
Abstract
Purpose:
To evaluate changes in renal function and overall survival in elderly vs nonelderly patients undergoing radical nephrectomy (RN) for renal masses.
Patients and Methods:
We reviewed available records of 392 patients undergoing RN from 2008 through 2013. Patients were divided into elderly, defined as ≥70 years old (n = 110), or nonelderly (n = 282) at the time of nephrectomy. The groups were compared for perioperative characteristics, renal functional outcomes, and overall survival. Standard Student's t-tests were used for continuous variables and Fischer's exact tests for categorical comparisons. Kaplan–Meier estimate models for survival were compared using log-rank tests.
Results:
Elderly patients were more likely to have comorbidities. Preoperative estimated glomerular filtration rate (GFR) of elderly patients was significantly lower (65.6 vs 77.9 mL/minute/1.73 m2, p = 0.0002), as was GFR at discharge (47.7 vs 57.2 mL/minute/1.73 m2, p = 0.001) and at maximum follow-up (46.8 vs 57.4 mL/minute/1.73 m2, p = 0.001). Of the patients with GFR >60 before surgery, de novo CKD stage III progression (defined as GFR <60) was detected in 74% of elderly and 53% nonelderly (odds ratio 2.47; 95% confidence interval 1.25–4.88; p = 0.01). Overall survival was not statistically different. When stratified for elderly and preoperative GFR <60, overall survival curves were not statistical different (log-rank test, p = 0.23).
Conclusions:
Elderly patients who undergo RN have worse renal functional outcomes. Following nephrectomy, these patients are at higher risk of CKD progression than nonelderly patients. However, there does not appear to be a difference in overall survival between cohorts, even when stratified for preoperative GFR <60. These findings should be considered during preoperative decision-making.
Introduction
K
Tumor size, patient comorbidities, and anticipated life expectancy are important factors in determining treatment approach in elderly patients with renal masses. Given that over 80% of elderly oncology patients have at least one significant comorbidity requiring treatment, the risk of surgery must be carefully weighed in the setting of the aging patient. 7
CKD is defined as a decrease in estimated glomerular filtration rate (GFR) ≤90 mL/minute/1.73 m2. Furthermore, CKD stage 3 (defined as GFR <60 mL/minute/1.73 m2) is an important comorbidity linked to increased incidence of cardiovascular events, hospitalization, and death. 8 In fact, a robust analysis of patients ≥75 years old undergoing active surveillance, nephron-sparing intervention, or RN by Lane and colleagues suggests that pretreatment GFR is predictive of cardiovascular death and exceeds that of cancer-specific mortality rate in each group. 5 Given the limited number of studies examining the rapidly growing elderly patient population, we sought to evaluate the patient characteristics, changes in renal function, and overall survival of elderly patients undergoing RN.
Patients and Methods
We performed a review of a prospectively maintained institutional review board-approved database of 392 patients who underwent RN from 2008 through 2013. Surgeries were performed by a variety of providers and both open and minimally invasive approaches were included. Patients were divided into elderly, defined as ≥70 years old (n = 110), or nonelderly (n = 282) at the time of nephrectomy. Designating age 70 as elderly was a compromise between the U.S. Census definition of elderly as ≥65 years old, the increasingly aging population, and previous studies that have used 70 and 75 years as a cutoff. 5,9,10
We captured baseline patient characteristics and medical comorbidities such as obesity, hypertension (HTN), diabetes mellitus (DM), coronary artery disease (CAD), chronic obstructive pulmonary disease (COPD), and hyperlipidemia (HLD). Preoperative renal function was recorded as serum creatinine and estimated GFR based on the Modification of Diet in Renal Disease study (MDRD) and recorded as mL/minute/1.73 m2. All patients underwent preoperative cross-sectional computed tomography to evaluate size of the mass and location. Pathologic analysis provided tumor stage.
Renal function characteristics were recorded postoperatively as they were available. The most recent follow-up serum creatinine and GFR were recorded. We evaluated the risk of de novo stage III CKD (defined as development of GFR <60 mL/minute/1.73 m2). The percent change in GFR from baseline to maximum follow-up GFR was also calculated. To avoid confounding GFR data, pre- and postoperative patients on dialysis were excluded from the analysis.
Postoperative complications were characterized according to the Clavien–Dindo system with complications ≥ grade 3 considered major. 11 Overall survival data were obtained through chart review and confirmation using the Social Security Death Index.
The data from each group are reported as mean with standard deviation and compared using Student's t-tests for continuous variables and Fischer's exact tests for categorical comparisons. Kaplan–Meier estimate models for survival were compared using log-rank tests. A calculated p-value of <0.05 was considered significant. Statistical analysis and graphing were performed using GraphPad Prism software, version 6.0. There was no financial support for this work and the authors have no disclosures.
Results
A total of 392 patients with available data underwent RN for renal masses between 2008 and 2013. One hundred ten (28%) patients were ≥70 years of age (range 70–91 years), and 282 patients (72%) were <70 years old (range 18–69 years). Elderly patients were more likely to have higher American Society of Anesthesiologists (ASA) scores (p = 0.0026). Younger patients had significantly higher average BMI (30.3 vs 27.9, p = 0.001) and higher rates of obesity based on BMI ≥30 (47% vs 35%, p = 0.03). Elderly patients were also more likely to have HTN (82% vs 70%, p = 0.02) and HLD (55% vs 39%, p = 0.004). However, the cohorts were similar in terms of rates of DM and COPD. Elderly patients had CAD more frequently, but the difference was not statistically significant. There was no difference in open or minimally invasive surgical approach between the groups (Table 1).
ASA = American Society of Anesthesiologists; CAD = coronary artery disease; COPD = chronic obstructive pulmonary disease; DM = diabetes mellitus; GFR = glomerular filtration rate; HLD = hyperlipidemia; HTN = hypertension.
Baseline tumor characteristics were similar between groups in terms of tumor laterality, size, and clinical stage. There was no difference between groups in terms of number of patients on preoperative or postoperative dialysis, and these patients were excluded from the final analysis. Mean preoperative GFR based on MDRD equation was significantly lower in elderly patients (65.6 vs 77.9 mL/minute/1.73 m2, p = 0.0002), Table 1.
Elderly patients were noted to have significantly diminished mean GFR at discharge (47.7 vs 57.2 mL/minute/1.73 m2, p = 0.001). Median time for maximum follow-up renal function testing was 447 days (range 1–1903 days). Absolute postoperative GFR reflected significantly diminished renal function in elderly patients and appeared quite similar to discharge results (46.8 vs 57.4 mL/minute/1.73 m2, p = 0.001). However, the mean percent decrease in absolute GFR was similar between elderly and nonelderly patients (−25.5 vs −24.5%, p = 0.79).
Of the patients with preoperative GFR ≥60, de novo CKD stage III progression (defined as GFR <60) was detected in 74% of elderly patients vs 53% nonelderly (odds ratio 2.47; 95% confidence interval 1.25–4.88; p = 0.01), Table 2. Twenty-three percent of elderly patients with preoperative CKD stage III progressed to higher stage of CKD, which was not statically different from the 29% of younger patients with preoperative CKD stage III who progressed (p = 0.63). Of note, there was no significant difference in the number of patients progressing to CKD stage IV or V (defined as GFR ≤30 and ≤15, respectively). A total of 4 patients had progressive renal failure requiring hemodialysis (HD) following surgery. One patient had bilateral malignancies and subsequent bilateral nephrectomies, two patients required acute HD related to multisystem organ failure before their death (both had metastatic disease), and one patient progressed to chronic CKD stage V requiring long-term HD who is currently alive.
CKD = chronic kidney disease; MDRD = Modification of Diet in Renal Disease study.
Rates of any complication were similar between groups. However, when stratified by degree of complication (major complication ≥ Clavien grade 3), the elderly patients had a nonsignificant trend to have more complications (8.2% vs 3.6%, p = 0.06). Major complications were mostly limited to T3 or T4 tumors requiring large aggressive resections and postoperative resuscitation. They included acute blood loss anemia requiring reexploration, hypoxic respiratory failure requiring intubation, non-ST elevation myocardial infarction, unstable atrial fibrillation requiring ICU stay, acute or chronic renal failure requiring temporary dialysis, and stroke. The rate of minor complications was similar between elderly and the younger cohort (12.7% vs 13.8%, p = 0.37, respectively).
Overall survival curves did not define median survival and tended to favor the younger cohort, but this was not statistically significant according to log-rank testing (p = 0.133). When stratified for elderly and preoperative GFR <60, overall survival curves were not statistical different between groups (log-rank test for trend, p = 0.23), Figure 1.
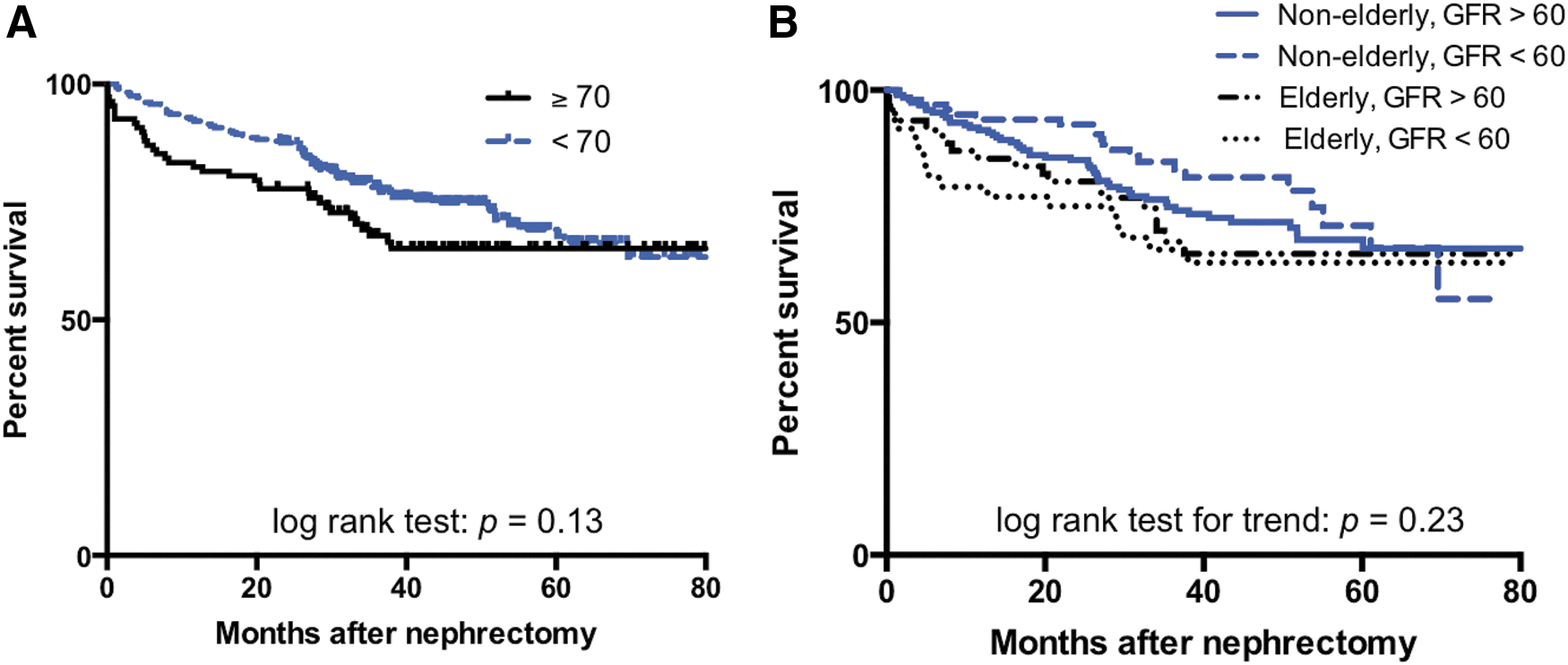
Kaplan–Meier estimates of overall survival stratified for age
Discussion
Although metastatic RCC is a lethal disease, localized RCC is a much more common diagnosis, and elderly patients may be more likely to succumb to competing causes of mortality. 12 Early detection of RCC has increased over the past two decades, but cancer-specific mortality rate has been minimally changed. 13,14 Thus, aggressive treatment of localized renal masses with RN should be thoughtfully considered, particularly in the elderly. Renal function is well recognized as an important factor influencing cancer survivorship following treatment for localized RCC. 15 Furthermore, RN predisposes patients to CKD more than nephron-sparing PN. 16 Even when controlling for diabetes and HTN, CKD is associated with increased risk of hospitalization, cardiovascular events, and death, 8 and this has been confirmed following development of chronic renal insufficiency after RN. 17 In this analysis, we observed significantly diminished GFR and increased risk of de novo CKD for elderly RN patients compared with the younger cohort. However, there was no difference in overall survival. Our data add to a growing cohort of literature highlighting that although RN decreases GFR, it may have minimal impact in survival for elderly patients.
Comparative patient demographics, preoperative comorbidities, and tumor characteristics between cohorts were similar to our previous evaluation of elderly patients undergoing PN. 10 Elderly RN patients had a higher prevalence of HTN, HLD, along with higher ASA scores, and lower preoperative GFR. The prevalence of COPD and CAD favored elderly patients, but was not significantly different. There was no difference in tumor stage for elderly and young. These results suggest consistency among the elderly population treated at our institution.
Despite the increased number of comorbidities noted in the elderly cohort, there was no difference in minor complications between groups. There was a nonsignificant trend for elderly patients to experience more major complications. This trend is expected given the known link between frailty, advanced age, and surgical complications, particularly for advanced kidney cancer. 18 –20
RN predisposes patients to the development of de novo CKD, which carries increased risk of cardiovascular events and death. 16,21 Pre-existing CKD (GFR <60 mL/minute/1.73 m2) was more frequently observed and mean GFR was significantly lower in the elderly population (66 vs 78 mL/minute/1.73 m, p = 0.0002). Elderly patients did appear to have a significantly decreased GFR at discharge and more frequent de novo CKD at maximum follow-up. However, the percent change in GFR at maximum follow-up time was similar between groups. This is likely explained by the lower preoperative GFR observed in elderly patients. Indeed, elderly patients with reduced GFR have limited reserve and are at higher risk of dropping GFR below the threshold of 60 mL/minute/1.73 m2. Regardless of age, there was an over 50% chance of developing stage III CKD with RN, which is consistent with previous publications. 5,16
As expected, we did note a trend of diminished overall survival in elderly patients, but median survival was not defined in our analysis. This may speak to the limited number of patients included in the study and limited follow-up. Considering the association of CKD with unfavorable outcomes and the increased risk of competing mortality rate for elderly patients, we evaluated overall survival stratified for age and preoperative CKD stage III. 5,8 Our analysis revealed no significant difference in overall survival of patients stratified by age and preoperative GFR <60. There was a trend for diminished survival for elderly patients with GFR <60, but this was not significantly different from the other curves, Figure 1.
Given the observed increased rate of de novo CKD in elderly patients following nephrectomy, the survival results are somewhat surprising. We hypothesized that diminished preoperative GFR and de novo CKD in elderly patients would translate to significant survival changes. However, this does not necessarily appear to be true in our analysis. The results are consistent with previous work by Lane and colleagues, demonstrating that surgically induced CKD had lower risk of progressive renal decline and impact on survival compared with medically induced CKD. 22 However, this study did not specifically examine elderly patients. 22 Taken together, the data suggest that GFR changes associated with RN in the elderly may not impact overall survival. These findings parallel another study by Lane and colleagues suggesting RN in elderly patients does significantly decrease GFR, but surgical treatment of RCC in the elderly may not prolong overall survival. 5
Considering this information is important in the context of selecting partial vs RN in the elderly population, EORTC 30904 is the only randomized control trial comparing PN vs RN and it reported that PN was associated with better renal function outcomes, but overall survival favored RN. 23 Thus, we must consider the question: Does GFR preservation in elderly patients translate to survival?
Demirjian and colleagues performed a notable comparative analysis of surgically induced CKD vs medical CKD in 2014. The study suggests that the relative risk of progressive renal dysfunction is low for patients undergoing nephrectomy who have a contralateral kidney, no preexisting CKD, and GFR >40 mL/minute/1.73 m2 following RN. 24 However, this study does not stratify for age. In the context of our analysis in which preexisting CKD III was not associated with decreased overall survival, the combined studies suggest that perhaps RN is an equivocal choice to PN for elderly patients in terms of survival. This may be particularly true when tumor size and location are unfavorable for PN. In other words, perhaps the comorbidities and reduced life expectancy of elderly patients may not require optimal GFR preservation and the survival impact of surgically induced CKD may be minimal.
This study is not without limitations. The data were evaluated in a retrospective manner and subject to the inherent biases related to this approach. There are intrinsic inadequacies of MDRD equation as an estimate of GFR, but it has been shown to be reasonably accurate in the elderly. 25 As a tertiary referral center, long-term follow-up is often referred back to local physicians. Longer term follow-up would better delineate differences between the groups. Regardless, we feel that this analysis adds to the growing collection of literature evaluating the importance of renal function consideration in the elderly when performing extirpative renal surgery. Further work is required to evaluate the optimal treatment options for renal masses in patients with limited life expectancy.
Conclusions
Compared with younger patients, elderly undergoing RN have diminished preoperative and postoperative renal function. The elderly are at risk for development of CKD stage III following RN. However, this does not translate to diminished survival for elderly patients, even when stratified for preoperative GFR <60 mL/minute/1.73 m2. Taken together, these data should be considered when counseling elderly patients to optimal therapy for renal masses.
Footnotes
Author Disclosure Statement
No competing financial interests exist.