
Abstract
Purpose:
The selective α-adrenoceptor blocker is widely used as a cost-effective treatment option for medical expulsive therapy (MET) of ureteral stones. In this review, we aimed to assess the efficacy and safety of naftopidil for MET compared with control or tamsulosin.
Methods:
A systematic literature search was performed in PubMed, Cochrane Library, Embase, and Google Scholar to identify randomized controlled trials that compared naftopidil with either control or tamsulosin for the management of distal ureteral stones.
Results:
We included 7 publications with 553 patients. Naftopidil was not only effective for distal ureteral calculi but also was comparable to tamsulosin in efficacy. The expulsion rate (risk ratio [RR] 2.00, 95% confidence interval [CI] 1.41, 2.83; P < 0.0001) and expulsion time (days) of distal ureteral stones (mean difference [MD] −1.72, 95% CI −3.27, −0.18, P = 0.03) indicated that naftopidil was more effective than control. Based on the expulsion rate (RR 1.05, 95% CI 0.74, 1.48; P = 0.80), expulsion time (days) (MD 0.18, 95% CI −0.49, 0.85; P = 0.59), and number of pain episodes (P = 0.87), naftopidil was comparable to tamsulosin. A little lower adverse effect rate was observed with naftopidil compared with tamsulosin (RR 0.47, 95% CI 0.23, 0.94; P = 0.03).
Conclusions:
In terms of efficacy for distal ureteral calculi, naftopidil would be superior to control and comparable to tamsulosin; moreover, the safety profile of naftopidil might be superior to that of tamsulosin. We conclude that naftopidil might be a powerful candidate in MET for distal ureteral stones.
Introduction
U
Over the past few years, medical expulsive therapy (MET) using anticholinergics, nonsteroidal anti-inflammatories, corticosteroids, calcium channel blockers, alpha 1 (α1) adrenergic receptor antagonists, or combinations of these agents has been demonstrated to be a cost-effective option for promoting spontaneous expulsion of ureteral stones. 3,9 Tamsulosin, an α1A/1D-selective blocker, has been extensively researched for this indication, with meta-analyses confirming its efficacy for the resolution of distal ureteral calculi. 10,11 Another agent, the specific α1D-selective blocker, naftopidil, has also been identified as effective in the treatment of lower urinary tract symptoms for males with benign prostatic hyperplasia. 12 However, naftopidil displays greater selectivity for the α1D-adrenoceptor, for which it has ∼3-fold and 17-fold higher binding affinities than for α1A and α1B, respectively. 13 Based on this observation, it might be expected that naftopidil could be effective for MET in distal ureteral calculi, perhaps even showing higher efficacy and fewer side effects than current treatments.
We therefore conducted this systematic review to assess the safety and efficacy of naftopidil compared with control or tamsulosin for use in MET of distal ureteral stones.
Methods
Search strategy
A systematic literature search was performed up to June 15, 2016, using the Cochrane Central Register of Controlled Trials, Medline, Embase, and Google Scholar databases. No language restrictions were used during the searches, and the following keywords were used in combination with both medical subject heading terms and text words: naftopidil plus ureteral calculi or distal ureteral stone or urolithiasis plus medical expulsion therapy plus randomized controlled trials (RCTs). Additional studies were retrieved using the reference lists, and urology journals were manually scrutinized for published relevant studies.
Study selection and data extraction
Studies were included if the following criteria were met: (1) the study was a RCT; (2) included patients were found to have a single, unilateral, symptomatic distal ureteral stone that measured ≤10 mm; (3) treatment interventions were either naftopidil compared with a control group (WW or standard therapy [ST], where the latter consisted of the use of painkillers, antispasmodics, sedatives, and antibiotics), or naftopidil compared with tamsulosin; and (4) the studies provided at least one of the predefined outcome measurements. Studies were excluded if: (1) they were quasi-RCTs or not RCTs; and (2) patients had multiple stones, severe incarcerated stones, a history of distal ureteral surgery, renal colic for more than 24 hours, renal dysfunction, urinary tract infection, severe hydronephrosis, pregnancy, diabetes, previous therapy for the stone, a solitary kidney, or were receiving treatment with an α-receptor antagonist or a calcium antagonist. The selection of studies, abstracts, and full articles was performed by two independent reviewers (L.G. and J.H.L.). If there was any discrepancy, consensus was reached by discussion. Data from the included trials were independently extracted by two investigators (Z.T. and F.Q.), and discrepancies were resolved with the aid of a third reviewer (J.Y.). The corresponding authors of original studies were contacted for missing information where necessary.
The following information was extracted from the included trials: first author, year of publication, intervention, control, total number of patients, included patients, duration of treatment, and outcome data. The following outcome measures were defined from the included studies: (1) Stone expulsion rate (SER): the percentages of patients who expelled stone at the end of the follow-up. (2) SER hazard ratios (HRs): the HRs of expulsion analyzed by Multivariate Cox proportional hazards regression models. (3) Stone expulsion time (SET): self-report expulsion time when patients expelled stone. Expulsion was confirmed by imaging studies to be more accurate. (4) Number of pain episodes (NPE): the NPE in all of the patients. (5) Adverse effects (AEs): the number of patients with dizziness, fatigue, constipation, and other effects accompanying treatment.
Among the outcomes, SER, SET, and AEs were defined the primary.
Bias assessment
The Cochrane risk of bias tool was used to assess the quality of the included studies. For each study, the following questions were considered: (1) “Was sequence generation adequate?”; (2) “Was there allocation concealment?”; (3) “Was there blinding of participants and personnel?”; (4) “Was there blinding of the outcome assessment?”; (5) “Were incomplete outcome data addressed?”; (6) “Was the study free of selective reporting?”; and (7) “Was the study free of other bias?” Bias for each factor was described as a low, high, or unclear risk of bias. Two investigators (L.G. and Z.T.) independently assessed the quality of all the studies, and any discrepancy was resolved in consultation with a third investigator (J.Y.).
Statistical analysis
Statistical analysis was performed by Review Manager Version 5.3 (Cochrane Collaboration, Oxford, United Kingdom). In the summary analysis, the risk ratio (RR) was used to evaluate dichotomous data (SER, AEs), and weighted mean differences (MDs) were used for the continuous data (SET, NPE). HR was also used to evaluate the probability of expulsion, SER (HR), in our meta-analysis. As a result, two forest plots were made to discuss the SER outcome considering that two types of data couldn't be synthesized in one forest plot.
Heterogeneity of the study results was assessed using the Mantel–Haenszel χ2 test and the I2 statistic. When the I2 value was <50% and the P value was >0.10, heterogeneity was considered acceptable, but an I2 > 50% was taken to indicate high levels of heterogeneity. A fixed-effects model was applied when there was no heterogeneity, and a random-effects model was applied when heterogeneity was >50%. Subgroup analysis was performed to explore potential heterogeneity. A P value <0.05 was considered statistically significant, and 95% confidence intervals (CIs) are given.
Results
Search results and study characteristics
The database search yielded 619 articles, and additional 7 studies were identified manually. After duplicates were removed, 409 studies remained and a further 385 studies were excluded after reviewing the titles and abstracts. Finally, after the full texts of 24 remaining citations were screened, only 7 clinical trials 14 –20 were included in the systematic review (Fig. 1). Among them, 6 trials 14,16 –20 involving 385 patients compared naftopidil against controls, and 2 trials 15,19 compared naftopidil with tamsulosin. The studies included in our meta-analysis are summarized in Table 1. The definitions and methods of SER and SET across the six trials were listed in Appendix Table 1.

Flow diagram of meta-analysis.
AEs = adverse effects; HR = hazard ratio; NPE = number of pain episodes; RCT = randomized controlled trial; SER = stone expulsion rate; SET = stone expulsion time; ST = standard therapy.
Risk of bias
As shown in Figure 2, three included studies 16 –18 did not describe their randomization methods, so had unclear bias risk when assessing the adequacy of sequence generation. Two studies 14,15 described the method of allocation concealment, but the others did not. Only one trial 14 showed low risk in the blinding domain, and all others had unclear risk. Five trials 15,16,18 –20 reported that all patients completed the studies without discontinuation. One study 17 reported that 2/70 patients were excluded because they withdrew their consent before the medication. In the other study 14 performing on an intention-to-treat basis, 3/92 patients were excluded. So attrition bias was low risk. A high risk of reporting bias was found in three studies 16 –18 as it explicitly did not report all outcomes based on their design. All included studies described their methods sufficient enough to exclude other sources of bias.
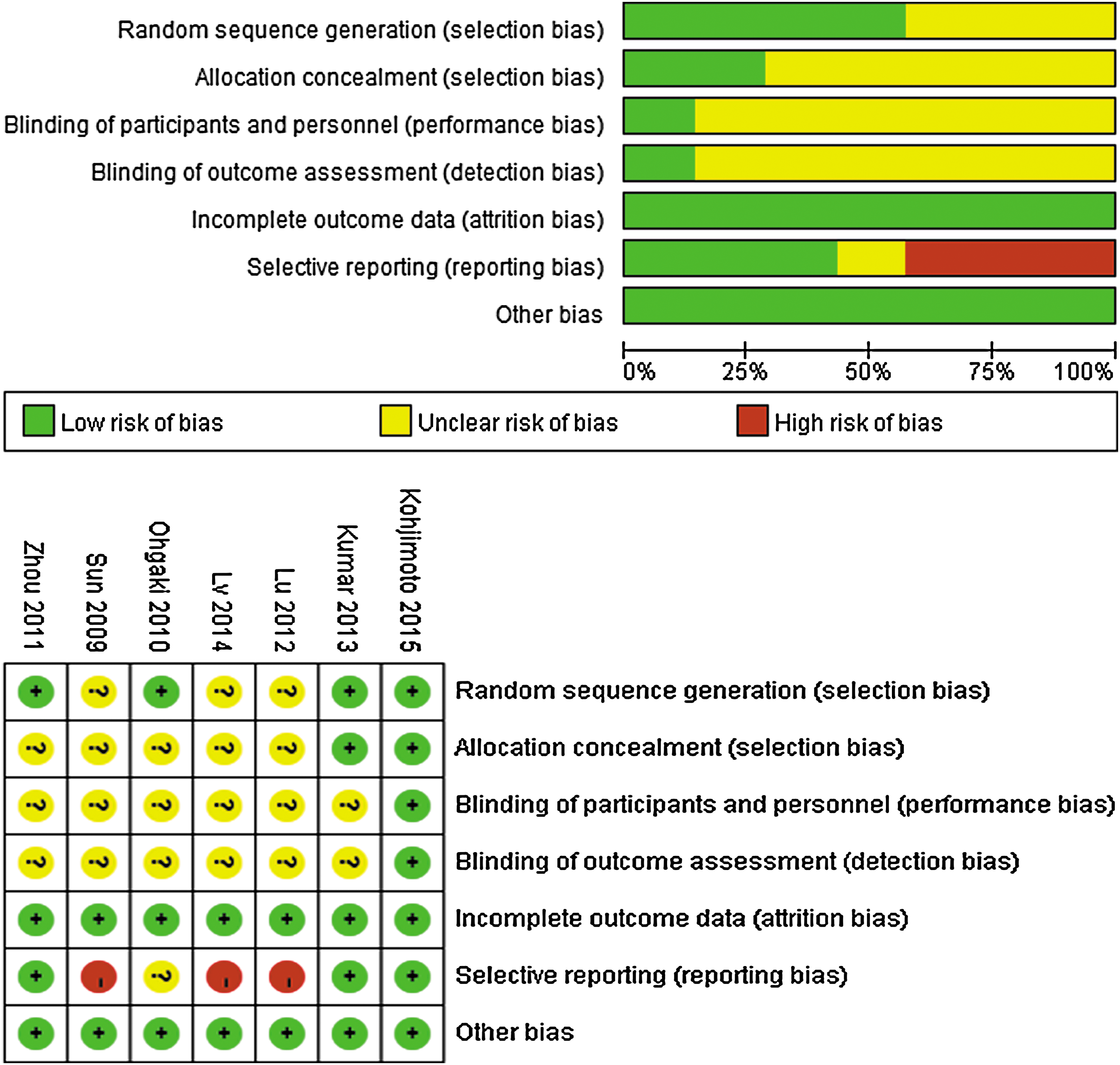
Risk of bias summary for included studies.
Studies comparing naftopidil with control groups
Six RCTs 14,16 –20 assessed the most important outcome, SER, with discontinuation rate of 2.1%, 0%, 0%, 0%, 0%, and 0% in the naftopidil group, respectively, and 4.3%, 0%, 5.7%, 0%, 0%, and 0% in the control group, respectively. Among them, four 16 –19 provided dichotomous data for the number of patients who expelled stone using RR analysis. Three trials 14,18,20 reported the SER outcome with HR based on multivariate Cox proportional hazards regression models. The pooled RR was 2.00 (95% CI 1.41, 2.83; P < 0.0001; I2 = 61%; Fig. 3.1) in favor of naftopidil over the control group. We then performed subgroup analysis because the I2 value indicated high levels of heterogeneity, which indicated that naftopidil had superior SER compared with the ST groups (RR 1.57, 95% CI 1.24, 2.00; P = 0.0002; I2 = 0%; Fig. 3.1.1) and WW groups (RR 2.74, 95% CI 1.87, 4.01; P < 0.0001; I2 = 0%; Fig. 3.1.2). The pooled HR of 2.62 (95% CI 1.38, 4.95) for the SER favored naftopidil over control (P = 0.003; I2 = 56%; Fig. 3.2). In the subgroup analysis, naftopidil was associated with a superior SER compared with either ST (HR 1.90, 95% CI 1.19, 3.03; P = 0.0007; I2 = 0%; Fig. 3.2.1) or WW (HR 5.26, 95% CI 2.30, 12.02; P < 0.0001; I2 not applicable; Fig. 3.2.2).
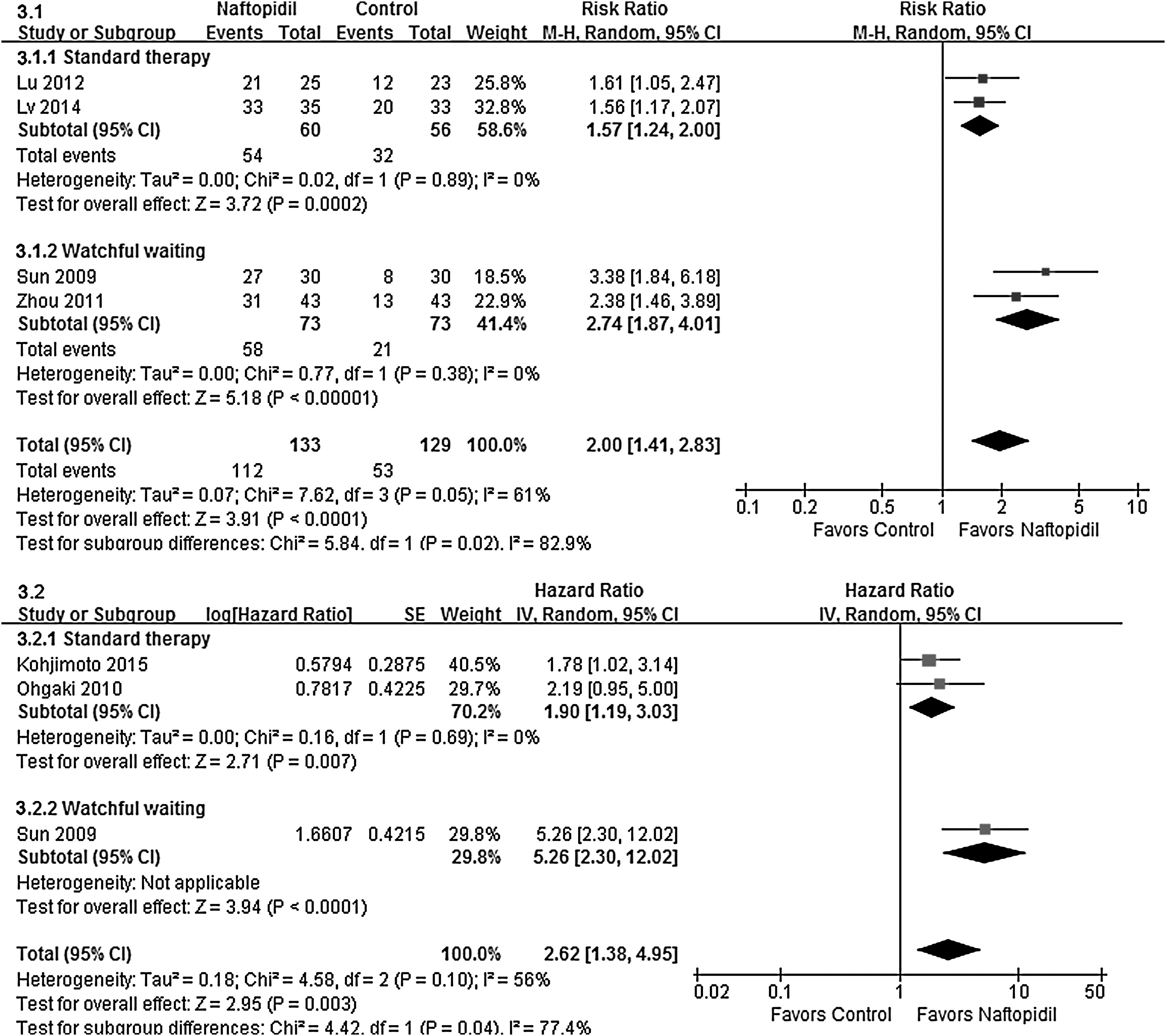
SER (analyzed by RR) (3.1) (3.1.1: Standard therapy; 3.1.2: Watchful waiting) and SER (analyzed by HR) (3.2) (3.2.1: Standard therapy; 3.2.2: Watchful waiting) of naftopidil vs control. HR = hazard ratio; RR = risk ratio; SER = stone expulsion rate.
Five trials reported the SET with discontinuation rate of 2.1%, 0%, 0%, 0%, and 0% in the naftopidil group, respectively, and 4.3%, 0%, 5.7%, 0%, and 0% in the control group, respectively. Three of them 16,17,19 provided the average time directly. The other two studies 14,18 reporting the median time exhibited the Kaplan–Meier curve by which mean value and standard deviation value can be estimated indirectly. Thus, five RCTs 14,16 –19 were included to the analysis of SET. This meta-analysis demonstrated that naftopidil was associated with a significant decrease in SET compared with controls (MD −1.72, 95% CI −3.27, −0.18; P = 0.03; I2 = 75%; Fig. 4.1). Subgroup analysis also revealed a statistically significant decrease in SET in the ST group (MD −2.80, 95% CI −3.89, −1.70; P < 0.00001; I2 = 0%; Fig. 4.1.1). However, no significant difference was found in the WW group (MD −0.57, 95% CI −2.90, 1.76; P = 0.46; I2 = 81%; Fig. 4.1.2).
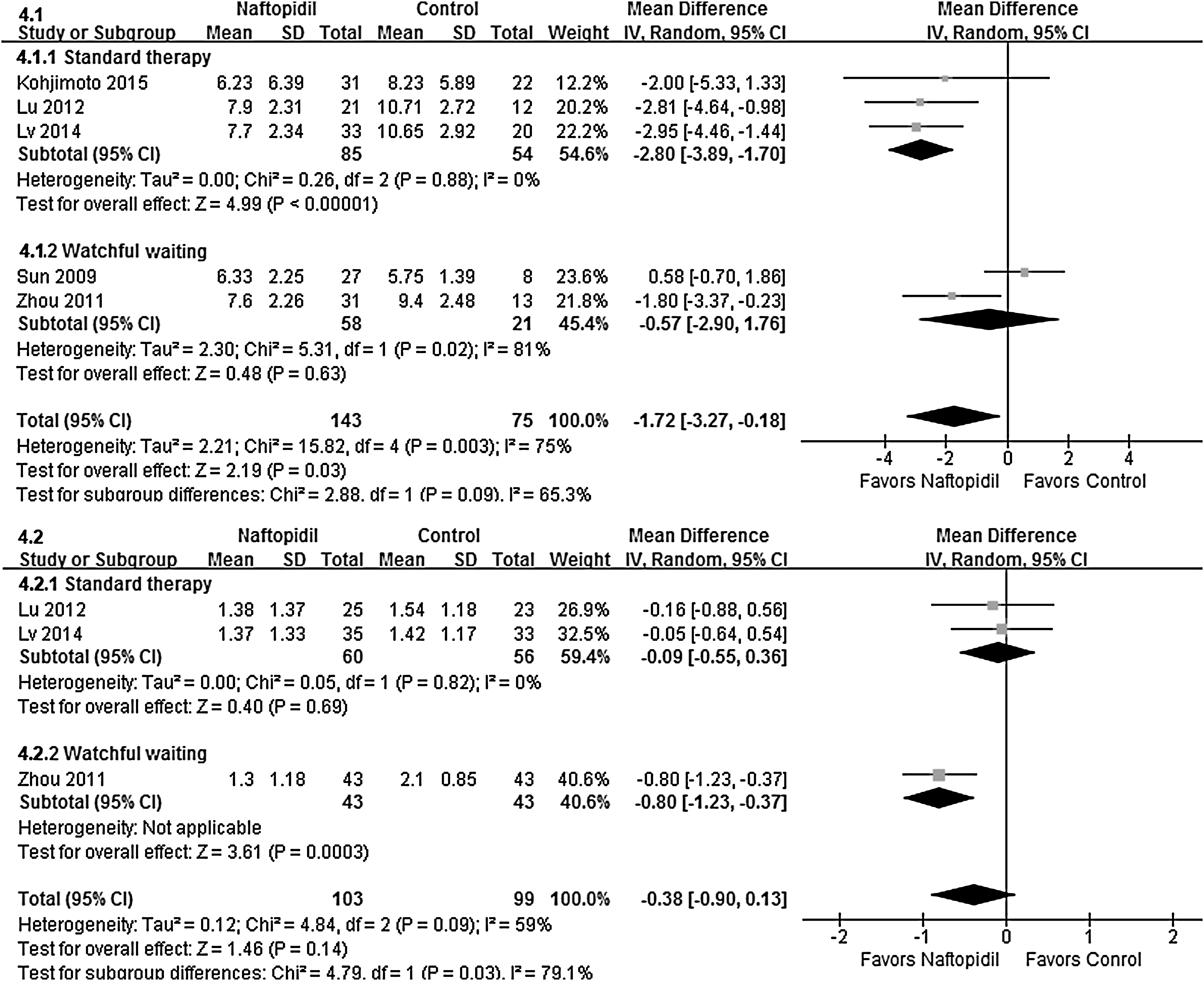
SET (4.1) (4.1.1: Standard therapy; 4.1.2: Watchful waiting) and NPE (4.2) (4.2.1: Standard therapy; 4.2.2: Watchful waiting) of naftopidil vs control. NPE = number of pain episodes; SET = stone expulsion time.
Three studies 16,17,19 of 202 patients (103 in the naftopidil group and 99 in the control group) contributed to the analysis of pain episodes. All the discontinuation rates were 0. The pooled MD for NPE (−0.38, 95% CI −0.90, −0.13; P = 0.14; I2 = 59%; Fig. 4.2) showed that there was no significant difference between the two groups. In the subgroup analysis, no significant difference was found in the ST group 16,17 (MD −0.09, 95% CI −0.55, −0.36; P = 0.69; I2 = 0%; Fig. 4.2.1), but a study comparing naftopidil with WW 19 indicated that naftopidil reduced the NPE (MD −0.80, 95% CI −1.23, −0.37; = 0.0003; I2 not applicable; Fig. 4.2.2).
Three studies 14,18,19 reported the number of patients with total AEs with discontinuation rate of 2.1%, 0%, and 0% in the naftopidil group, respectively, and 4.3%, 0%, and 0% in the control group, respectively. Two RCTs 16,17 reported dizziness, fatigue, and constipation, which were the most common AEs, but did not provide the total AEs. Although the authors were contacted for additional information, the attempts were unsuccessful. Figure 5.1 shows that 14 of 119 patients suffered AEs while receiving naftopidil compared with 1 of 119 in the control group (RR 7.50, 95% CI 1.75, 32.16; P = 0.007; I2 = 0%; Fig. 5.1), which meant that the AEs rate of naftopidil group was significantly higher than the control group. The AEs associated with naftopidil are summarized in Figure 5.2 to 5.5. Dizziness, fatigue, and constipation, with pooled RRs of 1.07 (95% CI 0.57, 2.01; P = 0.83; I2 = 17%; Fig. 5.2), 1.23 (95% CI 0.48, 3.25; P = 0.67; I2 = 0%; Fig. 5.4), and 0.84 (95% CI 0.33, 2.15; P = 0.72; I2 = 0%; Fig. 5.5), respectively, indicated no significant differences. By contrast, the naftopidil group had a slightly increased risk of headache compared with the control group (RR 6.03, 95% CI 1.10, 33.01; P = 0.04; I2 = 0%; Fig. 5.3). However, AEs caused by naftopidil were generally mild and did not require cessation of therapy in any patient of all the included trials.
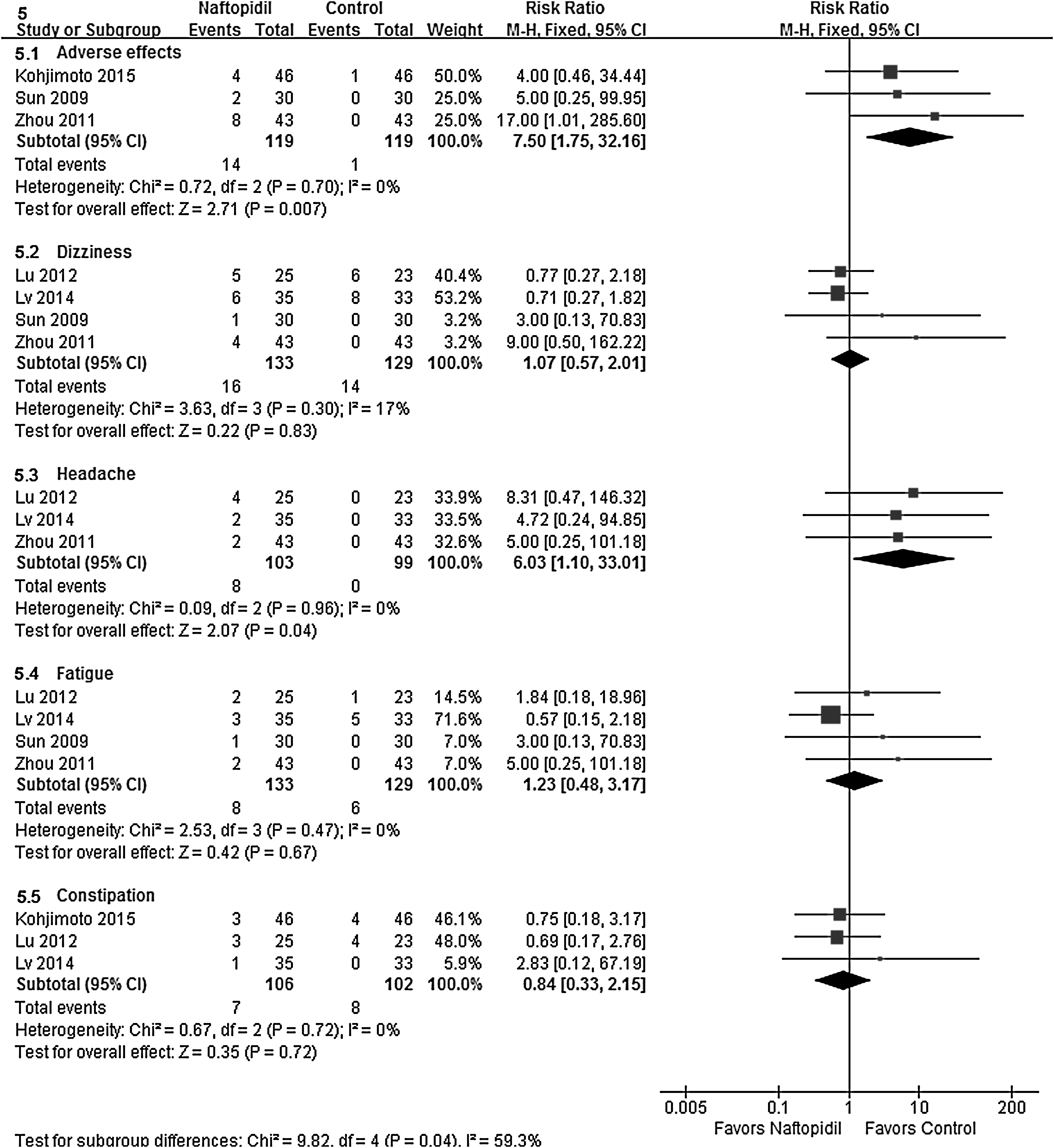
AEs of naftopidil vs control, respectively (5.1: Adverse effects; 5.2: Dizziness; 5.3: Headache; 5.4: Fatigue; 5.5: Constipation). AEs = adverse effects.
Naftopidil compared with tamsulosin
Two studies were included in the comparison of naftopidil with tamsulosin. 15,19 All the discontinuation rates were 0. Among the two trials, heterogeneity (i.e., the I2) was 78%, 0%, and 0% for the assessment of SER, SET, and NPE, respectively. As shown in Figure 6.1, the pooled RR for SER was 1.05 (95% CI 0.74, 1.48; P = 0.80), indicating that naftopidil had a comparable effect to tamsulosin on the expulsion rate. Figure 6.2 shows the pooled MD data for the SET, with no significant difference between naftopidil and tamsulosin (MD 0.18, 95% CI −0.49, 0.85; P = 0.59). In the assessment of NPE, the pooled RR was 0.02 (95% CI −0.27, 0.31; P = 0.87; Fig. 6.3), indicating no significant difference between the treatments.

SER (6.1), SET (6.2), NPE (6.3), and AEs (6.4) (6.4.1: Adverse effects; 6.4.2: Dizziness; 6.4.3: Retrograde ejaculation) of naftopidil vs tamsulosin, respectively.
A lower AE rate was observed with naftopidil compared with tamsulosin (RR 0.47, 95% CI 0.23, 0.94; P = 0.03; I2 = 0%; Fig. 6.4.1). However, neither dizziness, which is one of the most common AE, (RR 0.61, 95% CI 0.08, 4.57; P = 0.63; I2 = 0%; Fig. 6.4.2) nor retrograde ejaculation (RR, 0.55; 95% CI 0.19, 1.63; P = 0.28; I2 = 0%; Fig. 6.4.3) was significantly different between the groups.
Discussion
MET, particularly with α1-adrenergic receptor antagonists, has recently emerged as an alternative strategy to promote the expulsion of small distal ureteral stones and reduce the complication rate. 3,9 Malin and colleagues. 21 first characterized adrenergic receptors in the human ureter in 1970. Blockers of the α-adrenoceptor act by promoting relaxation of the distal human ureter, stabilizing peristalsis by reducing ureteral smooth muscle tone, and by inhibiting disorganized uncoordinated muscular activity. 22 These actions can, in turn, help facilitate the passage of a stone. The α1-adrenergic receptors have been classified into three subtypes, α1A, α1B, and α1D, by the International Union of Pharmacology. 23 Even though some studies have indicated that the α1A subtype plays the most significant role in ureteral contraction, it is the α1D that is most prevalent, especially in the distal ureter. 24 –26 Accordingly, an α1D-adrenoceptor blocker could plausibly be of benefit for the expulsion of distal stones. Specifically, we expected that naftopidil, a specific α1D-adrenoceptor blocker, could be more effective than tamsulosin, an α1A/1D-selective blocker, which is currently the most commonly used agent for MET. 3
This meta-analysis revealed that naftopidil was certainly effective in improving the SER and SET in patients with distal ureteral stones compared with controls. Indeed, the SER with naftopidil was 84.2% in the distal ureter, which was approximately twice that seen in the control group. Studies 14,18,20 in which Kaplan–Meier curves were plotted to assess the cumulative SET for each group over time have also demonstrated the efficacy of naftopidil compared with controls. Equally, our data indicated that naftopidil reduced the SET compared with ST. Moreover, no significant difference was found in the WW group. Sun and colleagues 18 found that naftopidil did not decrease the SET, which was not in accord with other trials.
As for NPE, there was no significant difference compared to ST. Because tolterodine and celecoxib have been reported to improve pain episodes effectively, 27,28 we assumed their use in ST may have explained the weaker pain-reducing effect of naftopidil compared with ST. 16,17 High-quality RCTs are needed that compare naftopidil with WW, and these should focus on the NPE.
In addition, naftopidil had similar effects on the SER, SET, and NPE compared to tamsulosin. The SER in patients with distal ureteral stones treated with naftopidil was 79.5%, which was only slightly higher than that for tamsulosin (76.5%), indicating that there was no significant advantage for naftopidil over tamsulosin in terms of efficacy for distal stones. However, when comparing tamsulosin with naftopidil for upper and lower ureteral stones, Meena and colleagues 29 reported SERs of 76% and 56% with tamsulosin and naftopidil, respectively. Tsuzaka and colleagues 26 also reported that the SER with naftopidil was no higher than that for silodosin, another α1A/1D-selective blocker. We assumed that the different distributions of α1A and α1D adrenergic receptors in the human ureter might explain this finding. More trials are needed that compare naftopidil with tamsulosin to explore whether α1A- or α1D-adrenergic blocking therapy is superior for MET of distal ureteral stones.
Commonly reported AEs of α1-adrenoceptor blockers include dizziness, headache, asthenia, postural hypotension, syncope, rhinitis, and sexual dysfunction. 30 In terms of safety, even though naftopidil showed no significant difference in the incidence of dizziness and retrograde ejaculation compared with tamsulosin, the overall incidence of AEs was much less for naftopidil (10.8%) than for tamsulosin (23.5%) in our analysis. Thus, our results indicated that naftopidil may be safer than tamsulosin. However, naftopidil still had a higher incidence of AEs (including headache) compared with controls, even though no significant difference was observed in the incidences of dizziness, fatigue, or constipation. Moreover, no relevant events were observed in some trials, but we think this was probably because of the short duration of use. From a clinical safety perspective, it was notable that AEs were generally mild in the treatment groups and that none required the cessation of therapy.
To our knowledge, this is the first meta-analysis to study the efficacy and safety of naftopidil, compared to control or tamsulosin, for expulsive therapy of distal ureteral stones. However, several limitations must be taken into consideration. First, some included studies were not of a high quality with insufficient allocation concealment, unclear blinding, and selective reporting outcomes. Second, the number of included trials was small. Third, regarding the small number for pooled estimate of each outcome, it is hard to make funnel plots, which indicate a potential risk of publication bias. Fourth, potential differences in stone size, ST, outcome measurements such as self-report form about SET, medical doses, and follow-up period may all increase the heterogeneity. To decrease this heterogeneity, we conducted subgroup analyses of the ST and WW groups when comparing naftopidil with control. A sensitivity analysis was also applied to explore the reliability of the meta-analysis results, which showed that all conclusions were stable and unaffected by the potential differences.
Considering that the overall quality of the body of evidence is not high, more high-quality trials are needed with larger samples to address the efficacy and safety of naftopidil in the distal ureter. As naftopidil is not available in the United States without approval by FDA, we advocate the use of naftopidil in more countries.
Conclusion
This meta-analysis indicated that naftopidil is superior to control and comparable to tamsulosin in terms of its efficacy for the management of distal ureteral stones. However, the safety profile of naftopidil appeared to be superior to that for tamsulosin. These findings indicate that naftopidil might be a promising MET for distal ureteral stones. High-quality trials are needed with larger samples to address the efficacy and safety of naftopidil in the distal ureter.
Footnotes
Acknowledgment
This article was supported by the Natural Science Foundation of China (Nos. 81170565 and 81270691).
Author Disclosure Statement
Abbreviations Used
Appendix
| Study | Follow-up (weeks) | SER | SET |
|---|---|---|---|
| Lu and coworkers. 16 | 2 | The percentages of patients who expelled stone on day 14. | Self-report expulsion time when patients expelled stone. Uloasis:rowasonography and KUB were performed to confirm the expulsion on days 7 and 14. |
| Lv and colleagues 17 | 2 | The percentages of patients who expelled stone on day 14. | Self-report expulsion time when patients expelled stone. Uloasis:rowasonography and KUB were performed to confirm the expulsion on days 7 and 14. |
| Ohgaki et al. 20 | 4 | The hazard ratios of expulsion on day 28. | Self-report expulsion time when patients expelled stone. Urinalysis, KUB, and uloasis:rowasonography were performed on days 1, 14, and 28. |
| Kohjimoto et al. 14 | 4 | The hazard ratios of expulsion on day 28. | Patients kept a diary to record the date and time of stone passage. Expulsion was confirmed weekly by urinalysis, abdominal uloasis:rowasonography, and plain abdominal X-ray or abdominal CT. |
| Sun and colleagues 18 | 2 | The percentages of patients who expelled stone on day 14. | Self-report expulsion time when patients expelled stone. Uloasis:rowasonography and KUB were performed to confirm the expulsion on days 7 and 14. |
| Zhou and associates 16 | 2 | The percentages of patients who expelled stone on day 14. | Self-report expulsion time when patients expelled stone. Uloasis:rowasonography and KUB were performed to confirm the expulsion on days 7 and 14. |
| Kumar et al. 15 | 4 | The percentages of patients who expelled stone on day 28. | Self-report expulsion time when patients expelled stone. Expulsion of stones was confirmed with plain X-ray, uloasis:rowasonography, or nonconoasis:rowast CT. |
CT = computed tomography; KUB = kidney ureter bladder X-ray; SER = stone expulsion rate; SET = stone expulsion time.