
Abstract
Objective:
Equipment and personnel contribute to the overall noise level in the operating room (OR). This study aims to determine intraoperative noise levels during percutaneous nephrostolithotomy (PCNL) and the effects of this noise upon intraoperative communication.
Methods:
A PCNL benchtop model was used to measure intraoperative noise and determine its effect upon communication in three progressively increasing sound environments (baseline ambient noise, ambient noise with PCNL equipment, and ambient noise with both PCNL equipment and music). Five trials with 20 different medical words/phrases were spoken by the surgeon and responses were recorded by the first assistant, anesthesiologist, and circulating nurse. In addition, noise levels during PCNL were compared to common environmental noise levels.
Results:
In the bench top model, noise levels were 53.49 A-weighted decibels (dBA) with ambient noise, 78.79 dBA with equipment in use, and 81.78 dBA with equipment and music. At the ambient noise level, the first assistant, anesthesiologist, and circulator correctly recorded 100%, 100%, and 96% of the words, respectively. The correct response rate by the subjects decreased to 97% (p = 0.208), 81% (p = 0.012), and 56% (p < 0.001) upon addition of PCNL equipment, and 90% (p = 0.022), 48% (p = 0.002), and 13% (p < 0.001) upon addition of music and PCNL equipment in the first assistant, anesthesiologist, and circulator, respectively. In the simulated OR model, PCNL noise level (81.78 dBA) was comparable to a passing freight train at 30 feet (82.2 dBA, p = 0.44).
Conclusion:
Noise pollution decreases effective intraoperative communication during PCNL. It is important for surgeons to understand the effect noise can have on attempted communication to prevent errors due to miscommunication. In addition, methods to decrease intraoperative noise pollution and improve communication in the OR could improve patient safety and outcomes.
Introduction and Objectives
W
Noise sources are often divided into two categories as follows: (1) noise from equipment and (2) noise resultant from staff behavior. 3 High-power suction devices, ultrasonic lithotripters, holmium lasers, and c-arms are just a few of the different pieces of urologic equipment used during percutaneous nephrostolithotomy (PCNL) that contribute to elevated OR noise levels. Staff-related behavior also adds to OR noise levels in the form of extraneous conversations, pager noises, phone conversations, and the playing of music. Studies have shown that music is played in as much as 63% of ORs during surgery. 4
Heightened noise levels in the OR can have a negative impact on communication, particularly when performing a surgical task. 5 Our study is the first to assess the impact of noise during PCNL upon communication of team members in the OR. In addition, we sought to compare baseline and maximum noise levels of PCNL to common environmental sources of noise.
Materials and Methods
Benchtop model
First, a benchtop model was developed to closely replicate an operating suite during PCNL. An OR used for PCNL was employed in the surgical model. Four physicians were positioned to simulate a surgical team, consisting of a surgeon, first assistant, anesthesiologist, and circulating nurse. With the surgeon as the reference point, the first assistant, anesthesiologist, and circulator were positioned 0.8, 1.8, and 2.5 m away, respectively (Fig. 1). Each listening subject was given an audiogram to ensure adequate hearing ability.
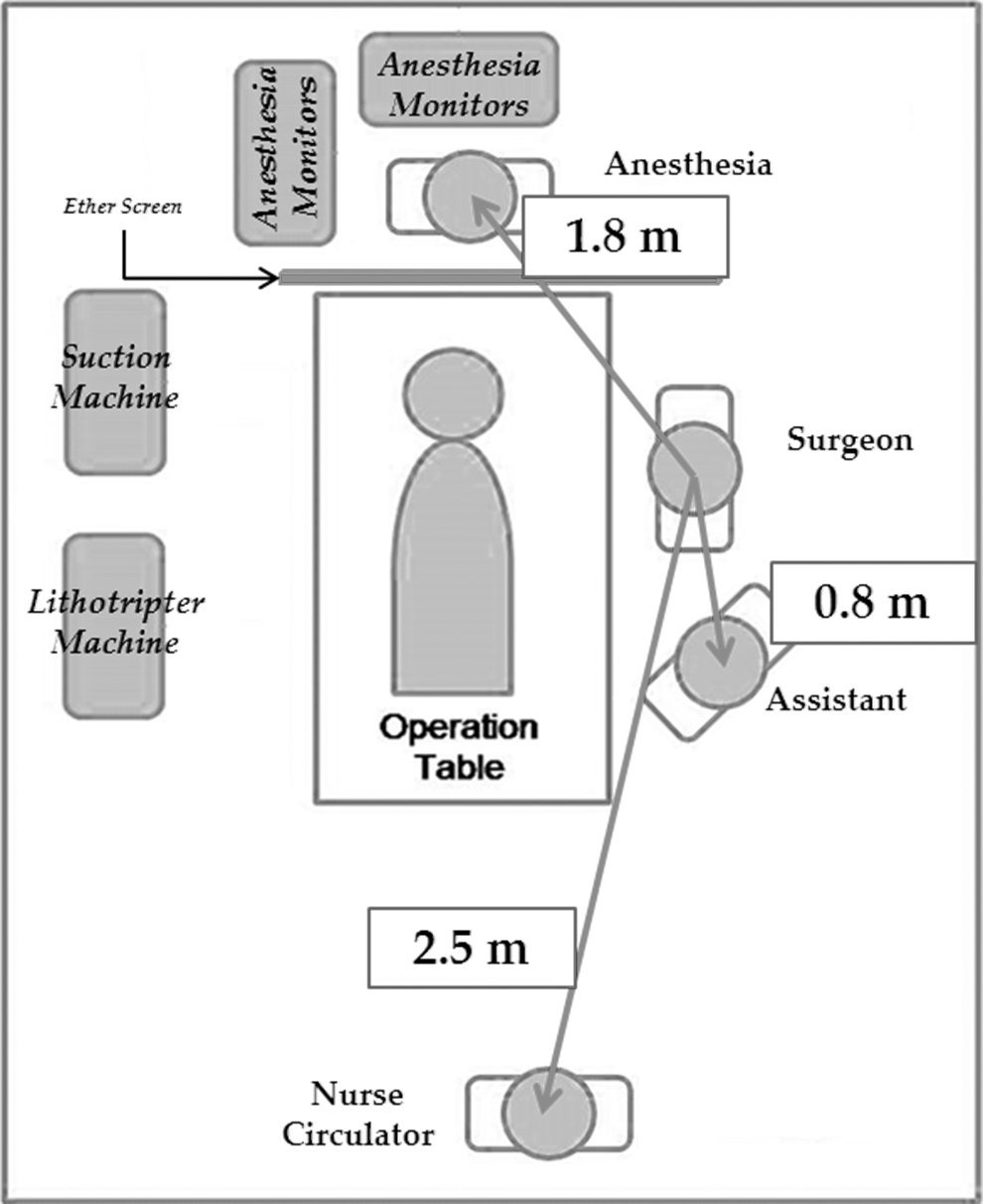
A diagram of the benchtop PCNL study setup. PCNL = percutaneous nephrostolithotomy.
Commonly encountered OR noise environments were then recreated as follows: baseline ambient noise, ambient noise with PCNL equipment, and ambient noise with PCNL equipment and music. Baseline noise was generated by room lights and the room's ventilation system. Added equipment included a Neptune 2 suction and its three attached suction tubes (Stryker, Kalamazoo, MI), a Karl Storz Endoscope Lithotriptor (El Segundo, CA), an AO4 pulse oximeter (Philips, Foster City, CA), and a Datex Aestiva 5 anesthesia suite (GE Healthcare, Pasadena, CA). These pieces of equipment were selected because they are the ones used at our institution during PCNL. Music played was “King of Anything” by Sara Bareilles, set to the same comfortable listening level through all trials. Twenty medical words or phrases were then spoken by the surgeon and recorded by the listening subjects at each of the three positions for each trial. Five trials, each with different words or phrases, were performed for each of the three different noise environments.
Environmental noise comparison
For the second phase of the study, we used the decibel meter to measure environmental noises for comparison to levels measured during the surgical model. Measurements of cars and pickup trucks driving 40 miles per hour (MPH) and freight trains travelling 45 MPH were recorded. All measurements were recorded at 30 feet. Twenty-five measurements were recorded for each environmental noise setting.
Sound
Sound levels were measured in dBA to most accurately represent the hearing of the human ear. 6 Noise measurements were reported in dBA and averages in equivalent continuous dBA level (Leq), the A-weighted equivalent for continuous noise level. 7 The decibel scale is a logarithmic measure used to quantify pressure created by various levels of sound. Therefore, increases of 3, 10, and 20 dB represent a 2-fold, 10-fold, and 100-fold increase of sound energy, respectively. For reference, a whisper is rated at 30 dB, normal conversation at 60 dB, and an ambulance siren at 120 dB. 8
Statistical analysis
Statistical analysis was done using Student's t-test for continuous variables and the chi-squared test for categorical variables in the IBM SPSS system (Version 22; Armonk, North Castle, NY) with p < 0.05 as significant.
Results
Benchtop model
The simulated PCNL showed average ambient noise alone to be 53.49 dBA. With machines in use, average sound level rose to 78.79 dBA. The addition of music caused the average sound level to jump to 81.78 dBA (Table 1).
dBA = A-weighted decibels; Leq = equivalent continuous sound level.
Bold values indicate level of significance compared to ambient noise.
After establishing noise levels of the different sound environments, we tested their effect on communication. At baseline noise level, the first assistant, anesthesiologist, and circulating nurse correctly recorded 100%, 100%, and 96% of the words, respectively. Once the equipment was turned on, the correct response rate of the first assistant, anesthesiologist, and circulating nurse decreased to 97% (p = 0.208), 81% (p = 0.012), and 56% (p < 0.001), respectively. Upon addition of music, a further decrease was noted with rates of 90% (p = 0.022), 48% (p = 0.002), and 13% (p < 0.001). Comparison of the equipment only rate to the equipment and music rate showed a significant decrease at the anesthesia (81% vs 48%, p = 0.010) and circulator (56% vs 13%, p = 0.001) positions, while the first assistant position trended toward significance (97% vs 90%, p = 0.052) (Table 2).
Bold values indicate statistically significant values.
Environmental noise comparison
In this model, total PCNL noise with equipment and music (81.78 dBA) was louder than a car (68.2 dBA; p < 0.001) or a pickup truck (69.6 dBA; p < 0.001) and similar to a freight train (82.2 dBA; p = 0.440) all at 30 feet (Table 3).
Compared to sound level of simulated PCNL with equipment and music.
PCNL = percutaneous nephrostolithotomy.
Discussion
There has been increasing appreciation of the harmful effects of noise pollution on caregiver health, cognition, and performance. Over the last 45 years, noise in the hospital has seen an 18 dB increase, 9 an almost 100-fold increase in sound pressure. Despite its reputation as a calm, quiet, and composed space, the OR is now recognized as one of the noisiest clinical environments. Some studies have noted peak levels exceeding 100 dBA and even high levels when unoccupied due to high-capacity air conditioning systems and other ambient environmental factors. 10
Noise-induced hearing loss (NIHL) is a concern when sound levels are elevated beyond 80 dB for a prolonged time or are >130 dB during one brief exposure. 11 Both the Occupational Safety and Health Administration (OSHA) and the National Institute for Occupational Health and Safety (NIOSH) make recommendations for prevention of work-related hearing damage. OSHA permissible exposure limit guidelines developed in 1981 state that employees are required to wear hearing protection when their 8-hour exposure level exceeds 85 dBA. Comparatively, NIOSH recommended that exposure limit guidelines are based on level and duration. Relating this to our model, 16 hours is the maximum amount of PCNL noise exposure a surgeon's ears can handle per day. 12
Previous studies have looked at average noise levels in the OR, with most values ranging from 60 to 70 dBA. 13 Values varied by subspecialty and one study noted that orthopedic procedures have the highest average levels at 66.3 dBA. In the same study, the average for urologic cases was 63.6 dBA. 9 It must be noted that these values can spike to much higher levels for short periods of time, such as when using drills in orthopedic cases where values can reach 96 dBA. 14 Other studies have looked at urologic procedures in particular. One study assessed occupational exposure during SWL and reported that it can average 83 dBA and reach as much as 112 dBA. 15
More recent studies have showed a marked reduction in sound pressure levels of SWL, with Terlecki and Triest reporting an average noise level of 79 dBA 16 and Soucy and colleagues reporting an average noise level of 77 dBA. However, Soucy also found that ultrasonic lithotripsy can reach levels of 93 dBA (CyberWand). 17 In agreement with more recent studies, our results show that average noise level in the OR during endourologic procedures do not exceed regulated limits, with the highest average level of 81.78 dBA in our benchtop model. However, this number is an average from the duration of the case. At various points, sound levels in the OR could have exceeded regulated limits, but were not captured by the decibel meter.
Miscommunication is one of the most frequently identified causes of medical errors. Greenberg and coworkers reviewed 258 surgical malpractice claims from 46 hospitals. They found 60 cases involving 81 communication breakdowns with 30% occurring in the intraoperative period. Ninety-two percent of all communication breakdowns were verbal. 18
In the OR, effective communication must exist between nurses, scrub technicians, surgeons, and anesthesia team members. The Environmental Protection Agency recommends that 24-hour average noise levels should not exceed 45 dB to avoid annoyance and maintain 100% speech intelligibility. World Health Organization guidelines recommend ≤55 dB 16-hour average noise levels for the same reason. 19
A study demonstrated that one must speak 10 to 15 dB higher than the surrounding noise level to achieve 90% accuracy in communication. 19 Relating this to our findings, during PCNL, a team member would need to speak at or above a volume of 95 dBA to be understood while equipment, music, and conversation are active. The 95 dBA level is equivalent to being inside an active MRI machine. 20 One survey of urologists noted that 15% believed external distractions, such as music and extraneous conversations, have caused at least one surgical complication in their OR. 21
Our study shows that the presence of music increases the noise level during endourologic procedures by 3 dB on average, a twofold increase in sound pressure. Music use is prevalent in the OR, with Ullmann and associates reporting that 63% of surgeons listen to music while operating. 4 Lee and colleagues noted that 57% of urologists listened to music in the OR. 21 However, there is no consensus on the effect of music on surgical outcomes. Surgeons self-report that music makes them calmer and more efficient. 4
Our results show that increasing noise levels can greatly affect communication in the OR. In the 1980s, there was an increased number of aviation accidents, and a common culprit was distraction of flight crews during critical times. To combat this, the Federal Aviation Administration (FAA) introduced the sterile cockpit rule, where pilots must refrain from all nonessential conversation and activity during flight that is not at an established cruising altitude. 22 Studies have looked at implementing similar concepts during anesthesia, cardiovascular surgery, and gastrointestinal procedures. 22,23 Wadhera and associates found that cardiovascular surgery instead has “critical events” such as initiation of cardiopulmonary bypass, crossclamp on, crossclamp off, and termination of cardiopulmonary bypass. After implementation of a communication protocol, frequency of ineffective communication during critical events decreased. 22 A group of gastrointestinal surgeons investigated their endoscopic procedures and detailed a change from 24 to 0 average procedural interruptions 9 months after implementing the “sterile cockpit” rule in their practice. 24 However, no studies have looked at attempting the “sterile cockpit” concept for endourologic procedures, but this question merits further research as distraction occurs once every 1.8 minutes. 25
We do not believe that music or conversation should be eliminated from the OR; we are merely trying to inform urologists of the fact that increased noise hinders communication among team members. During critical times, we suggest shutting music off and the ceasing of extraneous communication. Critical times to consider in endourology might include needle insertion and tract dilation, nephrostomy tube placement, tumor resection in partial nephrectomy with warm ischemia, and vascular control during donor nephrectomy. Another possible way to improve communication is using another FAA safety measure called positive exchange, a technique used when one pilot hands the flight controls off to another pilot. 26 In this scenario, when a surgeon asks for something, the listening party would repeat what they heard back to the surgeon, and if correct, the surgeon would repeat the phrase again, confirming that the listener heard correctly; thus creating a triple check system for communication, further minimizing the potential for miscommunication.
Our study is not free of limitations. The benchtop model was a simulated OR; as such, other factors present in a normal OR may not have been taken into consideration. Our trials only took into consideration equipment widely used at our institution. We used the Karl Storz Ultrasonic Lithotripter, but other models such as the CyberWand are considerably louder. 17 In addition, having one speaker say the words in our benchtop model may have introduced variation and bias; however, having a person rather than a prerecorded speaker more accurately simulated a true clinical scenario, as listeners use both verbal and nonverbal cues for comprehension.
Conclusions
Our study shows why noise levels should be a growing concern in the OR. Although not high enough to cause NIHL, noise pollution decreases effective communication during PCNL. It is important for surgeons to understand the effect noise may have on attempted communication, so that steps can be made to prevent error due to miscommunication. In addition, methods to decrease intraoperative noise pollution and improve communication in the OR could benefit patient safety and outcomes.
Footnotes
Acknowledgment
The authors thank Udochuckwu Oyoyo for providing statistical analysis.
Author Disclosure Statement
No competing financial interests exist.