
Abstract
Purpose:
To evaluate the long-term outcomes and safety photoselective vaporization of the prostate (PVP).
Patients and Methods:
From April 2005 to December 2015, a total of 1154 patients with benign prostatic hyperplasia underwent PVP. The type of Green Light laser was an 80 W potassium-titanyl-phosphate laser and later a 120 W lithium triborate laser. Before and after surgery, the International Prostate Symptom Score (IPSS), maximum urinary flow rate (Qmax), post-voiding volume of residual urine (PVR), prostate-specific antigen (PSA) level, and prostate volume were assessed regularly. After surgery, events such as second PVP, transurethral incision, and permanent urethral catheterization were defined as retreatment.
Results:
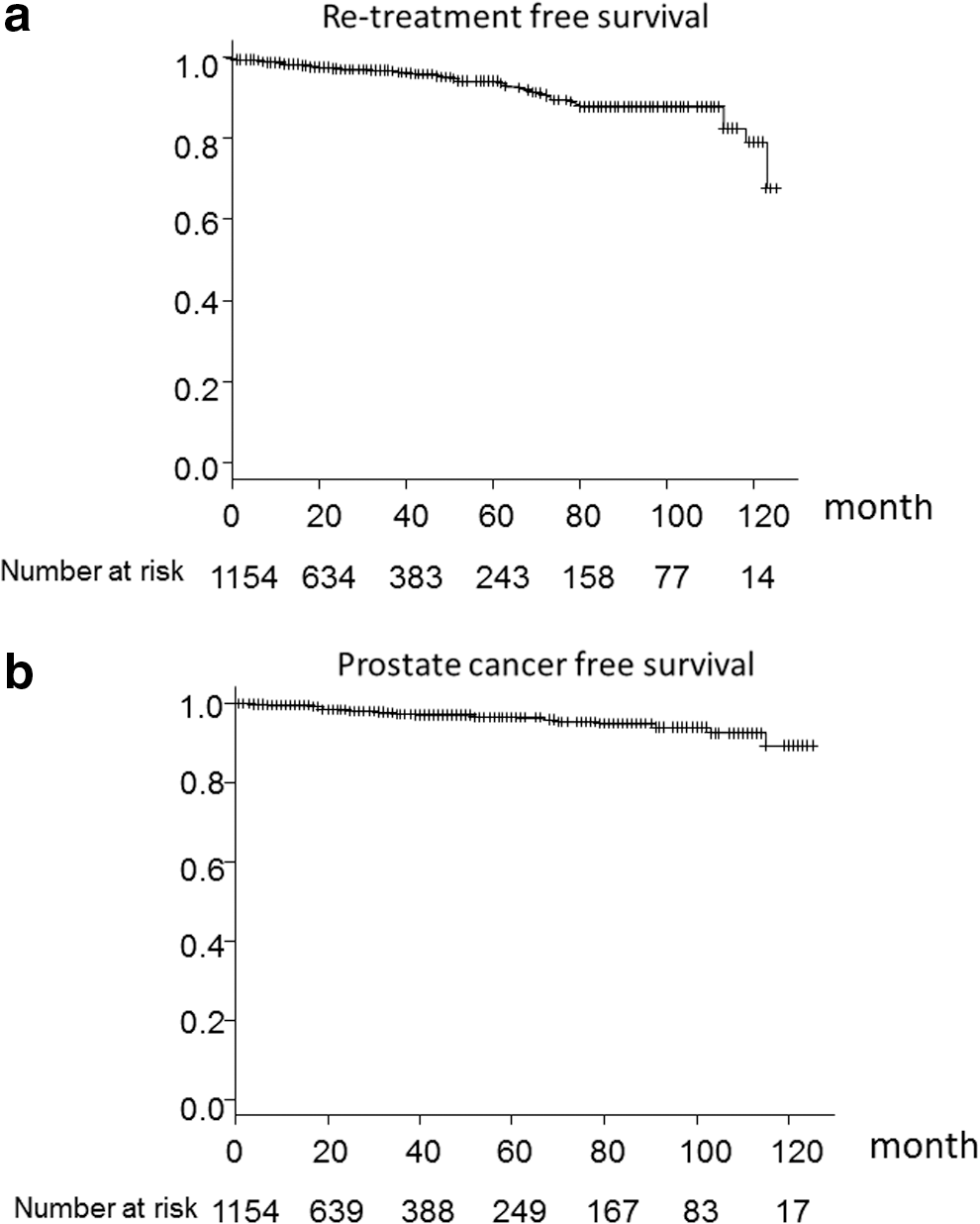
The mean and median periods of follow-up after PVP were 35.4 and 24.0 months, respectively. The maximum duration of follow-up was 125 months. Compared with before surgery, the IPSS, quality of life score, and PSA concentration improved significantly, even at 10 years after PVP; however, Qmax and PVR were not improved at 10 years. The retreatment-free survival rate was 93.9% at 5 years and 79.0% at 10 years. Prostate cancer was found in 27 cases after PVP, and all patients who were found to have prostate cancer remained alive. Prostate cancer-free survival after PVP was 96.7% at 5 years and 89.4% at 10 years.
Conclusion:
Our data suggest that the efficacy of PVP was maintained for 10 years; however, it may decrease after more than 10 years. PVP also did not promote the progression of or worsen the prognosis of prostate cancer.
Introduction
P
Another disadvantage of vaporization procedures such as PVP is the absence of tissue for histopathologic examination, which carries the risk of missing a diagnosis of prostate cancer. 9 The incidence of prostate cancer after PVP has been rarely reported. 7 It is also feared that patients who receive PVP may miss the chance for diagnosis or treatment of prostate cancer. Thus, we assessed the incidence and mortality rate of prostate cancer after PVP, for the purpose of determining whether PVP may worsen the mortality rate of prostate cancer by accelerating or masking prostate cancer.
In this study, we retrospectively show the long-term outcomes and safety of PVP at our institution.
Patients and Methods
From April 2005 to December 2015, a total of 1154 patients with obstruction from BPH underwent PVP. Before surgery, the International Prostate Symptom Score (IPSS), quality of life (QOL) score, uroflowmetry (UFM), post-voiding volume of residual urine (PVR), and prostate volume (PV) by transrectal ultrasound were assessed. For prostate cancer screening, a digital rectal examination, transrectal ultrasound, and measurement of serum prostate-specific antigen (PSA) were performed. If the concentration of PSA was ≥4.0 ng/mL, prostate biopsies were carried out routinely. We also performed cystoscopy before PVP for the purpose of bladder cancer screening and confirmation of prostatic shape.
Operative procedure
PVP was carried out under general or lumbar anesthesia. A 22.5F Olympus PVP continuous flow laser cystoscope was used. Initially, in 2005, we used a KTP laser with an 80 W GreenLight PV surgical system (American Medical System) for 557 cases; since April 2011, we have used an LBO laser with a 120 W GreenLight HPS surgical system (American Medical System) for 598 cases. During surgery, a distance of about 1 mm was maintained between the adenoma and the laser fiber, and a milk white color on the surface of the vaporized tissue by continuous bubble formation was used as an indication of good vaporization. 8 Vaporization was performed until the prostatic urethra was sufficiently opened. Perioperative data, such as operation time, total laser energy, laser time, laser type, catheterization time after PVP, and hospital stay after PVP, were recorded. The serum hemoglobin and sodium concentrations were also measured before and after surgery.
Follow-up
The IPSS, QOL score, maximum urinary flow rate (Qmax), and PVR were evaluated at 1, 3, 6, and 12 months and then every 1 year after PVP. The PSA concentration was evaluated at 3 months and every 1 year after PVP. PV was measured at 3 months and 1 year after PVP. Postsurgical events, such as second PVP, transurethral incision of the urethra for urethral stricture, or permanent urethral catheterization, were defined as retreatment, as was hematuria requiring hospitalization. During follow-up, if retreatment was required or prostate cancer was identified, the time period after the operation was recorded.
Statistical analyses
Comparisons of function before and after surgery were analyzed with nonparametric tests. Survival rates of retreatment-free or prostate cancer-free survival were estimated by Kaplan–Meier analysis. Risk factors for retreatment after PVP were analyzed by Cox regression models. All statistical analyses were performed with R statistical programming software v 3.1.1 (R Project for Statistical Computing).
Results
A total of 1154 patients with BPH were enrolled in this study. Patient characteristics are listed in Table 1. Perioperative results are summarized in Table 2. The mean decrease in hemoglobin was 0.7 mg/dL, and no patient required a blood transfusion. The mean and median periods of follow-up were 35.4 and 24.0 months, respectively. The longest period of follow-up was 125 months. The total number of patients at 5 and 10 years after surgery, including both those who participated in follow-up and those who were lost to follow-up, was 540 and 85 patients, respectively. Thus, the actual percentage of patients at follow-up was 37.6% at 5 years and 21.2% at 10 years.
Values are mean (SD, range) unless otherwise specified.
IPSS = International Prostate Symptom Score; PSA = prostate-specific antigen; PV = prostate volume; PVR = post-voiding volume of residual urine; Qmax = maximum urinary flow rate; QOL = quality of life; SD = standard deviation.
Values are mean (SD, range) unless otherwise specified.
KTP = potassium-titanyl-phosphate; LBO = lithium triborate.
At less than 10 years after surgery, the IPSS, QOL score, Qmax, PVR, and PSA level were improved compared with before surgery (Fig. 1). The reductions in PV were 54.8% at 3 months and 51.2% at 12 months after PVP. The reductions in PSA were 44.4% at 3 months after PVP and 35.1% at 12 months after PVP. At 10 years after PVP, the IPSS, QOL score, and PSA were significantly improved compared with before surgery; however, PVR and Qmax were not. Hematuria occurred in 37 (3.2%) cases, urethral strictures were recognized in 4 (0.3%) cases, and retreatment was performed in 54 (4.7%) cases. The retreatment-free survival rate was 93.9% at 5 years and 79.0% at 10 years (Fig. 2a). Laser energy more than 250 kJ, preoperative IPSS ≥20, operation time more than 75 minutes, and PV more than 80 mL were significant risk factors for retreatment after PVP (Table 3). Prostate cancer was found in 27 cases during follow-up. Prostate cancer-free survival was 96.7% at 5 years and 89.4% at 10 years (Fig. 2b). All patients were found to have localized cancer. Mean follow-up was 40 months since prostate cancer diagnosis, and all patients were alive within the follow-up period.

Changes in subjective and objective outcomes with PVP procedure:
Bold type indicates statistically significant values.
CI = confidence interval; HR = hazard ratio; PVP = photoselective vaporization of the prostate.
Discussion
PVP has been compared with TUR-P in several randomized controlled trials, and it has demonstrated comparable clinical outcomes with reduced morbidity, such as less blood loss and shorter hospitalization and catheterization times. 3,4,7 Another significant advantage of PVP is the ability to perform surgery in patients receiving anticoagulant therapy and in patients with poor performance status. 10 Because of these advantages, PVP has gained widespread acceptance as an alternative option requiring preoperative patient selection. 9
Although many studies have shown the usefulness of PVP for the treatment of obstruction from BPH, most reports are of short-term observations. 6,7 In contrast, other procedures for BPH, such as TUR-P or holmium laser enucleation of the prostate (HoLEP), have data regarding long-term outcomes. 11,12 Thus, there is concern regarding the long-term durability of outcomes after PVP.
We observed long-term outcomes of PVP, with a maximum duration of follow-up of 125 months. Efficacy outcomes as much as 10 years after PVP, including IPSS, QOL score, Qmax, and PVR, were improved compared with those before surgery. Catheterization time and length of hospital stay after PVP were 19 hours and 2.0 days, respectively. Hematuria occurred in 37 (3.2%) cases, urethral strictures were recognized in 4 (0.3%) cases, and retreatment was performed in 54 (4.7%) cases. Our data indicated that PVP is useful and safe, similar to other reports. 5,7
However, at 10 years after PVP, PVR and Qmax had worsened and were less significantly different from before PVP. These data indicate that the objective efficacy of PVP decreases at long-term periods after PVP, especially after more than 10 years. It is suspected that the reason for the worsening is age-related detrusor dysfunction. 13 Because we did not measure detrusor function with a pressure flow study, we could not determine the age-related dysfunction of the detrusor in our patients. However, Beltrame and colleagues used a pressure flow study to reveal a significant decrease in voiding efficiency (p = 0.029), voided volume (p < 0.001), Qave (p = 0.008), and Qmax (p = 0.048) with increasing age. 13 Another reason for the worsening could have been reobstruction of a residual nodule resulting from insufficient resection. 6
We first used a KTP laser, which is less powerful than an LBO laser. It is thought that appropriate resection of the prostate is reflected by a PSA reduction of more than 50%. 9 Our data showed that the PSA reduction was 35.1% at 12 months after PVP. Elmansy and colleagues reported that the PSA reduction achieved with vaporization with an 80 W KTP laser was 31%. 12 Currently, crystal lasers (GreenLight XPS) have shown superior outcomes for short-term periods. 14,15 In a new XPS study, the reduction at 12 months after PVP was 61% for PVs <80 mL and 50% for PVs ≥80 mL. 14 These comparisons indicated that the XPS laser has efficacy superior to the KTP laser in PVP. It is hoped that PVP using the XPS laser will maintain the effect for longer term periods, especially over 10 years. Thus, we must await the longer-term outcomes of PVP using the XPS laser.
We also assessed functional outcomes based on the retreatment rate. Retreatment-free survival was 93.9% at 5 years, 87.7% at 8 years, and 79.0% at 10 years. Hai reported a 5-year retreatment rate of 8.9% after PVP. 6 In contrast, Madersbacher and colleagues reported that the rate of secondary endourologic procedures within 8 years was 14.7% after TUR-P. 11 We showed that laser energy more than 250 kJ, preoperative IPSS ≥20, operation time more than 75 minutes, and PV more than 80 mL were significant risk factors for retreatment after PVP. Pfitzenmaier and colleagues reported a higher frequency of retreatment after vaporization for patients with prostates of ≥80 mL compared with prostates of <80 mL. 16 Because large prostates that require a long time for vaporization tend to have more remaining tissue, retreatment may be necessary. It is suggested that these risky cases should undergo long-term follow-up to monitor for future recurrence.
The vaporization technique also has been developed for the purpose of effective resection. Stone and colleagues reported vapoenucleation by the XPS laser on large-volume glands. 17 If vapoenucleation techniques reduce the residual nodule, especially in large glands, the retreatment rate may decrease. In contrast, our data showed that the long-term limitations at 10 years were objective outcomes, such as Qmax or PVR, while subjective outcomes, such as QOL score or IPSS, were maintained at 10 years. If patients are satisfied with their urinary symptoms at 10 years after PVP, it may be thought that the efficacy is maintained.
We also recorded the prostate cancer incidence of patients who received PVP. It is thought that long-term follow-up enables the performance of these surveys. It may be suspected that the loss of tissue for pathologic examination by vaporization of prostate tissue masks prostate cancer and delays the cancer diagnosis. It has been noted that the possibility of a delayed cancer diagnosis and progression of prostate cancer are weak points of PVP. 18 Ruszat and colleagues indicated that six patients were found to have localized prostate cancer after 500 procedures. 2 Our data showed that 27 patients were found to have localized prostate cancer after PVP. All of these patients were alive within the follow-up period. Thus, PVP does not promote the progression of prostate cancer or worsen the prognosis of prostate cancer. If patients are screened for prostate cancer by PSA measurements before and after PVP, the loss of tissue for analysis may not be a weakness of PVP.
Our study has some limitations. Although the longest duration of follow-up was 125 months, many of the cases were lost to follow-up for several reasons. In addition, the statistical evaluation of the outcomes used nonparametric methods. It is hoped that a strict prospective study that can be analyzed by parametric methods will be carried out. Second, we sequentially changed the type of laser used for PVP, from an 80 W KTP to a 120 W LBO, so the long-term outcomes were of patients for which only the KTP laser was used. Now, in addition to the 120 W LBO laser, the 180 W LBO laser is used. It is hoped that the long-term outcomes with these new laser types will be reported.
Conclusion
Long-term follow-up revealed that the outcomes of IPSS, QOL score, and PSA were significantly improved, even at 10 years after PVP; however, Qmax and PVR were no longer improved at 10 years. PVP also does not promote the progression or worsen the prognosis of prostate cancer. If patients are screened for prostate cancer by PSA measurements before and after PVP, the loss of tissue for analysis may not be a weakness of PVP.
Footnotes
Author Disclosure Statement
No competing financial interests exist.