
Abstract
Introduction:
Shared medical appointments (SMAs) have decreased patients' wait time to initial stone clinic appointment, standardized education, and increased exposure to nutrition therapy. We assessed the effectiveness of SMAs in reducing patients' urinary stone risk factors.
Materials and Methods:
Patients who established care in our stone clinic in an SMA between March 2012 and August 2015 were sequentially identified. After eliminating those without follow-up urine collections or whose urinary creatinine excretion between the two collections varied by >40%, 113 patients were included (M:F 63:50; 54 ± 15 years; body mass index [BMI] 30.6 ± 6.7). Results from before and after the SMA were compared with those from a similar cohort of patients who attended individual patient appointments (IPAs) for their first stone clinic visit (n = 63; M:F 37:26; 54 ± 14 years; BMI 30.1 ± 8.2). All patients received individualized medical therapy for stone prevention.
Results:
After medical and nutritional therapy, SMA patients with elevated risk(s) at baseline achieved significant reductions in uric acid, calcium, and sodium; p ≤ 0.001 for all. Those with low urine magnesium, low urine volume, low urine pH, and/or low urine citrate at baseline achieved increases; p ≤ 0.0008 for all. IPA patients with elevated baseline risk factors achieved reductions in oxalate and uric acid (p ≤ 0.004 for both) but neither calcium nor sodium and an increase in citrate (p = 0.003) but not magnesium.
Conclusions:
Patients from SMAs reduced their stone recurrence risk and compared favorably with patients from IPAs. Contributing factors may include shorter time from stone event to appointment and more standardized education for patients attending SMAs.
Introduction
N
A multidisciplinary stone prevention clinic has been available at our institution since 1995, and medical nutrition therapy has been included since its inception. Over time, however, timely access to the clinic decreased such that, in 2011, the average wait to establish care was >6 months. This was concerning as clinic “no-show” rates may be associated with a longer length of time between a patient's stone event and his/her initial stone clinic appointment. Others reported variable patient adherence to medical management for stone prevention and asserted that contributing factors might be age, socioeconomic status, and the waxing and waning of symptoms. 12 –14 Indeed, Lacy and colleagues confirmed that patients who felt better were more likely to not show for appointments. 15
As early prevention is most desirable, we sought to address the wait time from referral to actual appointment. After cause and effect analysis, we implemented shared medical appointments (SMAs) as a corrective action. 16 As previously reported, we reduced the wait time to appointment—shortening the time from stone event to the establishment of preventive care—and maintained high patient satisfaction. With this innovative model we have also ensured that all new patients receive nutritional care that includes a comprehensive review of dietary associations with kidney stones as well as individualized therapeutic regimens. Both patient satisfaction and knowledge of disease are as good as or better than among patients who attend individual appointments for their initial stone clinic visit. 16
As a next step in evaluating the efficacy of SMAs for establishing preventive stone care, we assessed whether patients attending SMAs achieved the same improvements in their stone risk factors as patients attending traditional individual appointments. To do this, we evaluated 24-hour urine risk factors before and after initial appointment and compared results between patients who attended SMAs and those from individual patient appointments (IPAs). Patient satisfaction with both SMAs and IPAs was assessed.
Materials and Methods
With IRB approval, patients' electronic medical records were used to identify those with both pre- and postappointment 24-hour urine collections. Clinical outcomes and satisfaction data were collected from patients who attended both SMAs and IPAs. The groups were characterized for gender, age, stone history, length of time between appointments, body mass index (BMI), and other factors (Table 1).
There were no significant differences between groups for any characteristics shown.
Stone composition analyses were available for 47% and 34% of patients who attended SMAs and IPAs, respectively, and were from before establishing care in the stone clinic.
CaOx = calcium oxalate; IPA = individual patient appointment; SMA = shared medical appointment.
Twenty-four hour urine collections were ordered for all patients before their appointments, regardless of appointment type. For the comparison of urinary risk factors, patients seen in SMAs and IPAs within the same time frame, that is, between 8 and 38 months before this analysis, were included (n = 287). Patients without follow-up urine collections within the study period (10% of patients from SMAs and 48% of patients from IPAs; total, 65) were excluded. Also, excluded were those without comparable pre- and postappointment 24-hour urine collections (urine creatinine varied by >40%; total, 46). Differences in urinary excretion factors were considered significant if p ≤ 0.05 (two-sided Student's t-test).
As described elsewhere, 16 patients calling to schedule an appointment to establish stone prevention were offered the opportunity to be scheduled in an SMA. The SMAs were 1-hour appointments and included as many as nine patients (average 5 patients/SMA). Patients were advised that follow-up appointments would be individual as SMAs are not currently offered for returning patients. The attending nephrologist and a registered dietitian (RD) were simultaneously present during each SMA. Medical prescriptions and/or dietary recommendations were made to patients on an individual basis in the SMA in a round-robin manner after reviewing (also in round-robin fashion) their medical and dietary histories as well as 24-hour urine risk factors. In addition, all SMA patients were guided through an interactive 20-minute presentation about general dietary influences on stone recurrence risk. As a comparison, patients from IPAs within the same time frame as the SMAs and who were seen by the same nephrologist and the same RD who saw patients in SMAs were identified; the same inclusion criteria as for patients from SMAs were used. Medical prescriptions and/or individualized nutrition therapy were provided to these patients as appropriate and as driven by clinical practice guidelines.
For the patient satisfaction study, data from a larger number of patients were assessed. Patients attending SMAs were offered patient satisfaction surveys from our earliest scheduled SMAs (October 2011) through April 2016. Surveys were distributed at the end of each SMA after providers had left the room. A similar survey was offered to patients attending IPAs beginning June 2015. Since then, satisfaction surveys were offered to all IPA patients at the conclusion of their appointments; all completed surveys were included in this analysis. Surveys were presented as optional, and patients were advised that providing their identities was optional. Using two-sided Student's t-tests, differences between groups—those who attended SMAs and those who attended IPAs—were considered significant if p ≤ 0.01.
Results
Patients from SMAs (n = 113) compared with patients from IPAs (n = 63) for gender distribution, age, BMI, and comorbidity (Table 1). The percentage of recurrent stone formers was similar between groups (Table 1). Other factors were also similar for groups, but time between appointments (7.9 ± 3.6 and 10 ± 5.3 months for SMA and IPA) and between the first and follow-up 24-hour urine collection (8.2 ± 3.3 and 11 ± 6.4 months for SMA and IPA) was shorter for patients from SMAs (p ≤ 0.003 for both; Table 1).
Twenty-four hour urine collections: overall results
Parameters from patients' pre- and postappointment 24-hour urine collections were averaged for each group; Table 2 provides these values and shows differences between groups in the preappointment collection for citrate and sodium. The table also shows differences between groups for citrate and sodium at the postappointment time point and identifies statistically significiant changes within groups for calcium (SMAs), oxalate (IPAs), pH (SMAs), volume (SMAs), and potassium (SMAs and IPAs).
Data shown are mean and SD. p values are from two-sided Student's t-tests and show differences between patients from SMAs and IPAs; differences for within-group changes are denoted with lettered superscripts. Time of 24-hour urine collection before initial appointment was not different between groups (p = 0.39), 1.9 ± 1.5 months for SMA and 1.7 ± 1.5 for IPA. Time between the initial 24-hour urine collection and the second (follow-up) collection was shorter for the SMA group, 8.2 ± 3.3 months, than for the IPA group, 10.6 ± 6.4 months (p = 0.001 for difference).
Bold values indicate statistically significant differences (p < 0.05).
Difference from within-group baseline value, 0.05 ≥ p ≥ 0.01, two-tailed paired Student's t-test.
Difference from within-group baseline value, p < 0.001, two-tailed paired Student's t-test.
Twenty-four hour urine collections: results of those with elevated baseline risk factors
In Figure 1, changes in urinary risk factors among subsets of patients who began with elevated urinary risk factor(s) are shown. Patients from SMAs with high urine calcium (n = 39, 34%), uric acid (n = 22, 19%), and/or sodium (n = 22, 19%) achieved significant reductions: 349–250 mg, 918–766 mg, and 261–186 mEq, respectively; p values for these changes are shown (Fig. 1). While urine oxalate was reduced (60–54 mg) in those with elevated oxalate (n = 41, 36%), this did not reach statistical significance. SMA patients with low urine volume (n = 74, 65%) and/or low pH (n = 21, 18%) achieved increases: 1.30–1.65 L and 5.41–6.01 (p ≤ 0.001 for both). SMA patients with low citrate (n = 33, 29%) and also those with low magnesium (n = 19, 17%) saw significant increases: 182–359 mg and 49–76 mg, respectively; p values for changes within these groups are shown (Fig. 1). Patients from IPAs who had elevated baseline 24-hour urine risk factors for oxalate (n = 27, 43%) or uric acid (n = 20, 32%) achieved significant reductions: 66–48 mg and 943–715 mg, respectively, and also increased citrate from 177 to 331 mg; p values for these changes are shown (Fig. 1). Both urine pH and volume increased among IPA patients with abnormal/low values (n = 10, 16%; and n = 37, 59%), and both changes were significant (p ≤ 0.001).

Patients from SMA and IPA who had abnormal 24-hour urinary risk factors at baseline. Results from 24-hour urine collections before and after either an SMA (first pair of bars for each parameter) or an IPA (second pair of bars for each parameter) in our multidisciplinary metabolic stone clinic are shown. Data represent mean (bars) ± SD (error bars) for patients with abnormal baseline values for any parameter. p Values are from paired t-tests within groups for each parameter and thus represent the average of within-person changes per group. IPA = individual patient appointment; SD = standard deviation; SMA = shared medical appointment.
Patient satisfaction surveys from larger group of stone clinic patients
Of total patient surveys offered, 429 were completed (291 from patients attending SMAs and 138 from IPAs); Table 3. Other than a few yes/no questions, respondents were asked to rank their satisfaction for a given clinical feature or component using a 1–5 Likert scale with 5 ranking highest (most true or favorable) and 1 ranking lowest (least true or favorable). Patients from SMAs rated their experience similarly to those who attended IPAs with a few exceptions (Table 3). Interestingly, ease of clinic check-in and helpfulness of clinic reception staff were rated higher (more favorable) by patients who attended SMAs. In contrast, patients who attended IPAs scored higher than their SMA counterparts for questions related to being encouraged to participate and fulfillment of their needs (Table 3). Responses were further characterized by calculating the percentage of those ranking items a 4 or 5, corresponding to very true and extremely true. Overall satisfaction with the appointment was comparable between groups (Fig. 2).
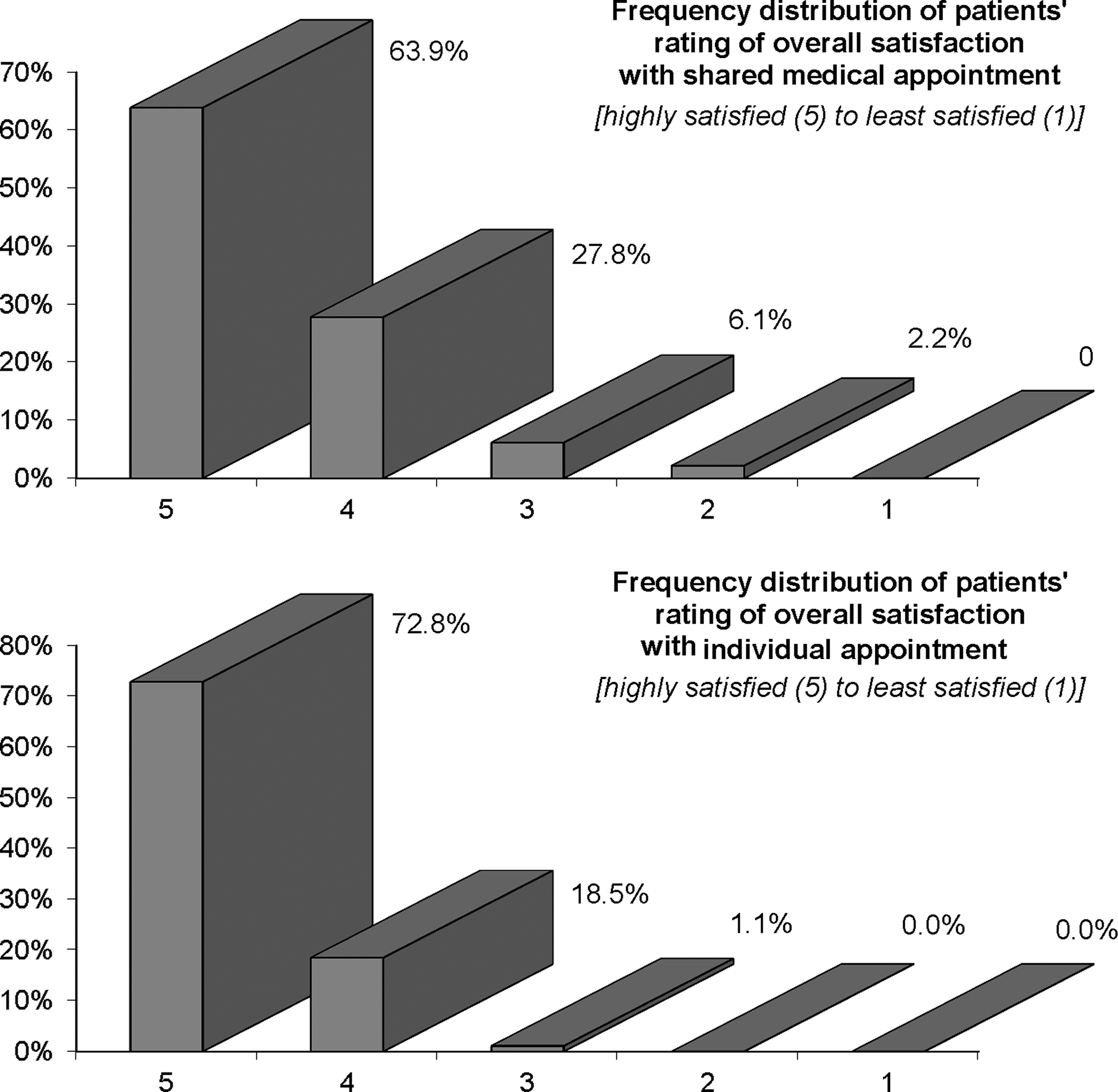
Patient satisfaction with SMAs compared with those who attended IPAs for their first visit to stone clinic. Data show the overall clinic experience of 291 patients who established preventive care in an SMA (top panel) and 138 patients who established care in an individual stone clinic appointment (bottom panel). The numbers on the x-axis correspond to the 5-point Likert scale used to assess overall satisfaction.
Data show results from patients from SMAs (n = 291 from October 2011 to April 2016) and those from IPAs (n = 138 from June 2015 to April 2016). p values ≤ 0.01 were considered significant.
Bold values indicate statistically significant differences (p < 0.05).
Discussion
We previously demonstrated that SMAs were acceptable for medical management, increased the proportion of those exposed to nutritional management, demonstrated similar or higher patient knowledge than IPAs, and reduced the wait time for an initial appointment from 180 to <90 days. 16 In the current study, we show that patients who attended SMAs for their initial stone clinic appointment achieved similar reductions in urinary stone risk factors as those who attended traditional individual appointments. We observed good satisfaction among patients attending both types of appointments but also differences between patients for specific aspects of their appointments.
Urinary risk factors are routinely assessed in the medical management of kidney stones, so this is a suitable outcome for comparing results from both appointment groups. Improvements in urinary risk factors were similar between groups (Table 2) overall. However, while group results are informative, perhaps more significant is how urinary risk factors changed among patients with risks at baseline. As shown in Figure 1, among patients with hypercalciuria, reductions in the urinary excretion of calcium and sodium were achieved in patients from SMAs but not IPAs. While both groups reduced urinary sodium, this change was significant only in the patients from SMAs. On the contrary, among those with hyperoxaluria at baseline (Fig. 1), urinary oxalate excretion decreased significantly in patients from IPAs but not SMAs. This may represent a limitation in the SMA format for counseling about dietary factors related to urinary oxalate excretion. Normalizing (which typically means increasing) dietary calcium intake and timing it with meals is a primary strategy by which to reduce oxalate absorption and urinary excretion. However, this idea is often contrary to what patients have been previously told; significant and individualized efforts to dispell preconceived notions are frequently required. It could be that the explanation of this principle in the SMA setting was not as effective as in individual counseling. However, another explanation is that the etiology of patients' hyperoxaluria varies widely and may, in addition to suboptimal calcium intake, include dysbiosis, malabsorption, excessive oxalate biosynthesis, high intake of oxalate or oxalate precursors, and/or vitamin B6 deficiency. The SMA format may not be as effective as individual appointments in counseling some of these patients, particularly if their underlying disorder is complex.
As part of ongoing quality improvement, we also examined patients' satisfaction with their stone clinic encounters, whether an SMA or IPA. Patient satisfaction is an important factor in the quality of care and is increasingly thought to be related to clinical outcomes. Our results identify areas for potential improvement. While satisfaction in both groups was quite high (Fig. 2), patients from IPAs scored significantly higher than patients from SMAs for (1) feeling their needs were met during the appointment, (2) feeling that staff were sensitive, and (3) being encouraged to participate (Table 3). While each patient in the SMA setting had a turn being discussed individually in front of others, and while both the physician and dietitian came to the SMAs with detailed medical histories on each patient, it could be that patients felt they received less attention than anticipated, leading some to feel their needs were unmet or that staff were not sufficiently attentive. This could be due, in part, to the fact that the before-appointment preparation and time spent by providers is basically invisible to patients. As to not feeling as encouraged to participate, the presentation format of the SMA may have promoted a more passive dynamic, even though repeated encouragements to ask questions and provide comments were made by the providers.
In contrast to these items, patients from SMAs were more satisfied than their IPA counterparts in the check-in process and for helpfulness of clinic reception staff. As a way to explain this, it is possible that patients attending SMAs were more promptly checked in and brought back to the conference room than IPA patients who may have had delays if providers were behind on their schedules.
Finally, while not statistically significant, there was a trend (p = 0.098) for more patients from SMAs to agree to start potassium citrate (Table 1). This phenomenon could be related to the joint presence of the physician and RD and the strong nutritional component of the SMA. The collaborative approach to decision-making in the SMA—visible to patients in real time—may have led patients to understand that nutritional strategies were fully considered before prescribing medication. Alternatively, as patients from SMAs may have been seen at a time closer to their stone event than patients from IPAs, their acceptance of medication therapy may have been more favorable. Either way, the early initiation of appropriate care may prevent future events. 17
Shortcomings of this study include lack of stone recurrence data and the constraints of the information retrievable from patient satisfaction surveys. To preserve the anonymous nature of the surveys, we could not link results to disease severity or other factors. Moreover, satisfaction data were provided by patients from IPAs only after timely access to the clinic had been improved due to the implementation of the SMAs (data not shown). This may have had a positive influence on satisfaction and could have masked lower satisfaction of patients in our stone clinic before the advent of the SMAs. Also, significant bias exists regarding patient decision to undergo SMAs vs IPAs. Finally, we did not track the rate of compliance with follow-up appointments beyond the study period, and this limits our comparison of the two appointment types. Although patients from SMAs appeared to have greater compliance with follow-up 24-hour urine collections than patients from IPAs, the time between appointments was shorter for patients from SMAs, and this may have influenced compliance. Moreover, we did not collect data for completion of follow-up 24-hour urine collections beyond the study period and thus likely did not capture the total number of patients who did eventually complete their second urine collection.
At this time, the SMA for patients initiating medical management in our stone clinic appears to provide equivalent care when compared with IPAs and is met with good patient satisfaction. SMAs and IPAs appear equally effective in achieving medical management goals. Future work should include effects on stone recurrence and factors affecting patients' expectations and satisfaction.
Conclusion
SMAs for kidney stone prevention have enhanced both patient access to appointments and provider productivity. Urinary risk factors for stone recurrence, with exception to management of higher urinary oxalate excretion, decreased among patients who established their preventive care by attending an SMA. Patient satisfaction was high in both groups but was higher in a few categories among patients from IPAs. SMAs appear to be a promising option for busier stone clinics.
Footnotes
Author Disclosure Statement
No competing financial interests exist.