
Abstract
Introduction:
The traditional procedure for the management of bilateral ureteral stones is staged ureteroscopic lithotripsy (URS). However, in recent years particularly, some urologists advocate same-session bilateral URS on the ground of success rates and minimal morbidity. This systematic review is to evaluate the efficacy and safety of same-session bilateral ureteroscopy for the treatment of ureteral calculi.
Materials and Methods:
We conducted a bibliographic search using MEDLINE (1980 to August 2015) and EMBASE (1980 to August 2015). Review articles and abstract data were excluded and only studies in English reporting on outcomes of bilateral URS were included in this meta-analysis. Two reviewers independently assessed the quality of each included studies and extracted data. STATA 12.0 was used for meta-analysis.
Results:
In 11 studies, 431 patients were reportedly treated with bilateral URS. Most of the stone sizes were not larger than 20 mm. The mean stone-free rate is 96% for the distal ureter, 85% for the middle ureter, and 72% for the proximal ureter. The mean operative time ranged from 45 to 100 minutes with an average hospital stay from 2 to 4 days. The overall complications rates were 17%, with the incidence of postoperative fever 4%, postoperative pain 20%, and gross hematuria 4%. Other complications, including urosepsis, urinary tract infection, small mucosal laceration, stone migration, and ureteral perforation, accounted for 6% of overall complications.
Conclusions:
This meta-analysis found that bilateral same-session ureteroscopy could achieve a high overall stone-free rate. There might be a relatively higher complication incidence, but most of the complications are minor. For selected cases, bilateral URS could be safe and effective.
Introduction
O
The 2007 EUA/AUA Guidelines for the Management of Ureteral Calculi indicate that URS can be used simultaneously to treat bilateral ureteral stones in selected cases. 7 Several studies on bilateral URS suggested that it is safe and effective. 3,4,8,9 However, the reported results differed among those studies. In addition, those results might potentially be biased and imprecise, as most studies are case series, and only involved a relatively small number of patients. The same-session bilateral ureteroscopy for treatment of ureteral calculi still requires evaluation. To understand and interpret the available evidence, we conducted a systematic review to evaluate the efficacy and safety of same-session bilateral ureteroscopy for the treatment of ureteral calculi.
Materials and Methods
Literature search and inclusion criteria
We conducted this meta-analysis in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis Statement. 10 PubMed and EMBASE were searched by two authors independently (H.G., X.Z.) to identify the relevant studies (from 1980 to August 2015). The search strategy was combining the subject term and free term with the following key words: (((“Ureteral Calculi”[Mesh] OR “Kidney Calculi”[Mesh])) AND ((((((((Bilateral synchronous ureteroscopy) OR Bilateral single-stage ureteroscopy) OR Bilateral same-session ureteroscopy) OR Bilateral one-session ureteroscopy) OR Bilateral single-session ureteroscopy) OR Bilateral simultaneous ureteroscopy)))).
We considered a broad range of study designs, including randomized control trials (RCTs), observational studies, and noncomparative case series. Review articles, nonpeer-reviewed local/government reports, conference abstracts, and presentation were excluded in this study. In addition, the reference lists of retrieved studies were also rechecked manually to identify whether these listed trials are eligible. This process was repeated until no further relevant studies were detected. Studies included met the following criteria: (1) patients—people with bilateral ureteral stone; (2) intervention—bilateral same-session URS; and (3) outcomes—stone-free rate, operation duration, complications, and hospital stay.
Data extraction and outcome measures
Two reviewers (H.G., X.Z.) independently extracted the following information from the included studies: first author, date of publication, number of patients, patient characteristics, stone location, stone burden, intervention of bilateral same-session URS, stone-free rate (or data to calculate the rate), serum creatinine, complications, operation duration, and hospital stay. The extracted data were inputted into an Excel file and checked by the third author (C.Y.). Disagreements were solved by discussion.
Quality assessment
Critical appraisal of the studies was considered by study type and data collected. Case series, which comprised most of the studies, were assessed by the National Institute for Health and Care Excellence (NICE) Quality Assessment for Case Series system (Table 1). 11 It assesses characteristics of methodology, outcomes, and interpretation from a possible score of 8. We consider studies with a total score ≥4 to be “higher quality” and scores <4 to be “lower quality.”
NICE = National Institute for Health and Care Excellence.
Methodologic index for nonrandomized studies (MINORS) was used to evaluate the quality of non-RCTs included in this meta-analysis (Table 2). 12 This scale consists of 12 evaluation items, and each item scores 0 to 2. One point would be allocated to each item if it has been mentioned in the article, and an additional point would be given if the item has been detailed and appropriately described. If the item had not been recorded, then one point was deducted. A MINORS score ≤12 is considered to be of low quality, whereas a study with a MINORS score >12 is thought to be of high quality.
0 = Not reported; 1 = unclearly stated; 3 = clearly stated; NRCT = Non-randomized controlled trial.
Statistical synthesis
We carried out the meta-analysis using STATA 12.0 (2012; STATA Corporation, College Station, TX). Heterogeneity of included studies was checked using the χ2-test, which was a qualitative analysis to judge statistical heterogeneity, and the I 2-test, which was a quantitative analysis of measuring the percentage of inconsistency. If a P-value for heterogeneity was >0.1 in aχ2-test, indicating no heterogeneity among studies, fixed-effects models were applied. Otherwise, the random-effects models were used. The I 2-value in I 2-test delineated the proportion of total variation due to heterogeneity instead of errors of sampling, and I 2-value >50% presents faithful heterogeneity. For all studies analyzed, a P-value of <0.05 was considered statistically significant.
Results
Study selection
One hundred and seven citations were identified from the literature search, and 11 studies (431 patients) were included in this systematic review. Figure 1 shows the literature selection process.

The flow diagram of literature selection process in this study.
Study characteristics and quality assessment
The baseline characteristics of the 11 studies in this meta-analysis are shown in Table 3. These studies were published between 1994 and 2012. The sample size ranged from 7 to 89 patients. Studies included were scored from 6 to 8 out of a full NICE credit of 10, and all these studies were considered to be of high quality. One noncomparative study was scored 22 points according to MINORS scale and was considered of high quality.
MINORS = methodologic index for nonrandomized studies.
Stone burden
Six studies 3,4,13 –16 reported stone burden, and they calculated the stone size by measuring the length of the maximum stone diameter. In patients with multiple stones, the length of the maximum diameter of each stone was added up to calculate the size. Most of the stone sizes were not larger than 20 mm.
Operative time
Out of the 11 trials, 7 studies 3,4,13 –17 considered the operation duration and the majority of the operation duration was 50 to 100 minutes.
Serum creatinine
Four studies 4,15,18,19 described serum creatinine change in their reports. Watson and colleagues 4 described in their study that among 47 patients (49%), the mean change of serum creatinine level postoperatively was 0.02 mg/dL (ranging −0.9 to 1.3), including −0.01 mg/dL (ranging −0.9 to 0.3) in 18 with no stent postoperatively, 0.18 mg/dL (ranging −0.1 to 0.8) in 6 with a unilateral stent, and 0.07 mg/dL (ranging −0.7 to 1.3) in 23 patients with bilateral stents. And most of the studies reported that serum creatinine level returned back to nearly normal level within 4 to 12 days.
Length of hospital stay
Out of the 11 trials, 6 studies 13 –18 considered the length of hospital stay and the majority of the participants were discharged 2 to 4 days after surgery. These six studies were published ranging from 1996 to 2012, and that hospital stay is a bit too long in today's opinion. As the surgical skills improved and instruments advanced, ureteroscopy has been performed as daycare procedures in some big centers now.
The overall stone-free rate
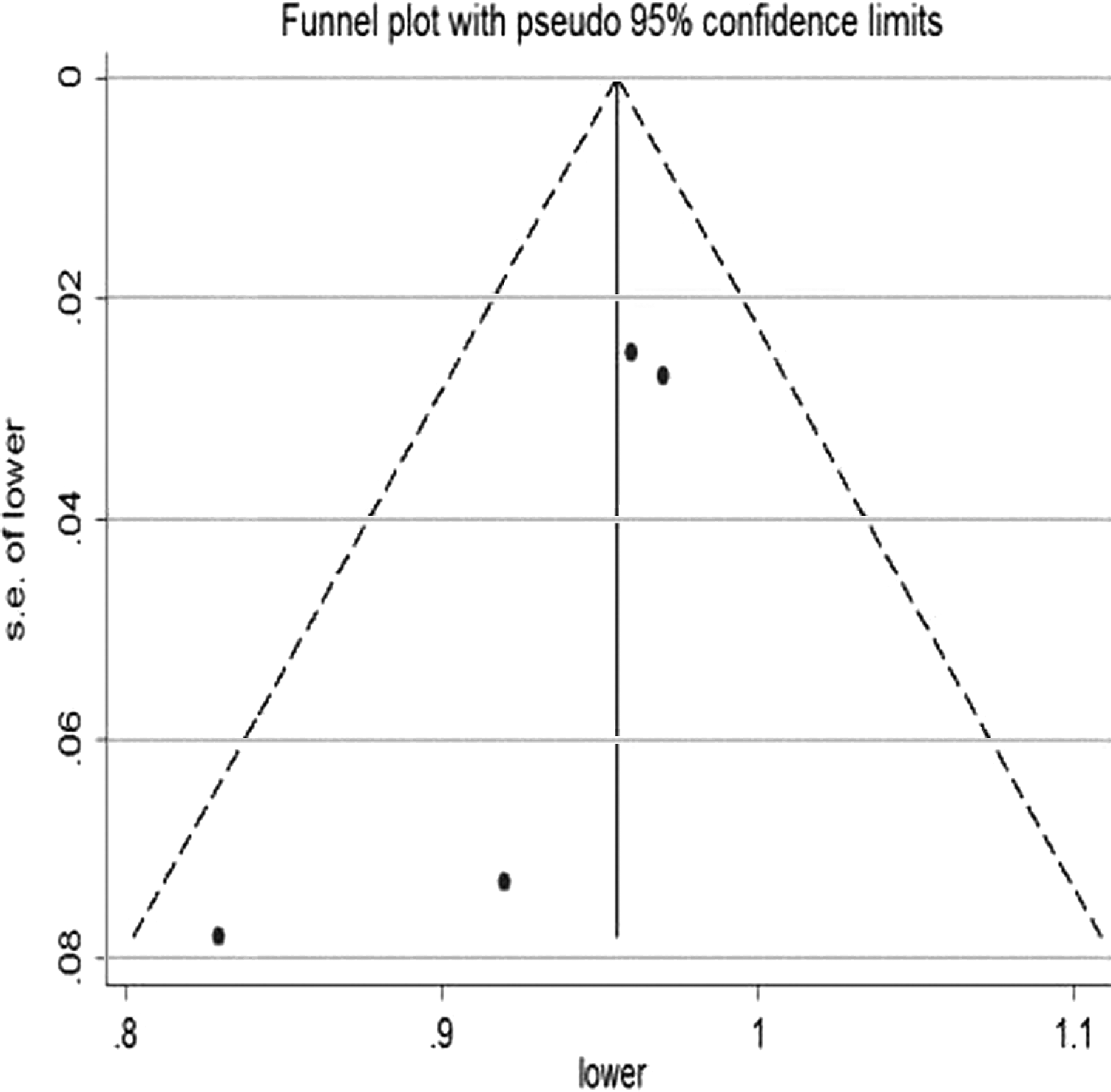
All the 11 studies 3,4,8,13 –20 described overall stone-free rate after surgery. Six studies 3,4,8,13,16,18 mentioned the standard and detection methods of stone-free rate, including postoperative Plain Film of Kidney-Ureter-Bladder, Ultrasound, or CT scan. A result without any residual fragments or only with residual fragments <2 mm, but no clinical symptoms, was considered to be effective. The other five studies did not specifically mention the stone clearance rate standard and detection method. There was evidence for heterogeneity between the studies (P = 0.027, I 2 = 50.6%). The funnel plot showed a fairly symmetrical distribution of the stone-free rate. One study lies outside of the confidence intervals (CIs). The random effect model of meta-analysis showed that the overall stone-free rate was 82% (95% CI: 52%, 90%; Figs. 2 and 3).
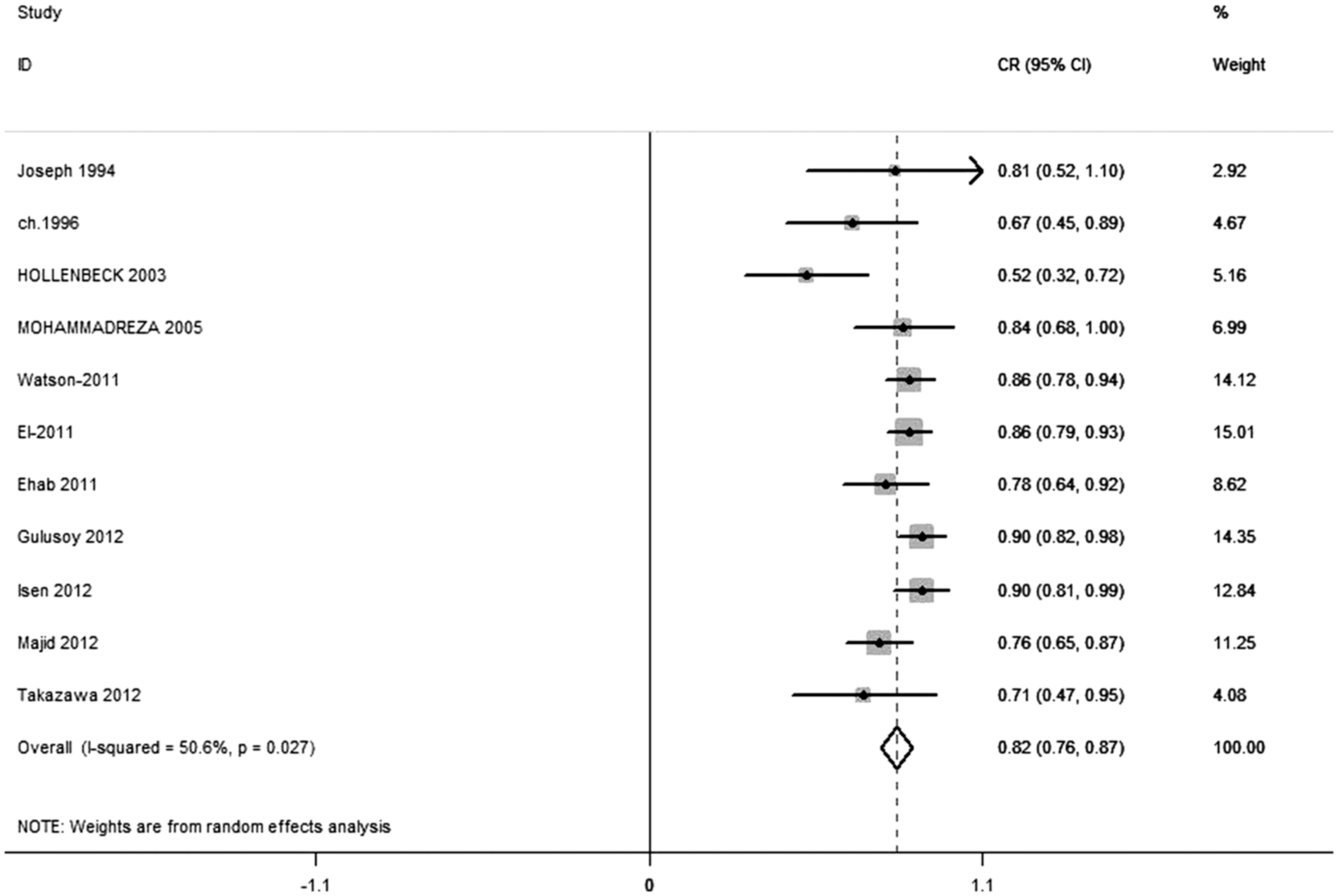
The random effect model showing overall stone-free rate. CR = clearance rate, CI = confidence interval.

The funnel plot for total stone clearance rate. s.e. = stand error.
Seven studies 3,4,15 –19 reported the overall stone-free rate after follow-up, and most of the follow-up time were 1 to 3 months. There was evidence for heterogeneity between the studies (P = 0.049, I 2 = 52.6%). The funnel plot showed a fairly symmetrical distribution of the stone-free rates; one study lies outside the CIs. The random effect model of meta-analysis shows that the overall stone-free rates were 91% (95% CI: 87%, 95%; Figs. 4 and 5).

The random effect model showing overall stone-free rate after follow-up.

The funnel plot for stone clearance rate after follow-up.
Stone free-rate for the distal ureter
Four studies 3,8,13,14 described stone-free rate for the distal ureter after surgery. There was no evidence for heterogeneity between the studies (P = 0.37, I 2 = 4.3%). The fixed effect model of meta-analysis shows that the stone-free rates for the distal ureter were 96% (95% CI: 92%, 99%; Figs. 6 and 7).
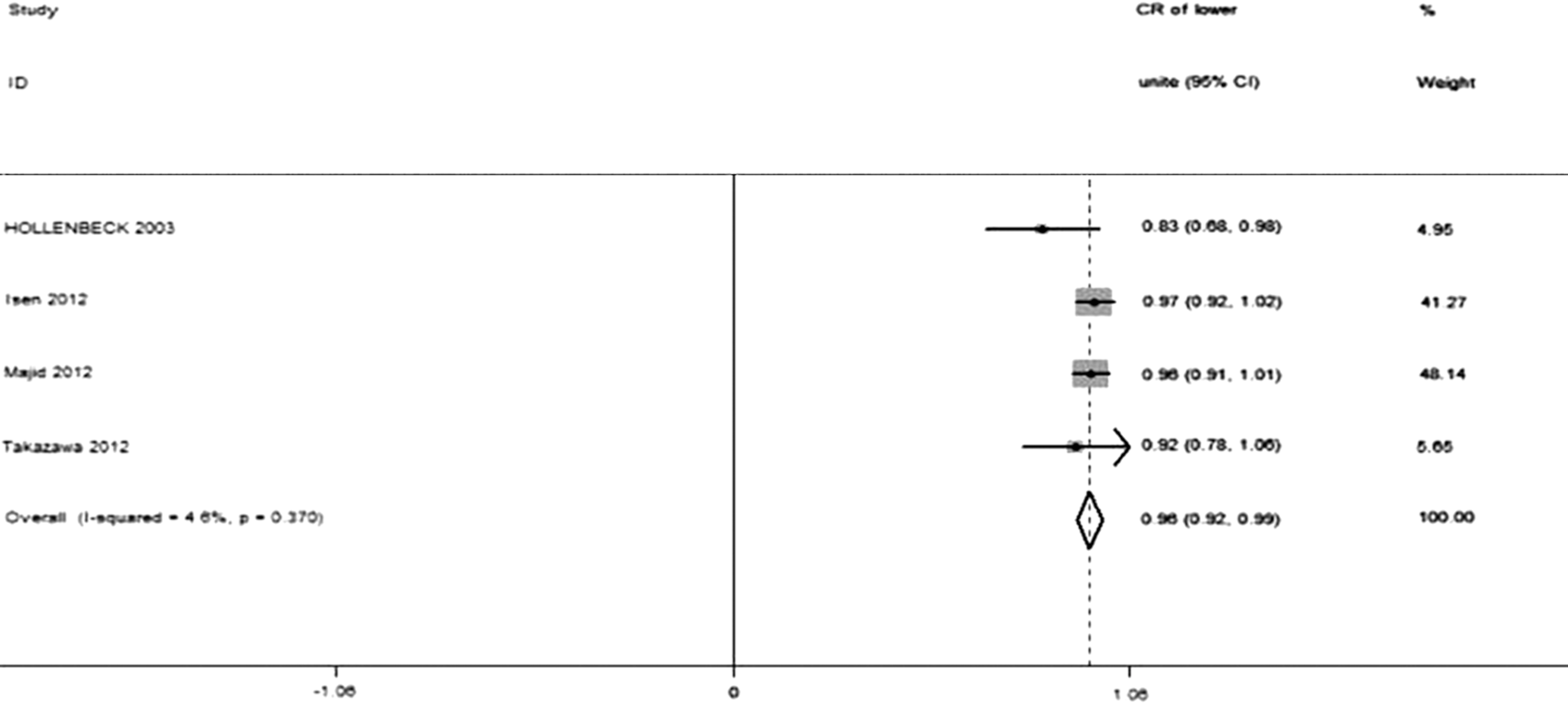
The fixed effect model showing the stone-free rate for distal ureter.
The funnel plot for the stone-free rate of distal ureter.
Stone-free rate for the mid ureter
Three studies 8,13,14 described stone-free rate for the middle ureter after surgery. There was no evidence for heterogeneity between the studies (P = 0.589, I 2 = 0). The fixed model of meta-analysis show that the stone-free rates for the mid ureter were 85% (95% CI: 79%, 92%; Figs. 8 and 9).
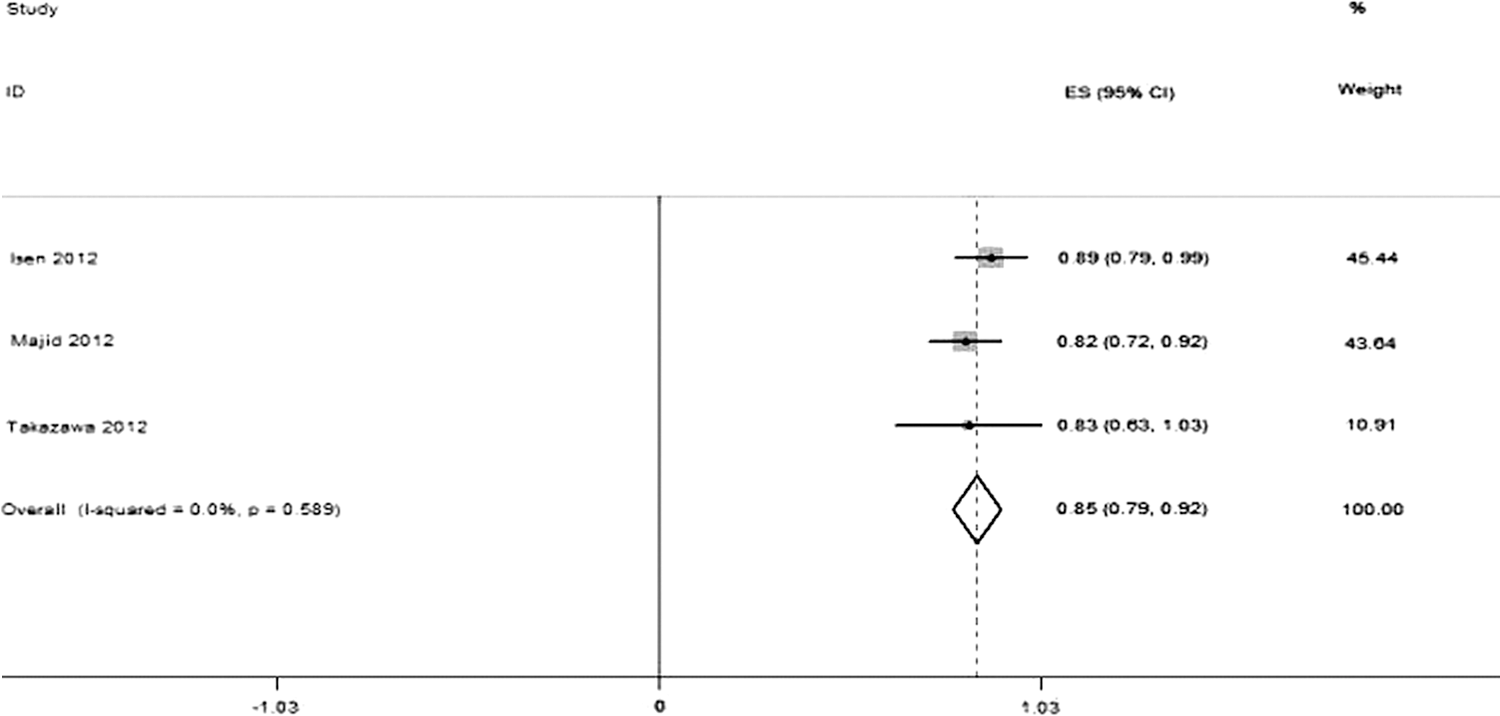
The fixed effect model showing the stone-free rate for the mid-ureter.

The funnel plot for the stone-free rate for the mid-ureter.
Stone-free rate for the proximal ureter
Four studies 8,13,14,17 described stone-free rate for the proximal ureter after surgery. There was no evidence for heterogeneity between the studies (P = 0.784, I 2 = 0). The fixed effect model of meta-analysis shows that the stone-free rates for the proximal ureter were 72% (95% CI: 64%, 79%; Figs. 10 and 11).
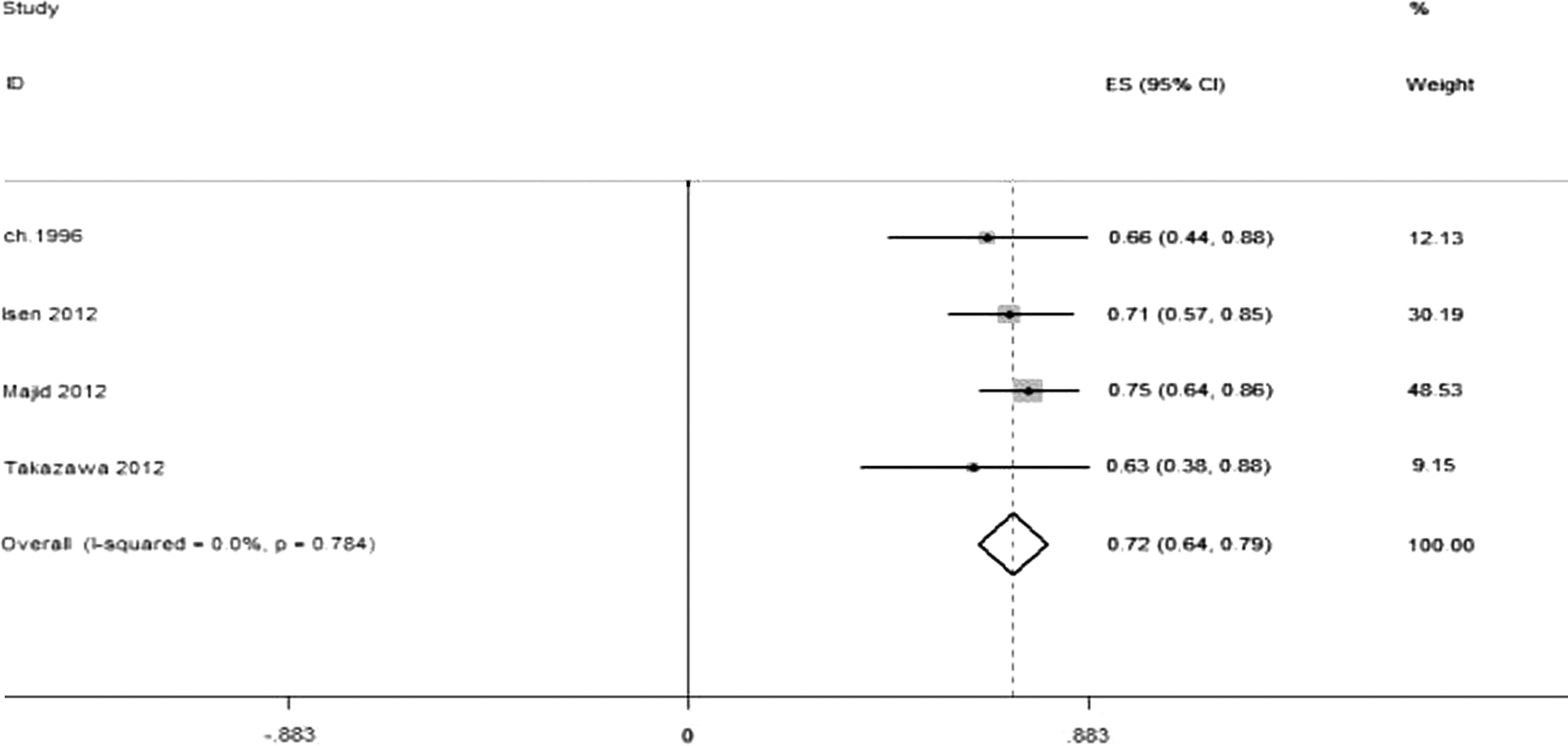
The fixed effect model showing the stone-free rate for the proximal ureter.

The funnel plot for the stone-free rate for the proximal ureter.
Complications
Postoperative fever
Six studies 13 –16,18,20 described incidence of postoperative fever. There was no evidence for heterogeneity between the studies (P = 0.1, I 2 = 45.9%). The fixed effect model of meta-analysis shows that the incidence of postoperative fever was 4% (95% CI: 2%, 7%; Figs. 12 and 13).
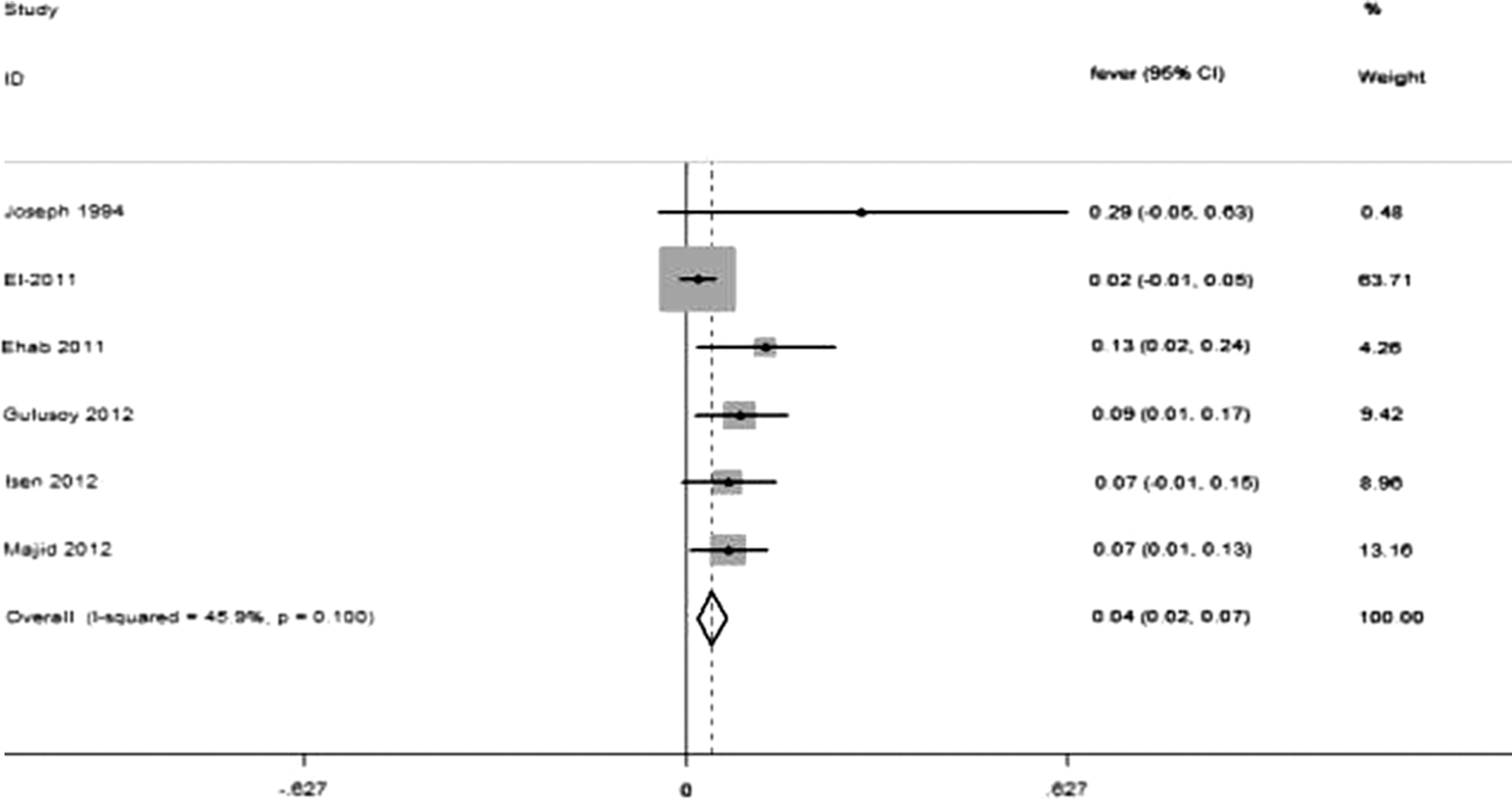
The fixed effect model showing the incidence of postoperative fever.
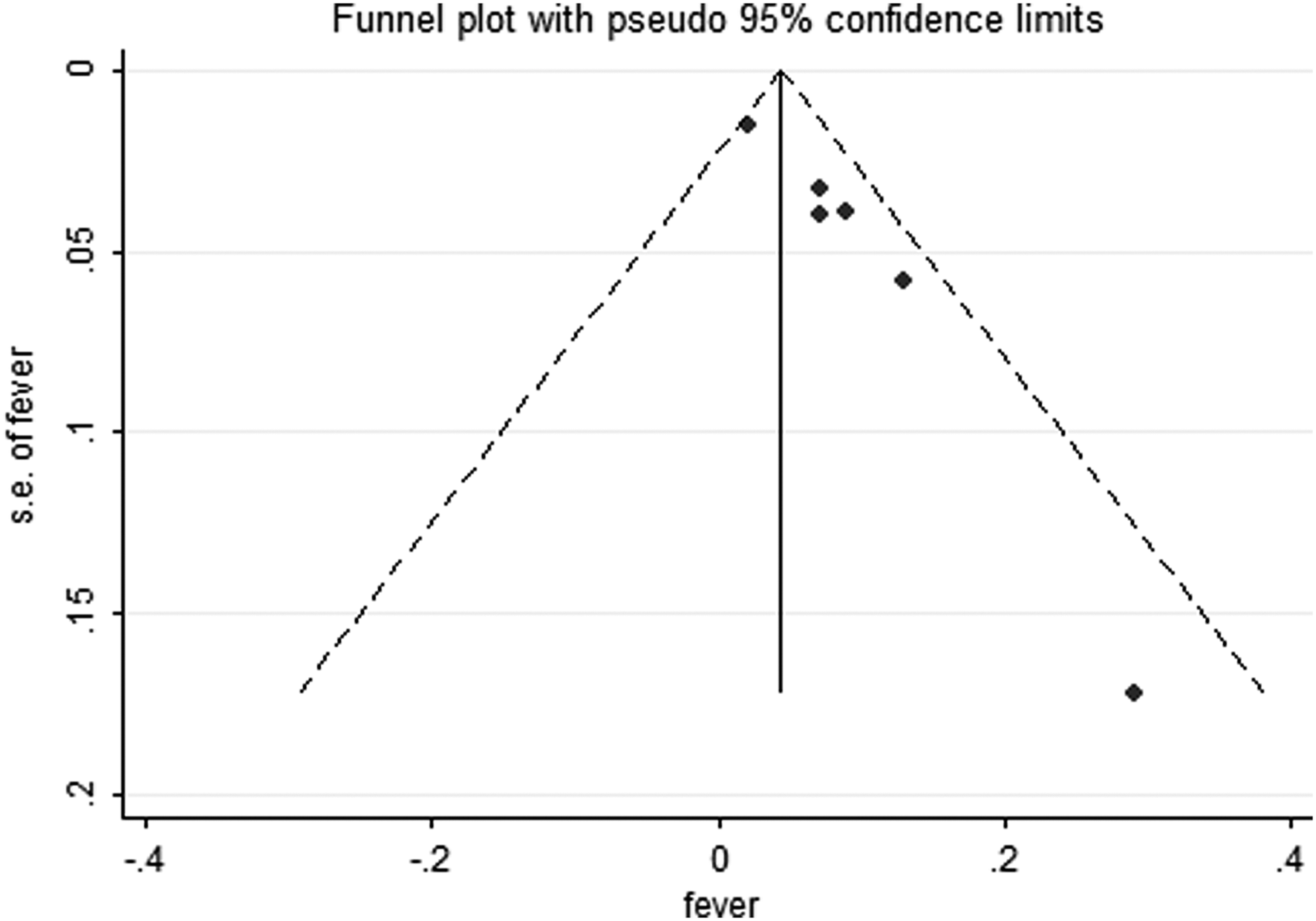
The funnel plot for the incidence of postoperative fever.
Postoperative pain
Four studies 3,13,14,20 described incidence of postoperative pain; there was no evidence for heterogeneity between the studies (P = 0.492, I 2 = 0). The fixed effect model of meta-analysis shows that the incidence of postoperative pain was 20% (95% CI: 14%, 27%; Figs. 14 and 15).
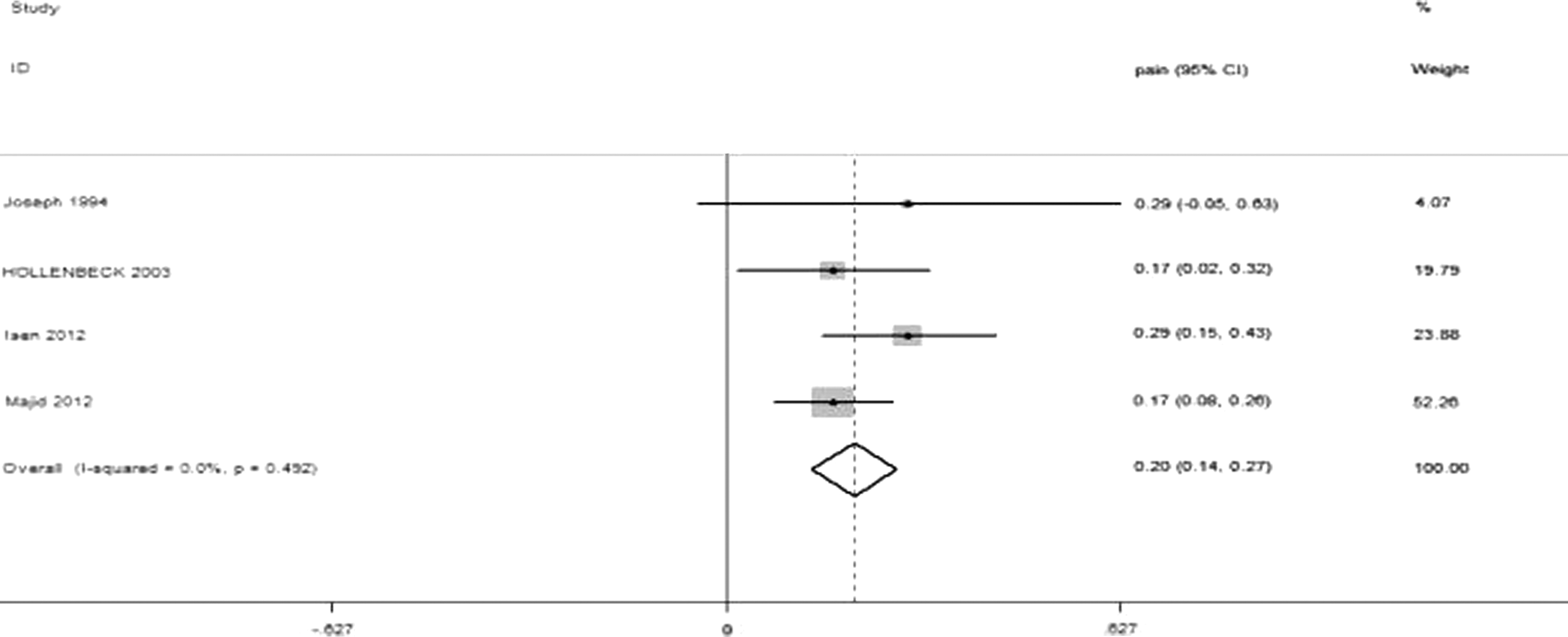
The fixed effect model showing the incidence of postoperative pain.

The funnel plot for the incidence of postoperative pain.
Gross hematuria
Five studies 13 –15,18,20 reported incidence of gross hematuria after surgery. There was evidence for heterogeneity between the studies (P = 0.019, I 2 = 62.9%). The random effect model of meta-analysis shows that the overall incidence of gross hematuria was 4% (95% CI: 1%, 7%; Figs. 16 and 17).
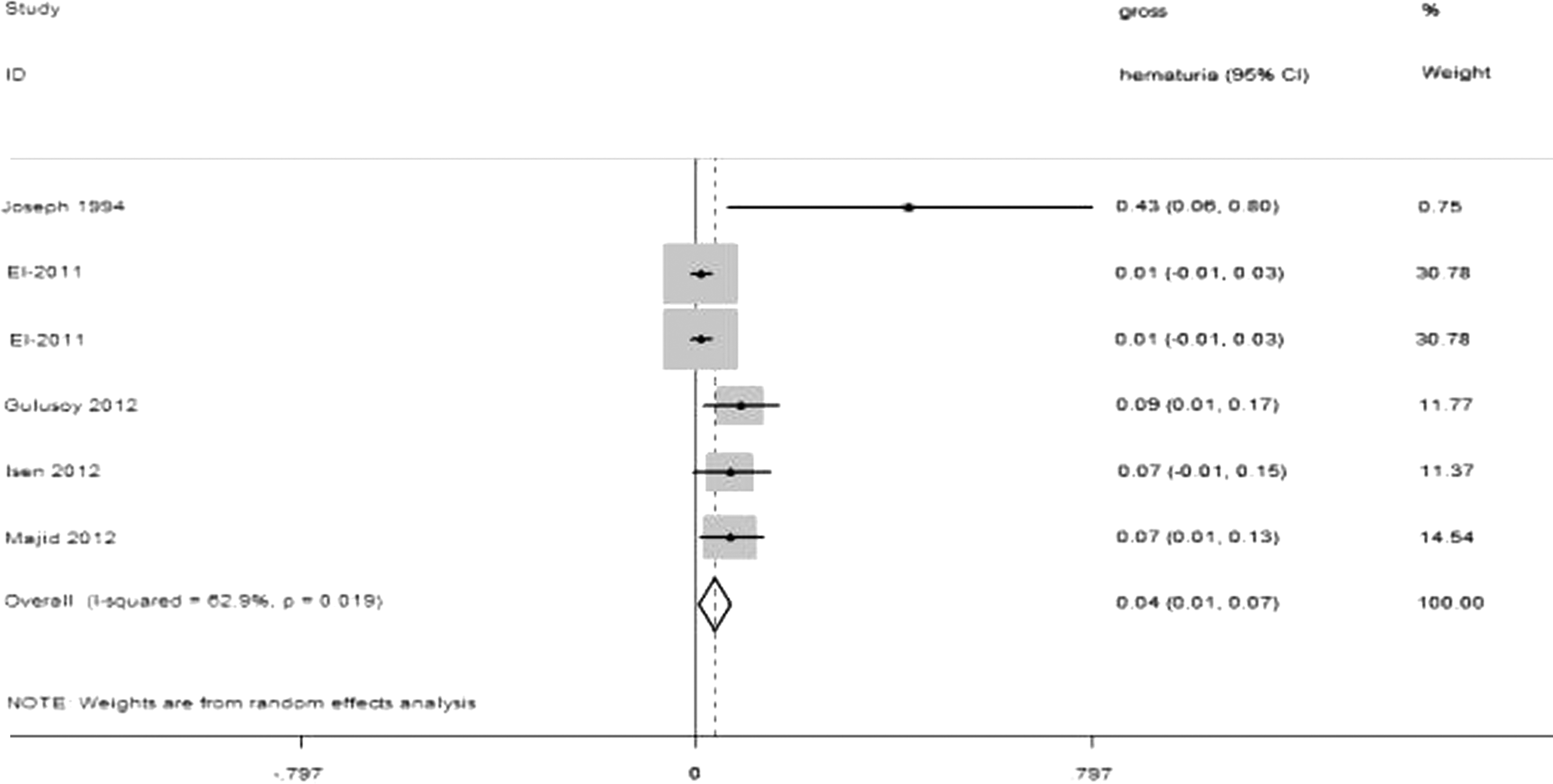
The random effect model showing the overall incidence of gross hematuria.

The funnel plot for the incidence of gross hematuria.
Other complications
Other complications included urosepsis, urinary tract infection, small mucosal laceration, stone migration, and ureteral perforation, and each complication has been reported in 1, 3, 6, 5, and 11 patients, respectively. A total of 26 other complications occurred in 431 patients, accounting for a ratio of 6% (Table 4).
UTI = urinary tract infection.
Overall postoperative complication rate
Four studies 3,14,16,18 described incidence of overall postoperative complication rate. There was evidence for heterogeneity among the studies (P = 0, I2 = 87.3%). The random effect model of meta-analysis shows that the overall incidence of gross hematuria was 17% (95% CI: 3%, 31%; Figs. 18 and 19).
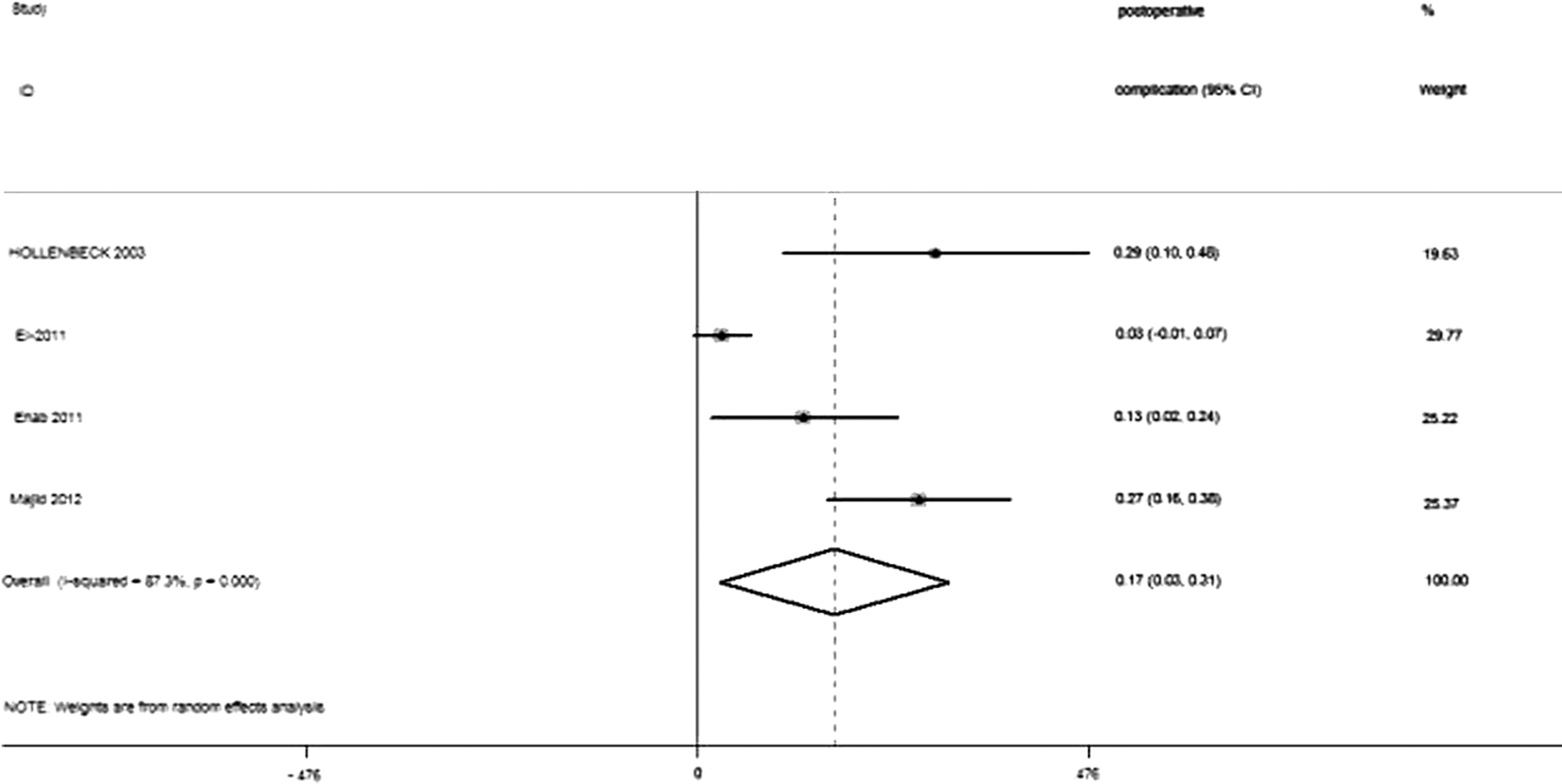
The random effect model showing the incidence of postoperative complications.

The funnel plot for the incidence of postoperative complication.
Discussion
This meta-analysis summarizes the efficacy and safety of same-session bilateral ureteroscopy for treatment of ureteral calculi, and this review is important at this time as same-session bilateral ureteroscopy has been used by a growing number of urology centers. Eleven studies involving 431 patients were included in this study. Most of the stone sizes were no larger than 20 mm. According to studies that reported individual data, the overall stone-free rate ranged from 52% to 90% with mean operative time ranging from 45 to 100 minutes and hospital stay from 2 to 4 days.
In our systematic review, bilateral same-session ureteroscopy had an average stone-free rate of around 96% for the distal ureter, 85% for the middle ureter, and 72% for the proximal ureter. It was similar to the results in a previous Clinical Multicenter Study, which reported that the stone-free rate of single stone was 94.2% for the distal ureter locations, 89.4% for the mid-ureter locations, and 84.5% for the proximal ureter locations. Although the criteria defined differ in these two studies, results suggested that bilateral same-session ureteroscopy has a similar stone-free rate with ureteroscopic stone treatment of single stone.
In this systematic review, the overall complication rate was 17%, with the incidence of postoperative fever 4%, postoperative pain 20%, and gross hematuria 4%. A potential drawback of simultaneous bilateral manipulation is the increased complication rates, and concerns about it may dissuade urologists from same-session ureteroscopy for bilateral stones. At first glance, the risk of developing complications appears to be twice that of staged procedures. However, this implies that the overall risk of treating a patient with bilateral stones is determined by the number of renal units addressed instead of whether patients are treated simultaneously or in separate procedures and it also implies that by staging the treatment, the risk of developing a complication is only diffused over time rather than being faced entirely at the time of same-session bilateral procedure. 14 In addition, with appropriate patient selection (stone size no larger than 20 mm), enough experience, and proper facilities, complications can be minimized and patients can be effectively treated. Patients with bilateral lower ureteral stones are the best candidates for same-session ureteroscopy because it has high stone-free rates for such patients.
Initial opposition to the same-session bilateral ureteroscopy arose from concerns that renal units from both sides could be compromised simultaneously. In fact, acute renal failure was reported in one patient after same-session bilateral ureteroscopy. 21 That patient is a 53-year-old female. She was found to have a 5 mm lower pole and an 8 mm interpolar bilateral calculi, and no ureteral stent was placed after the procedure. Anuric renal failure (elevation of serum creatinine from 0.9 to 3.5 mg/dL) was developed in 24 hours. After emergent bilateral ureteral stent placement, her creatinine returned to normal in 24 hours and she was eventually discharged home 6 days after surgery. Although there is no consensus about stenting patients who underwent same-session bilateral ureteroscopy, in consideration of renal failure in rare cases, ureteral stent should be given at least one side to avoid severe complications.
Other complications like urosepsis, small mucosal laceration, and ureteral perforation also occurred. However, serious intraoperative complications have greatly decreased over the years as a result of careful instrument selection and improvement of surgical techniques.
Bilateral same-session URS may be a cost-effective treatment option for patients with bilateral urinary tract stones. Cone and associates 22 have reported the cost-effectiveness of URS for patients with renal stones in the United States. The average costs per URS procedure were $4470, including $456 for surgeon's fee charge, $2475 for anesthesia fee charge, $1375 for facility cost, and $164 for stent placement cost. Apparently, bilateral URS can at least save patients the charge of surgeon's fee, anesthesia fee, and facility cost by once, not to mention the cost of radiologic, preoperative, and postoperative laboratory analysis, drug administration, and cumulative hospital stay.
Moreover, in consideration of social cost, it is rather intuitive that bilateral procedure takes the patients much shorter time to return to normal activities. And it should also be stressed that there is an increasing awareness of reducing healthcare costs under the current medical and political climate. Therefore, if clinical safety and outcomes are guaranteed, social cost containment is something that a doctor should always be aware of.
Another advantage of bilateral URS is single anesthesia. It is well known that the duration of surgery and anesthesia is probably one of the strongest predictors of postoperative pulmonary complications; bilateral URS can avoid second anesthesia and may reduce the risk of postoperative pulmonary complications.
Our meta-analysis has some limitations. First, the number of included studies is relatively small, and no RCTs were included. The small number of participants and included studies, as well as the moderate or low quality of most studies in this analysis, might not lead to a reliable conclusion.
Second, we only included the data of published studies, while unpublished reports may show less positive results. So the exclusion of these abstracts might have introduced bias in favor of the intervention due to small sample and limited methodologic quality of the included studies.
And hence a larger sample of higher quality, long-term randomized controlled trials with more vigorous and more efficient performance, and more detailed outcomes are needed to confirm the above results.
Conclusion
Overall, bilateral same-session ureteroscopy holds considerable promise as a therapy for the treatment of bilateral ureteral stones. However, despite being reported almost for 20 years, many serious questions still remain to be answered before this method can be widely advocated. More quality research is still needed because this treatment lacks clear criteria to screen target patients for this treatment. In addition, details related to the surgery require further evaluation to guarantee the most safe and effective practice. Well-designed RCTs and long-term follow-up registries are needed to capture the efficacy and safety profile of this method.
To summarize, based on our meta-analysis, bilateral same-session ureteroscopy could achieve a high overall stone-free rate; the complication rate seemed to be high, but most complications are minor. For selected cases, bilateral URS is safe and effective.
Footnotes
Author Disclosure Statement
No competing financial interests exist.