
Abstract
Purpose:
The aim of this study is to assess the effectiveness, safety, and reproducibility of the micro-ureteroscopy (m-URS) in the treatment of distal ureteral stones in women.
Materials and Methods:
A multicenter, prospective observational study was designed and conducted between March and December 2015. We included women having at least one stone in the distal ureter and being a candidate for surgical treatment using the 4.85F sheath of MicroPerc®. Patients with clinical criteria and/or laboratory analysis indicating sepsis or coagulation alteration were excluded.
Results:
Thirty-nine women were operated in eight hospitals. The profile of the patients was fairly homogeneous among hospitals. Only differences were found in age, preoperative stent, and the result of the previous urine culture. Immediate stone-free status was achieved in 88.2% and 100% 7 days after the procedure. 97.4% of patients did not present any complication in the postoperative period, with only one case with complication Clavien II. Postureteroscopic Lesion Scale (PULS) in 76.9% of patients did not show any injury, 20.5% had lesions grade 1, and grade 2 lesions 2.6%. As for the reproducibility of m-URS between hospitals, statistical analysis of the results showed differences between all the centers participating in the study.
Conclusions:
m-URS is an effective, safe, and reproducible technique that minimizes surgical aggression to the ureteral anatomy. Satisfactory and comparable results to “conventional” ureteroscopy were obtained in the treatment of distal ureteral stones in women, although clinical trials are needed. The reduction of the ureteral damage may reduce secondary procedures and increase the cost-effectiveness of the procedure.
Introduction
V
Ureteral stones generate the greatest morbidity. The therapeutic options are medical expulsive therapy (MET), or active treatment, either with extracorporeal shockwave lithotripsy (SWL) or ureteroscopy (URS). Although MET appears to be the most attractive option, 3 as the least interventional, its efficacy might be limited 4 even in stones smaller than 10 mm. Therefore, active treatment options for ureteral lithiasis are growing in popularity.
The objective of SWL is the external fragmentation of the stone, so the smaller fragments can then be spontaneously passed by the patient. In URS, the stone fragmentation occurs directly in the ureter, and its extraction is immediate. This is the primary advantage of URS over SWL, at the expense of higher morbidity. 5 One of the major advances in endourology to reduce iatrogeny while maintaining efficacy is the miniaturization of the endoscopic instruments. The use of smaller caliber ureteroscopes reduces ureteral damage, the risk of complications, and the need for postoperative catheterization, thereby improving the patient's quality of life after the procedure. 6,7 In 2015, we published our first experience in the treatment of distal ureteral lithiasis in women using micro-ureteroscopy (m-URS) with the retrograde use of the 4.85F 8 sheath from the micro-percutaneous (MicroPerc®) surgery set. 9
The aim of this study is to evaluate the effectiveness, safety, and reproducibility of this technique in the treatment of distal ureteral stones in women.
Materials and Methods
Study design
A multicenter, prospective observational study was designed and conducted between March and December 2015. The inclusion criteria were: woman over 18 years of age, having at least one stone of any size in the distal ureter, and being a candidate for surgical treatment according to the standard practice of each site, either scheduled or as an emergency. Patients with clinical and/or analytical sepsis criteria, patients with an irreversible clotting disorder, or patients who would not sign the informed consent to undergo the procedure were excluded. The ethical principles and recommendations of the Declaration of Helsinki were respected during this research.
Eight surgeons from different centers participated in the study. Between four and five operations were performed at each center. Three of the surgeons had prior experience in m-URS. The rest understood the material used and attended a workshop to learn the technique.
Surgical technique
The 4.85F sheath from the MicroPerc set and the 10,000 pixel, 120°, 0.9 mm diameter flexible optic system (PolyDiagnost) (Figs. 1 and 2) were used for m-URS. A three-arm luer lock adapter was connected to the sheath to insert the optics (through the middle arm), the irrigation (either with perfusion pump or gravity dripping) through one lateral arm, and the 230 laser fiber through a Tuohy Borst Adapter (Cook®) to avoid irrigation dripping through the third arm.
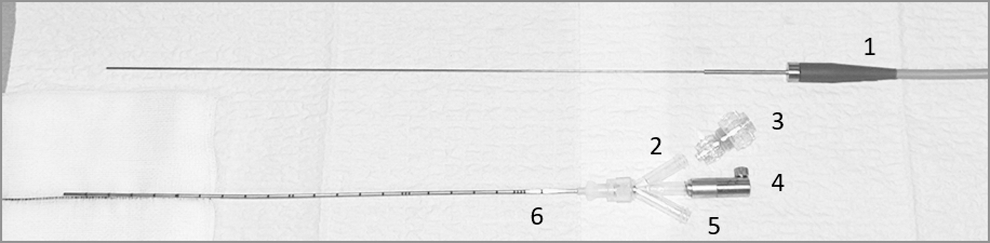
Equipment used in micro-ureteroscopy: 1, 0.9 mm diameter optic; 2–3, Luer Lock adapter; 3, Tuohy Borst Adapter; 4, optic adapter; 5, irrigation channel; and 6, 4.85F sheath of MicroPerc set.
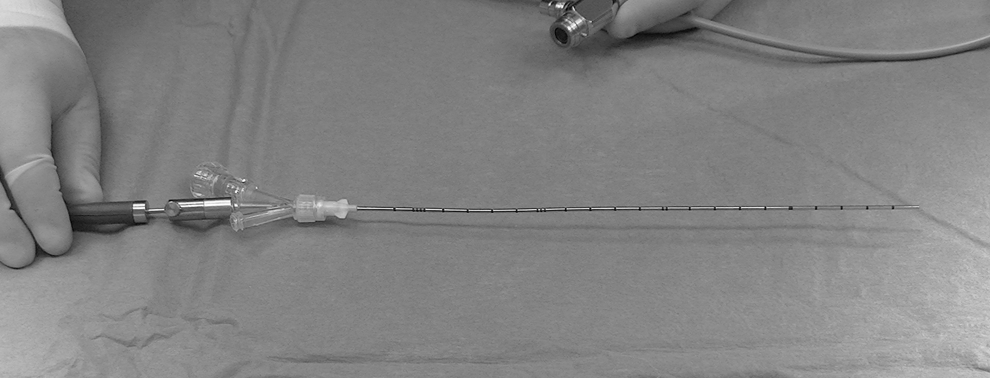
Material prepared for micro-ureteroscopy.
The use of accessory materials (safety guidewire or 1.3F stone basket), antibiotic prophylaxis protocols, anesthesia techniques, or the decision to insert a stent before surgery or afterward was left to the surgeons' criteria, according to their standard practice. Most of the times the sheath was inserted retrogradely in the ureter with neither need of meatus dilation nor safety guidewire. The entire procedure was performed under endoscopic vision (Fig. 3). Laser settings were adjusted to dust the stone and try avoiding the need for fragment removal.
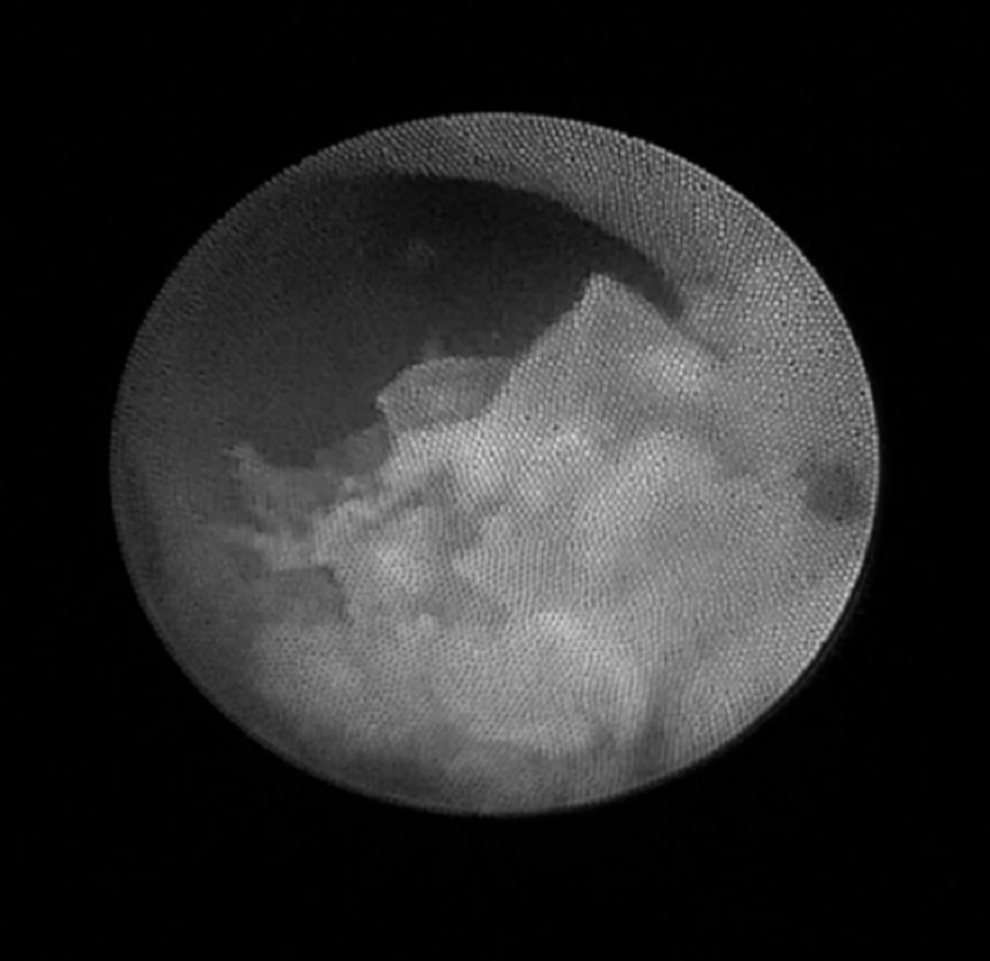
Endoscopic image during the procedure before start of dusting of a stone.
In those cases in which the surgeon observed difficulty in completely treating the stone with m-URS, the conventional ureteroscope could be used. We defined a “conventional” ureteroscope as that not designed a priori for use in pediatric patients (i.e., tip diameter greater than 7.5F).
Study variables
The independent variables consisted of: age, body mass index (BMI), diabetes history, use of antiplatelet or anticoagulant drugs, ASA classification, possible genitourinary malformations, characteristics of the stones, previous treatments for ipsilateral lithiasis, and the result of the previous culture.
The primary end points are encompassed under the study objectives. The effectiveness of the procedure was assessed through the number of immediately stone-free cases as observed through endoscopic and/or fluoroscopic study (Fig. 4) after the procedure and 7 days after the intervention through KUB of the abdomen. The safety of the technique was evaluated through the incidence of complications, using the modified Clavien–Dindo scale, and through the analysis of any ureteral damage caused, with the Postureteroscopic Lesion Scale, or PULS. In all cases, a renal ultrasonography and/or a computed tomography were performed 3 to 6 months after the procedure.

Intraoperative fluoroscopy, in which the sheath for micro-ureteroscopy is identified inside the left ureter during the treatment of a distal ureteral stone.
Other variables were the use or not of cystoscope, safety guidewires, “conventional” ureteroscope, or urinary catheter during the procedure. The duration of the intervention and the need to convert to conventional URS, as well as the reason, the need to use postoperative ureteral stent, and its duration, were also recorded.
Statistical analysis
The primary study variables were summarized using means as measures of central tendency and the 95% confidence interval (95% CI) as measure of dispersion for the quantitative variables and frequencies and percentages for the qualitative measures.
For the study of the reproducibility or homogeneity of the procedure, percentages were calculated for the qualitative variables for each one of the hospitals. To discuss the possible differences between the hospitals, the nonparametric statistics chi-square distance, symmetrical lambda, and the Goodman–Kruskal Tau were calculated. In the case of quantitative variables, medians per hospital were calculated. The nonparametric Kruskal–Wallis statistic was used to obtain possible differences between hospitals, in addition to the parametric, single-factor ANOVA procedure. The statistical package used was the SPSS 15.0 program.
To perform the analysis of the homogeneity of the results between the different hospitals, the sites that were required to use the cystoscope to remove a ureteral stent before the current procedure were excluded. A decision was made to also exclude the site that systematically uses a safety guidewire to perform the procedure and the site that, per protocol, leaves any ureteral stent inserted in situ for 14 days.
Results
The demographic characteristics of the study population are reflected in Table 1. The patient profile was fairly homogeneous among the hospitals (Table 2). Differences were only observed in age, having a preoperative stent and the result of the previous culture. While in one hospital the median age was 37 years, in another, it stood at 79 years. In half of the sites, no patient had preoperative stents, while in two sites, four and three women, respectively, had preoperative stents in place. Finally, in three hospitals, the previous culture was negative in all cases and, in another, all of the cultures were positive.
Quantitative variables are expressed as mean and 95% CI, while qualitative do in frequency and percentage.
Mean values.
ASA = American Society of Anesthesiologists; BMI = body mass index; CI = confidence interval.
Statistically significant value.
χ2 = chi-square; λ = Symmetric Goodman and Kruskal Lambda; τ = Hospital independent Goodman and Kruskal Tau; K-W = chi-square Kruskal–Wallis; df = degrees of freedom; NA = not available.
Previous treatments included six SWL performed no more than 1 month previous to the m-URS, one retrograde intrarenal surgery, and a percutaneous nephrolithotomy each. Finally, in two cases, an ipsilateral URS was done more than 4 years ago and in one case the URS was performed 2 weeks prior m-URS. Regarding surgeon's preferences for the m-URS technique (Table 3), the cystoscope was chosen in 2 of the 27 cases not bearing Double-J stent. In 94.3% (86.6%–100%), the meatus was accessed directly, with no safety guidewire. In four patients, 10.3% (0.8%–19.8%) of the total, the conventional ureteroscope had to be used. The reasons for using the ureteroscope were, in three cases, poor image quality and, in one case, the inability to mobilize an impacted stone using the m-URS equipment. In no case was it necessary to convert due to stone retropulsion to a level of the ureter where, due to the sheath's length, the stone was not reachable.
Measures calculated on the number of patients not previously carrying a Double-J stent. Quantitative variables are expressed as mean and 95% CI, while qualitative do in frequency and percentage.
PULS = Postureteroscopic Lesion Scale; URS = ureteroscopy.
In 35 patients (89.7%), the stone was dusted using the Holmium laser. In six renal units, a Double-J stent was inserted and, in five, an external straight ureteral stent was inserted for 24 hours. The ureteral stents were maintained for a mean of 3.5 days. The mean duration of the surgery was 35.8 minutes (95% CI 29.3, 42.2).
In terms of the effectiveness of m-URS, 30 patients (88.2%) were stone free immediately and 100% 1 week after the procedure. No retreatment was required in any case.
Regarding the safety of the technique, 97.4% of the patients showed no problems during the postoperative period, with a single case with Clavien II complication. On the PULS, 76.9% of patients did not present any lesion, 20.5% presented grade 1, and 2.6% grade 2 lesions. The renal ultrasonography and/or the computed tomography performed 3 to 6 months after the procedure demonstrated no hydronephrosis.
With respect to the reproducibility among hospitals, the result analysis for the intervention revealed no differences between the sites participating in the study (Table 4). Moreover, no differences were found between novel and experienced surgeons (Tables 1 and 3).
Measures calculated among patients not previously carrying a Double-J stent.
Median calculated among patients with a postoperative stent in each center.
χ2 = chi-square; λ = Symmetric Goodman and Kruskal Lambda; τ = Hospital independent Goodman and Kruskal Tau; K-W = chi-square Kruskal–Wallis; –/– = non employed data for methodological reasons.
Discussion
According to the AUA and the EAU guidelines, patients with ureteral stones under 6 mm, or even under 10 mm, can be offered conservative medical management provided there are no complication criteria. 10,11
Male patients were excluded from this study since the urethral length anatomy limits the instrumentation with the m-URS sheath, with its reduced length (22.5 cm) and caliber. The upper limit in women is L5-S1 level, in men being the sciatic spine and, in children, according to the age we can even reach the renal pelvis. Patients' age was higher than in the majority of the studies consulted. 12 The level of comorbidity and BMI were comparable to that of other series.
The surgical time in our study with m-URS (35.8 minutes) was shorter than that published by the CROES (Clinical Research Office of the Endourological Society) with “conventional” URS (42.2 minutes). This could be explained by a smaller mean surface area of the stones treated in our series (33.3 mm2 vs 66.6 mm2). 13
Except for those patients with ureteral stent before the intervention or in the cases in which safety guidewires were used per protocol, the use of a cystoscope was only required in two cases to perform the m-URS. Therefore, in these specific cases, m-URS could involve an increase of instrumentation.
Although guidelines recommend the use of safety guidewires, 10,11 some authors have previously compared the complications with and without their use. 14 In our study, each surgeon was free to use them or not. Guidewires could be inserted through the 4.85F sheath with fluoroscopic guidance or before the insertion of the sheath with a cystoscope. The meatus was accessed with no guidewire in 85% of all cases. One of the sites used the safety guidewire in 75% of its cases. In the rest of the sites, only two surgeons, in one procedure each, observed a need to use it during the treatment of the stone.
The reduced diameter of the sheath makes the distance between it and the ureteral wall greater. Therefore, the risk of damaging the meatus or the intramural ureter could be lower with m-URS.
The m-URS sheath only allows us to work with laser fibers between 230 and 270 μm (classic tip, not round), while “conventional” URS allows for the use of wider fibers. The existing studies are not conclusive regarding whether or not the diameter of the fiber affects the capacity to fragment the stone. 15,16 In any case, we consider its performance to be sufficient to treat the lithiasis in an acceptable period of time. In the study by Galán and colleagues, 17 the mean surface area of the stones treated was 33 mm2, which is similar to ours, with a longer surgical time, at 42 minutes. It should be noted that the majority of the sites participating in the study were experts in URS, but that this was their first contact with m-URS.
The use of the conventional ureteroscope was due to poor image quality in three out of four cases. All of them occurred in the same site. This leads us to believe that it could be due to an isolated failure of the site's m-URS equipment.
Although there were 15 impacted stones, the use of the “conventional” ureteroscope was only required to treat the stone in one case. The frequency of impacted stones in our series (38.5%) is higher than that published by the CROES (29.2%) for distal ureter lithiasis. 13 This is an independent factor increasing postoperative complications. 18
It is remarkable that starting treatment with m-URS did not impede the effective completion of the procedure in any case. Therefore, no patients required retreatment.
About the effectiveness of m-URS, the immediate success of the treatment was homogeneous among the different sites. One site considered that no patient could be declared stone free right at the time the procedure was finalized. In the rest of the hospitals, all of the patients were stone free 7 days after treatment. This result is in line with the results of conventional URS in the treatment of distal ureteral lithiasis. 19
To measure the safety of m-URS, the adaptation of the Clavien–Dindo classification was used 20 –22 for postoperative complications. A total of 97.4% of patients did not present any complications, and there was only one case of a grade 2 complication (postoperative fever that was resolved with endovenous antibiotic treatment). The study by Perez Castro and colleagues for the Endourological Society, in which 9681 patients were included, presented 3.8% intraoperative complications and 2.4% postoperative complications for distal ureter stones.
Moreover, we used the PULS, 23 to assess ureteral damage, caused by either the surgical intervention or by the ureteral stone itself. However, the series published to date differ regarding the characteristics of the stones treated; therefore, those results are not comparable to ours. 23 –25 It would be advisable to reach an agreement on the adoption of this scale in results reporting from different groups.
The postoperative ureteral stent independently affects patient quality of life. 26,27 The study conducted by the CROES for the treatment of ureteral lithiasis, showed that a Double-J ureteral stent was inserted in 54.7% of the cases 13 despite multiple studies certifying that a ureteral stent is not to be used systematically in uncomplicated ureteroscopies. 28 –30 Moreover, Caballero-Romeu and colleagues in a prospective–retrospective study described a reduction in the insertion of ureteral stents in patients treated with m-URS vs patients treated with URS using a 7.5F to 9.5F ureteroscope. 31 In our study, a ureteral stent was inserted in 17.1% of the cases. This highly favorable result may be due to the smaller size of the stone treated or to the reduced size of the m-URS sheath; in any case, further studies are needed to draw any conclusions in this regard.
During the study, surgeons were able to follow their standard practice and, at one site, the duration of the ureteral catheterization was always 14 days, regardless of the degree of ureteral lesion observed. Since some authors 23 establish that each degree of ureteral lesion requires a different duration of ureteral catheterization, this is not always possible due to the healthcare or administrative circumstances of each site.
No significant differences were found in the technical variables or in the results of the technique across the hospitals participating in the study; therefore, the result could suppose the homogeneity of the m-URS technique.
The primary limitations of the study were the reduced sample size, although the multicenter nature of the study reinforces the reproducibility data found. The nonuse of a standardized protocol may seem to be a limitation of this study, but in the authors' opinion, it shows that the technique is feasible regardless of the procedure used and its variations. Another limitation of the study might be the inability to determine the cost-effectiveness of the procedure. The sheath is a disposable device. Its cost is about 400 U.S. dollars. In any case reducing the ureteral damage could reduce the readmission rate, the rate of inpatient procedures, the need of secondary procedures, and/or the use of analgesics.
Conclusions
m-URS is an effective, safe, and reproducible technique that minimizes surgical aggression to the ureteral anatomy. Comparable results to “conventional” URS are obtained in the treatment of distal ureteral stones in women, although clinical trials comparing the two techniques are needed to assess any advantages or disadvantages. The reduction of the ureteral damage may reduce secondary procedures and increase the cost-effectiveness of the procedure.
Footnotes
Author Disclosure Statement
No competing financial interests exist.