no more than 2.5 cm in largest diameter, which is the ideal size accommodated by the PercSac. Use of the device for larger stones would require fragmentation into ∼2 cm pieces, which could then be individually entrapped and fragmented in the PercSac. However, any fragmentation outside the bag would reduce the chance of leaving behind no residual fragments. Second, in our model the interpolar and lower pole calices were solid. The 2 cm stones were too large to migrate from the renal pelvis into calices so this likely had little effect on the ability to trap a stone in the PercSac. In addition, it could favor the trials without the PercSac by reducing the available space into which residual fragments could migrate. Finally, the rigid nature of our kidney model does not mimic the consistency of a human kidney. While a softer model would better assess if the PercSac is atraumatic to a human collecting system, the polyethylene, Nitinol, and rubber tip that comprise the PercSac are the materials in most disposable devices safely used during PCNL. Furthermore, a softer model may lend an advantage to the PercSac not seen with our rigid model by allowing for collecting system dilation with irrigation, and subsequently, more room to deploy the PercSac. We plan future testing of the device in a softer in vitro kidney model, as well as in in vivo bladder and kidney models with use of other lithotripsy devices.
Conclusion
A novel polyethylene stone entrapment sack (PercSac) is an effective and efficacious adjunct to conventional PCNL for the treatment of 2 cm renal pelvis stones in a kidney model. The benefits of this device are likely to be even more pronounced during clinical PCNL where stone fragments can migrate into more complex and difficult to access calices and/or the ureter.
Footnotes
Acknowledgments
These data were presented at the following conferences: The Engineering and Urology Society Meeting at the American Urological Association Annual Meeting, 2015 and The World Congress of Endourology Annual Meeting, 2015.
Author Disclosure Statement
Dr. Jodi Antonelli is on the scientific advisory board for Boston Scientific. No completing financial interests exist for the remaining authors.