
Abstract
Introduction:
The incidence of urolithiasis is increasing in the Western population. Significant advances in ureteroscopy and stone fragmentation energy sources have resulted in a paradigm shift in urolithiasis management. We aimed to assess the current state of urolithiasis management in Australia over the last 15 years using population-based data.
Methods:
Medicare Australia databases were accessed and Medicare rebate codes pertaining to ureteroscopy, extracorporeal shockwave lithotripsy (SWL), and percutaneous nephrolithotomy (PCNL) were extracted per state, year, and gender between 2001 and 2015. Population data were extracted from the Australian Bureau of Statistics website and provided the “population at risk” denominator to calculate incidence proportions.
Results:
From January 2001 to December 2015, 114,789 ureteroscopy or pyeloscopy procedures for stone extraction in adult patients were performed in Australia. During the same period, 48,209 SWL and 6956 PCNL procedures were performed. Ureteroscopy and pyeloscopy procedures have been increasing by an average of 9.3% year-on-year, population adjusted, while SWL has decreased by 3.5% and PCNL by 6.4% every year over the same period. In absolute terms, scope procedures have increased yearly by an average of 3.9 per 100,000 of population (confidence interval [95% CI]: 3.2, 4.5), while SWL has changed by −0.77 (95% CI: −0.88, −0.65) and PCNL by −0.16 (95% CI: −0.17, −0.14).
Conclusion:
Over the past 15 years in Australia, the total number of stone treatment procedures has increased significantly. Considerable increases in ureteroscopy were observed with relative and absolute reductions in SWL and PCNL. Regional variations in urolithiasis management strategies highlight the need for consensus on stone treatments within Australia.
Introduction
O
The introduction of flexible ureteroscopy and respective fragmentation energies has resulted in significant practice changes. Population-based studies from the United States and the United Kingdom have recently demonstrated a modification in stone treatment management techniques. 3,4 Similarly, in 2011, Lee and Bariol identified similar trends in the Australian population, reporting a movement toward increased use of less invasive techniques. 5 Despite this, precise regional variations in stone treatment practices have not been clearly established. 2,6 –10 Such information is critical due to the significant burden that stone disease provides to healthcare expenditures annually.
The aims of the current study are multiple. We first aimed to identify contemporary stone treatment trends in the Australian population. Furthermore, we aimed to identify locoregional variations in stone treatment strategies within Australia.
Methods
Data extraction
From January 2001 to December 2015, data regarding the total number of ureteroscopies, pyeloscopies, SWL, and PCNL were obtained from the Medicare Australia website. 11 The Medicare Benefit Schedule (MBS) code was identified for ureteroscopy (36806 and 36809), pyeloscopy (36654 and 36656), SWL (36546), and PCNL (36627, 36639, and 36645). Data were stratified by year, age, gender, and state. Chronologic data were extracted in calendar year format. We excluded surgeries performed on pediatric patients aged younger than 15 years. Ureteroscopy and pyeloscopy statistics was pooled for statistical analysis. Such data represent private practice remunerations. Public practice data are not captured by MBS-based data. MBS and respective definitions are summarized in Table 1.
MBS = Medicare Benefit Schedule; PCNL = percutaneous nephrolithotomy; SWL = extracorporeal shockwave lithotripsy.
Corresponding population data were extracted from the Australian Bureau of Statistics (ABS) from 2002 to 2014 12 and for 2015. 13 The population figures obtained were from the ABS estimates at June 30th of the corresponding year, in accordance with the Medicare data. Data pertaining to the number of practicing urologic surgeons were available for 2005, 2010, 14 and 2015. 15 During these time points at 2005, 2010, and 2015, there were 266, 324, and 408 registered urologists, respectively.
Statistical analysis
We calculated incidence proportions per 100,000 people using a denominator specific to the study population; for example, the incidence of SWL for Victorian males in 2004 was calculated as the total number of SWL procedures in 2004 for Victorian men, multiplied by 100,000 and divided by the estimated male population on June 30, 2004, in Victoria. By taking the population-adjusted incidences in 2001 as the reference and setting them to 100, we evaluated relative increases/declines in the rates of the procedures. To evaluate the growth or decline in a particular surgery, we used univariable linear regression. Data analysis was performed using Stata v.12.0 SE (College Station, TX).
Results
From January 2001 to December 2015, 50,239 pyeloscopy procedures for stone extraction in adult patients were performed in Australia. During the same period, 48,209 SWL and 6956 PCNL procedures were performed (Table 2). The SWL procedure was proportionally preferred for younger patients (30% vs 25%) while PCNL was favoured more in female patients (48% vs 41%) while PCNL was favoured more in female patients (8.5% vs 5.8%). State-based differences in the mix of treatments were observed. With SWL being popular in Victoria and Tasmania, pyeloscopic procedures overwhelmingly more common in Western Australia and PCNL relatively more common in South Australia and the territories. Pyeloscopy procedures have increased exponentially from 269 in 2001 to 8496 in 2015, while SWL and PCNL have been in relative decline to 60% and 39% of their 2001 incidences, respectively (Fig. 1).
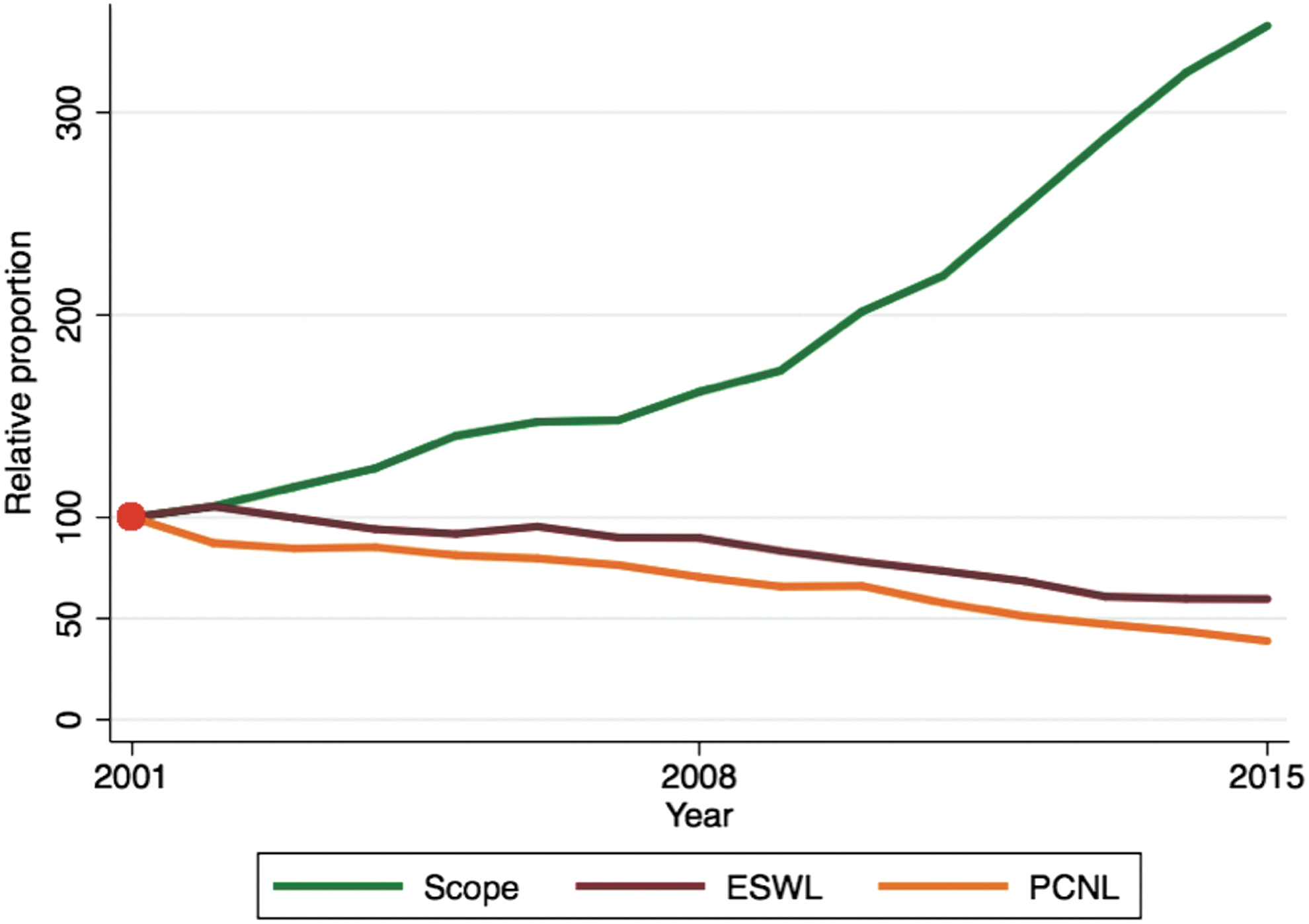
Relative population-adjusted incidence of stone clearing procedures. 2001 figure set as reference level.
The numbers in parentheses are the percentage split within the column and according to geographic location.
Over the 15 years, pyeloscopy procedures have been increasing by an average of 26% every year, population adjusted, while SWL has decreased by 3.6% and PCNL by 6.5% every year over the same period. In absolute terms, scope procedures have increased yearly by an average of 3.9 per 100,000 of population (confidence interval [95% CI]: 3.2, 4.5), while SWL has changed by −0.77 (95% CI: −0.88, −0.65) and PCNL by −0.16 (95% CI: −0.17, −0.14). The divergent incidences of stone elimination procedures were mirrored both for males and females and for those aged 15 to 65 years and older than 65 years (Figs. 2 and 3).
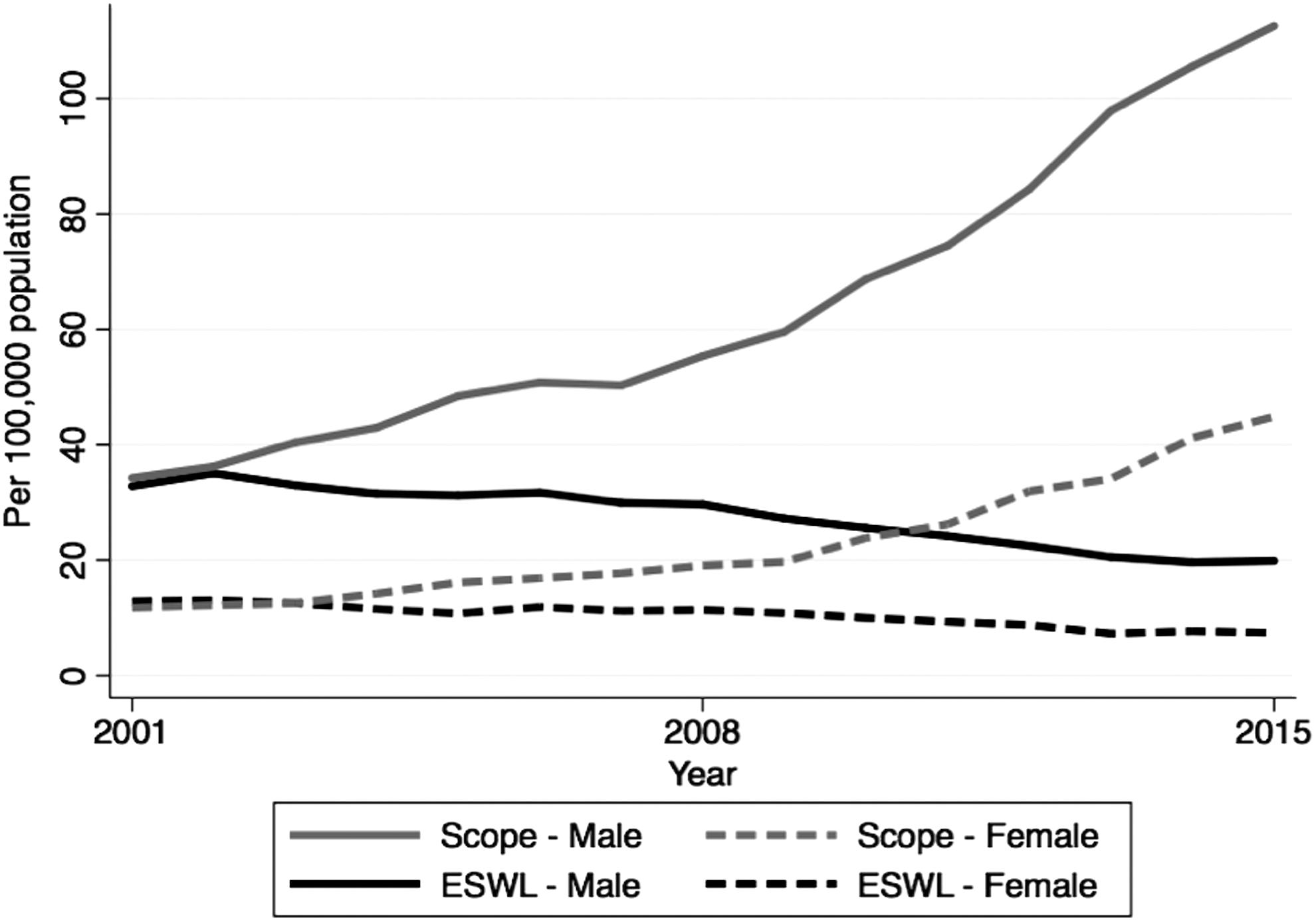
Scope and SWL procedures per 100,000 population, stratified by gender. SWL = extracorporeal shockwave lithotripsy.

Scope and SWL procedures per 100,000 population, stratified by age group.
State-based differences in the mix of therapies were observed (Fig. 4). In Victoria where SWL remains popular, the rapid uptake of pyeloscopy occurred in 2010, much later than other states, whereas in WA, the SWL procedure never achieved much favor. In 2015, in all states, pyeloscopy was the more prevalent procedure for renal stone clearance.
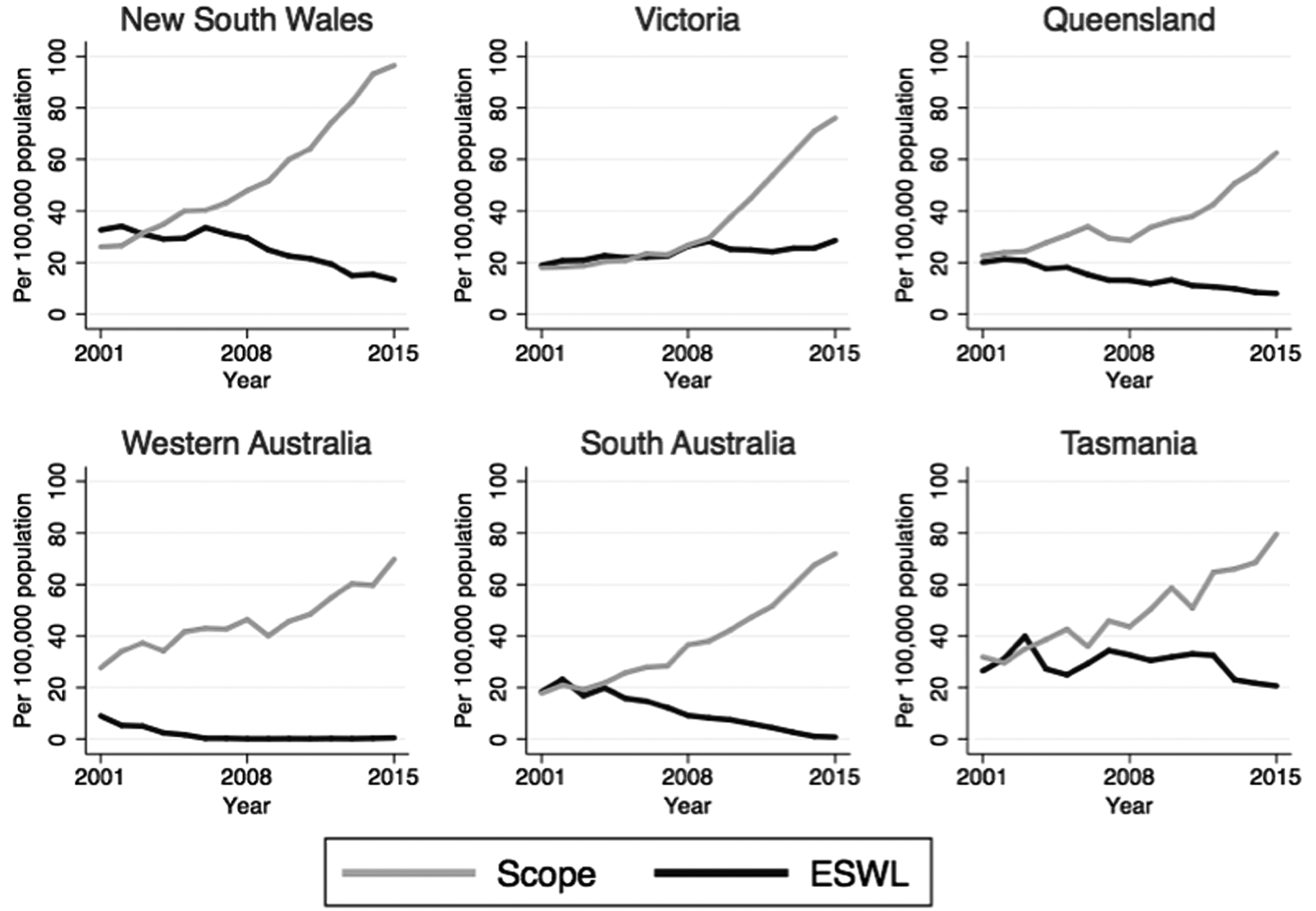
Scope and SWL procedures per 100,000 population, by state.
Discussion
Both the increasing incidence of urolithiasis and considerable advances in operative technology have resulted in significant changes in urolithiasis treatment over the past decades. The findings of the current study highlight the treatment trends in private practice stone management within Australia over the last 15 years. Pertinently, the findings from the current study identified increased volumes of retrograde renal surgery, declines in SWL and PCNL, and significant state-based discrepancies in practice patterns.
The current study emphasizes the rapid increase in private-practice operative MBS billings for stone treatments over the last 15 years. This may be attributed to an increase in stone prevalence and shifting treatment patterns. It has been demonstrated that stone prevalence continues to climb, 16 more than doubling in the United States over the last 30 years. 2,9 Similar trends in increasing stone treatments have been reported from the United Kingdom. 4 This may be related to the modern pervasiveness of stone risk factors such as a lithogenic diet, obesity, and metabolic syndrome, 3,17 as well to CT scanning becoming ever-more commonplace. 18,19 Accordingly, there has been an increased incidental detection of asymptomatic urolithiasis. Furthermore, increased MBS billings for stone treatments may be attributed to a lowering of the stone treatment threshold, as a result of the improved safety and efficacy of ureteroscopic interventions. Specifically, it may be assumed that there have been increased procedures for small asymptomatic upper tract calculi. 16,20
The current study identified the considerable uptake in endoscopic urolithiasis management with relative stagnation of SWL and PCNL. This finding has been previously reported in Australia, 5 New Zealand, 20 Brazil, 16 the United States, 3 United Kingdom, 21 and other nations. 22 The cause of this is likely multiple. Significant advances in endoscopic equipment have improved intrarenal accessibility and potential for lithotripsy. Specifically, newer ureteroscopes are narrower, more flexible, able to achieve greater deflection, and have considerably higher resolution. 23 In addition, newer ureteroscopes are able to accommodate more sophisticated lasers or baskets to facilitate stone fragmentation and extraction. 23 Furthermore, ureteroscopic equipment has become more readily available. 5,20 These factors have made ureteroscopy easier to learn and perform. Due to this increasing availability, training surgeons are now exposed to large volumes and thus achieve relatively high levels of competence before commencement of independent private practice. This may be evidenced, in part, by Matlaga et al. who demonstrated a greater use of ureteroscopy among early-career urologists. 24 Finally, the increased uptake in ureteroscopy and pyeloscopy may also be influenced by financial incentives. However, from the current data, no meaningful conclusions may be drawn regarding the possible impact of remuneration on stone treatment trends.
This change in practice in the management of urolithiasis is clearly reflected in the recommendations of the major urological authoritative bodies. Of these guidelines, the most widely recognized are published by the European Association of Urology (EAU) and the American Urological Association (AUA). To compare the recommendations of the EAU and AUA in 2016 to their own guidelines two decades ago is to witness great change in urolithiasis assessment and management. This is especially so for preferred interventions, which often contrast sharply with current practice. The EAU in 200125 did not recommend ureteroscopy as first-line management for calculi in the proximal ureter or any renal site. Second-line treatment for any ureteral calculi consisted of the now out-dated technique of performing ureteroscopy to push calculi proximally into the renal pelvis, followed by SWL. Similarly, the AUA in 1997 recommended SWL for all ureteral stones, with ureteroscopy being a viable alternative for distally located stones only. 26 In contrast, the latest urolithiasis recommendations by the same authoritative bodies advocate the use of ureteroscopy as first-line treatment for larger or distal ureteral stones. Currently, the AUA guides and supports the use of SWL for proximal ureteral stones. Regarding intrarenal calculi, the latest recommendations support SWL or ureteroscopy as first-line options for smaller intrarenal calculi. 27,28 The guidelines for larger intrarenal stones (>20 mm) remain unchanged, with PCNL recommended. 25,27
State-based discrepancies were identified regarding the treatment trends for urolithiasis. Specifically, the time at which divergence of ureteroscopy and SWL occurred differed significantly. New South Wales, Queensland, and South Australia experienced a rapid uptake of ureteroscopy earlier in the study period, occurring between 2002 and 2004. Conversely, divergence occurred in Victoria at a later time point, occurring after 2009. It is likely that the Victorian SWL use has been stable or increased during the study period, given that Victoria provides a centralized SWL service. Furthermore, Victoria is more densely populated, with SWL service more readily accessible to a greater proportion of the Victorian population. Such variation in practice may be attributed to the availability of ureteroscopic technologies, variation in calculi size and location, or surgeon preference. Nevertheless, limitations to the current data impair the ability to further assess such postulations. These variations in practice however, highlight the need for standardized treatment protocols within Australia to optimize patient outcomes.
There are several limitations to the current data. MBS billings only reliably capture private-practice data, and thus, the current data are not a reflection of public practice. Despite this, such data have been validated in other domains of medical practice, including melanoma excision. 29 Data pertaining to calculi size or location, cost, stone-free rates, time-of-procedure, and associated morbidity were not available for further analysis. Data pertaining to retreatment per patient and per stone were not available for analysis due to deficiencies in the Medicare-based data.
Conclusions
Over the past 15 years in Australia, the total number of stone treatment procedures has increased significantly. Considerable increases in ureteroscopy were observed with relative reductions in SWL and PCNL. Regional variations in urolithiasis management strategies highlight the need for consensus on stone treatments within Australia.
Footnotes
Acknowledgment
M.P. is supported by a research scholarship provided by the Royal Australasian College of Surgeons.
Author Disclosure Statement
No competing financial interests exist.