
Abstract
Introduction:
The efficiency of holmium laser lithotripsy for urolithiasis depends upon several factors, including laser pulse energy and frequency and stone composition and retropulsion. This study investigates the complex interplay between these factors and quantifies lithotripsy efficiency using different laser settings in a benchtop kidney and ureter model.
Materials and Methods:
In vitro caliceal and ex vivo porcine ureteral models were constructed. Calcium oxalate monohydrate stones were fragmented using a 200-μm laser fiber. In the caliceal model, stone fragmentation and vaporization rates at settings of 0.6 J/5 Hz, 0.2 J/15 Hz, and 0.2 J/50 Hz were compared. In the ureteral model, fragmentation time, retropulsion rate, fragmentation rate, and fragmented stone weight were compared at settings of 0.6 J/5 Hz and 0.2 J/15 Hz. Retropulsive forces generated at 0.6 J/5 Hz, 0.2 J/15 Hz, and 0.2 J/50 Hz settings were compared. Analysis was performed using Student's t-test and one-way ANOVA.
Results:
In the caliceal model, the 0.6 J/5 Hz setting fragmented and vaporized stones at a higher rate than the 0.2 J/15 Hz setting (0.072 vs. 0.049 mg/s; p < 0.001). However, when the 0.2 J energy setting was combined with the 50 Hz frequency, the fragmentation rate (0.069 mg/s) was similar to the fragmentation rate at 0.6 J/5 Hz (0.072 mg/s; p = 0.677). In the ureteral model, the 0.6 J/5 Hz setting produced higher fragmentation rates (0.089 vs. 0.049 mg/s; p < 0.001), but resulted in significantly lower fragmented stone weight overall (16.815 vs. 25.485 mg; p = 0.009) due to higher retropulsion rates (0.732 vs. 0.213 mm/s; p < 0.001). Retropulsive forces decreased significantly when pulse energy decreased from 0.6 to 0.2 J (0.907 vs. 0.223 N; p < 0.001). Frequency did not affect retropulsive force at 15 and 50 Hz settings (0.223 vs. 0.288 N; p = 0.509).
Conclusions:
Laser lithotripsy of calcium oxalate monohydrate stones in the ureter should be performed using the low-energy, moderate-frequency dusting setting to minimize retropulsion and maximize efficiency. In the renal calix, the low-energy high-frequency setting performed similarly to the high-energy low-frequency setting.
Introduction
T
Prior in vitro trials studied the interplay between these factors and various laser generator settings, including pulse energy, frequency, and pulse duration. 2 –4 In general, these studies were carried out using stone phantoms or mixed composition stones and in vitro models. As a result, the influence of conventional and stone dusting settings upon the disintegration efficiency of pure calcium oxalate monohydrate (COM) stones has not been well characterized.
Our study was designed to recreate the multifactorial interaction surgeon's encounter during laser lithotripsy. We studied the efficiency of holmium laser lithotripsy upon calcium oxalate monohydrate urinary calculi in multiple surgical environments, using different holmium laser generator settings. Additionally, we measured the retropulsive force transmitted to stones at various laser generator settings.
Materials and Methods
Calculi
Four-millimeter pure COM urinary calculi were separated by weight and diameter into 20 matched groups of three in the caliceal model and into 20 pairs in the ureteral model. Before use, all stones were dried for 24 hours and weighed on an AT460 DeltaRange electronic balance (Mettler Toledo, Columbus, OH). All stones were prehydrated for 24 hours before laser lithotripsy. Following fragmentation, stones were again dried for 24 hours and weighed. Lithotripsy was performed by the same surgeon.
Caliceal model
A caliceal model was constructed by mounting two metal sieves with 0.92- and 0.25-mm pores onto a hollow polymer tube with an inner diameter of 10 mm. The sieve with larger pores was mounted superiorly and supported the calculus during lithotripsy, while the sieve with smaller pores was mounted beneath to entrap residual stone fragments. A 5-mm polyethylene tube was attached to the polymer apparatus to mimic the infundibulum inserting into the renal calix (Fig. 1). The model was immersed in saline during treatments.
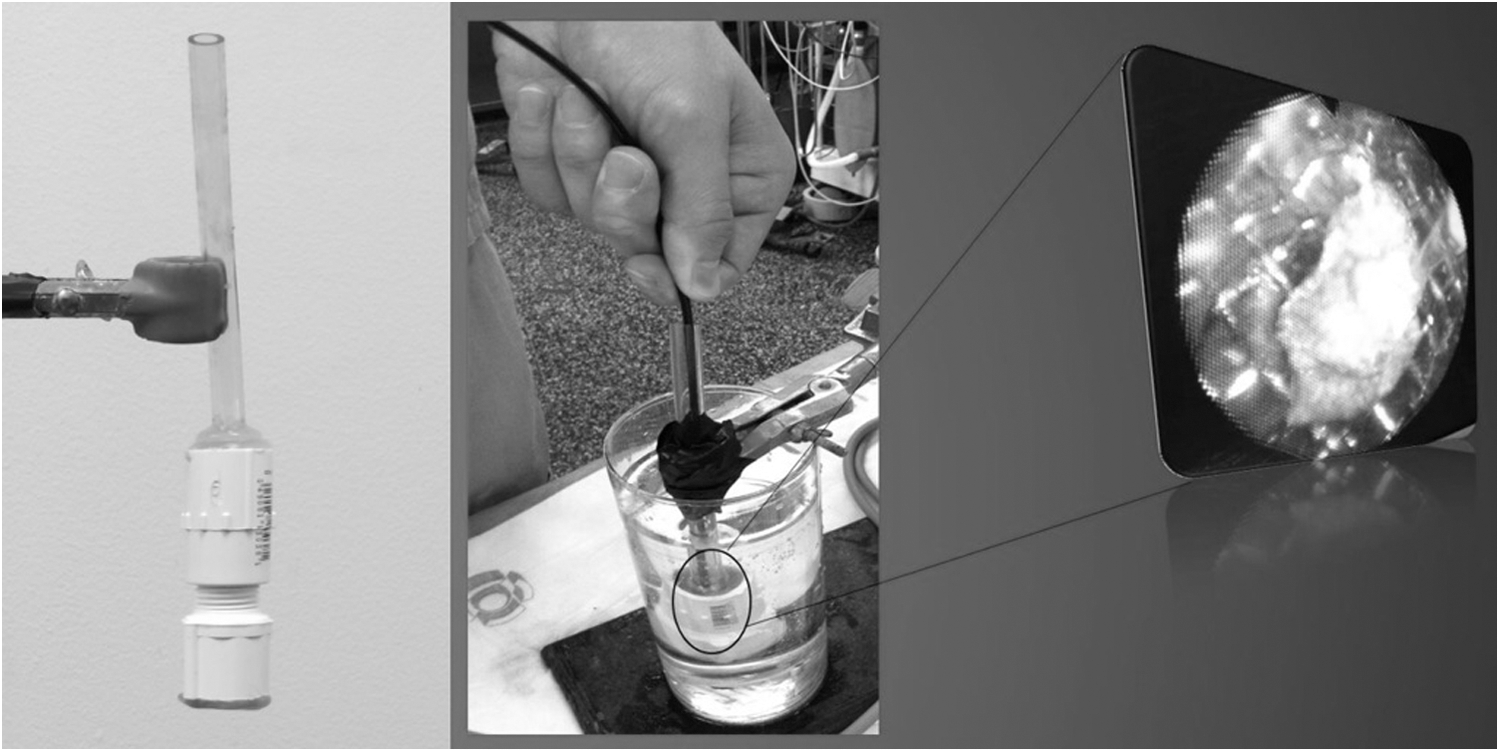
An in vitro model of the renal calix and pelvis utilized during the caliceal portion of the study (left), including the endoscopic view (right).
The Lumenis VersaPulse® PowerSuite™ 100-watt laser (Lumenis, Yokneam, Israel) was used in all trials. Laser lithotripsy was performed using a SlimLine 200 reusable laser fiber (Lumenis, Yokneam, Israel) deployed through an 8.8F Viper flexible ureteroscope (Richard Wolf, Vernon Hills, IL). Ceramic scissors were used to cleave a 4-cm section of laser fiber between each trial.
Stones were randomly assigned to lithotripsy at settings of 0.6 J/5 Hz, 0.2 J/15 Hz, and 0.2 J/50 Hz. Lithotripsy duration was timed until all fragments passed through the 0.92-mm sieve. Residual fragments on the lower 0.25-mm sieve were dried and weighed. The laser fiber was cleaved after each group of three stones. Vaporization was defined as fragments <0.25 mm in diameter and was calculated by subtracting the residual weight left on the 0.25-mm sieve from the original weight. Rates of fragmentation and vaporization were calculated by dividing fragmented and vaporized weights by treatment times, respectively (Fig. 2).
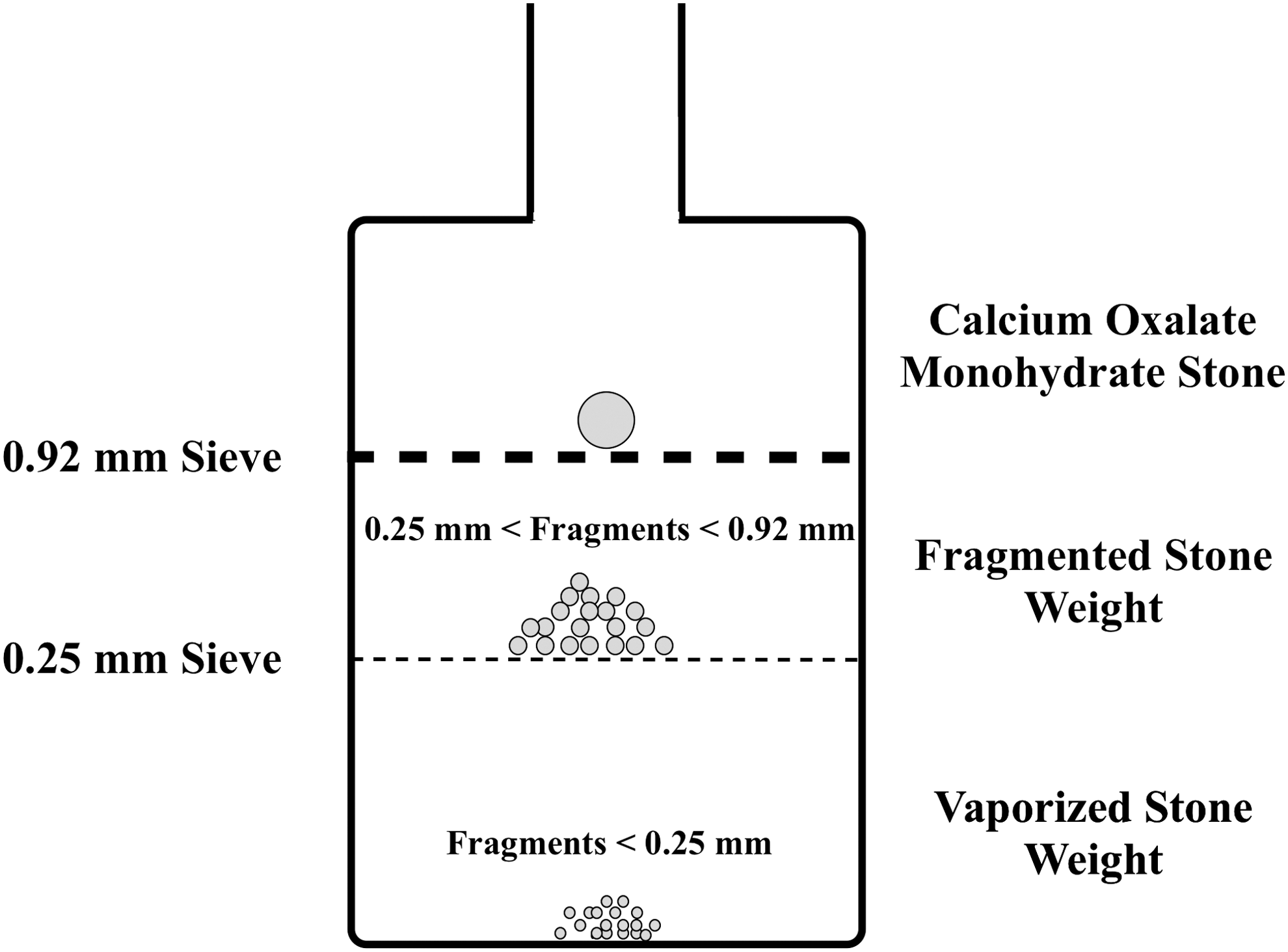
Diagram of renal calix and pelvis model demonstrating sieves and stone fragments.
Ureteral model
Porcine ureters were obtained from a local abattoir. Differences in lengths were accounted for by treating paired stones sequentially in the same ureter and by comparing rate of migration per time. On one end, ureters were sutured using 4–0 poliglecaprone 25 (Ethicon Endo-Surgery, Somerville, NJ) to shortened, single-use urethral catheters (Finnegan Medical, Little Rock, AR) to facilitate introduction of calculi into the ureter before lithotripsy. The cut ends of the catheter were subsequently fixed to a stationary platform. Size 0 silk suture (Ethicon Endo-Surgery, Somerville, NJ) was used to close the opposite end of the ureter, which was also fixed during lithotripsy (Fig. 3). The entire apparatus was submerged in saline.

Porcine ureter model closed at one end with 0 silk suture and anastomosed to a shortened catheter at the other; ureteroscope has been inserted through the catheter. Fiber optic light denotes location of ureteroscope tip within ureter. Arrows are included to identify the item designated by the label.
Each calculus was inserted into the shortened urethral catheter, advanced through the sutured anastomosis, and precisely positioned at the distal end of the ureter using the flexible ureteroscope. In the same manner as the kidney model, lithotripsy was performed sequentially on each of the paired calculi at generator settings of 0.6 J/5 Hz and 0.2 J/15 Hz in random order. Lithotripsy was performed for 10 minutes or until the calculus reached the proximal end of the ureter as this signified stone retropulsion into the renal pelvis.
Stone fragments were collected, strained through a sieve with 0.92-mm pores, dried, and weighed. Distance between initial position and position at termination of lithotripsy was recorded as the distance of retropulsion. Similar to the caliceal trials, the laser fiber was cleaved after each randomized pair of calculi. Twenty pairs of calculi were fragmented in eleven porcine ureters. Weight fragmented and fragmentation rate were calculated as in the caliceal model. Rate of retropulsion was calculated by dividing retropulsion distance by duration of lithotripsy.
Force of retropulsion
A glass tube with 1 cm diameter was mounted into a polymer basin. A small opening was drilled on the side of the container in line with the lumen of the glass tube to accommodate an extension rod attached to a Series 5 digital force gauge transducer (Mark-10, Copiague, NY). A flathead detector was placed flush with the glass tube opening (Fig. 4) and the container was filled with saline. Stones of relatively higher mass (5.5 mm, 65 mg) were selected to produce higher peak retropulsive forces and highlight any potential differences between laser settings.
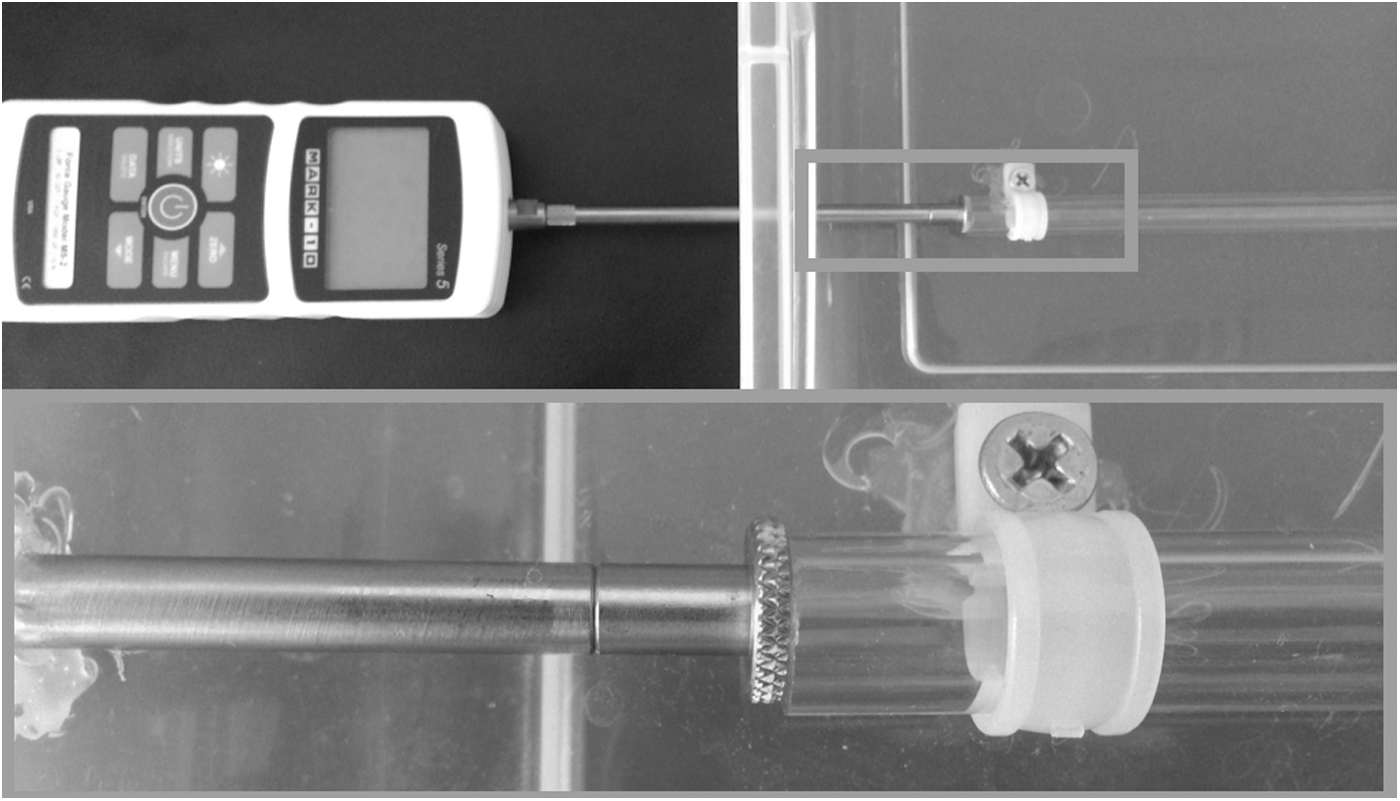
Retropulsive force model showing digital force gauge (top) and close-up of flathead detector (bottom).
Twenty calculi were lasered per trial at settings of 0.6 J/5 Hz, 0.2 J/15 Hz, and 0.2 J/50 Hz for 5 seconds while in direct contact with the force transducer's detector. Peak retropulsive forces generated during each lithotripsy session were recorded.
Statistical analysis
Statistical analysis was carried out using Student's t-test and one-way ANOVA for continuous variables in the IBM SPSS system (Version 22, Armonk, North Castle, NY) with p < 0.05 characterized as significant.
Results
Caliceal model
In the caliceal model, there was no difference between the three groups of calculi in pretreatment weight (31.6, 31.6, and 31.9 mg; p = 0.992) or pretreatment diameter (4.405, 4.325, and 4.409 mm; p = 0.532). Fragmentation rate was significantly higher at laser settings of 0.6 J/5 Hz (0.072 mg/s) and 0.2 J/50 Hz (0.069 mg/s) when compared with the 0.2 J/15 Hz (0.049 mg/s) setting (p < 0.001 for both comparisons). Fragmentation rates associated with the 0.6 J/5 Hz and 0.2 J/50 Hz were comparable (p = 0.677). Vaporization rates followed a similar trend, the 0.2 J/15 Hz setting generated significantly slower vaporization than both the conventional and the high-frequency dusting settings (p < 0.001 for both comparisons). The conventional and high-frequency dusting settings were similar (p = 0.138) (Table 1).
Bold values indicate p < 0.05.
Ureteral model
Pretreatment weight (36.9 and 36.2 mg; p = 0.863) and diameter (4.395 and 4.405 mm; p = 0.956) were similar for each pair of ureteral calculi. In the 0.6 J/5 Hz group, 100% of the calculi were retropulsed to the end of the ureter after a mean lithotripsy time of 189 seconds. Mean retropulsion rate was 0.732 mm/s. In the 0.2 J/15 Hz group, only 60% of the COM calculi had been retropulsed to the end of the ureter after 10 minutes of laser lithotripsy, contributing to a longer mean lithotripsy time of 510 seconds (p < 0.001) and a lower mean retropulsion rate of 0.213 mm/s (p < 0.001). Due to the longer treatment time afforded by the slower retropulsion, the 0.2 J/15 Hz setting fragmented a significantly higher stone weight (25.5 vs. 16.8 mg; p = 0.009), although at a slower rate (0.049 vs. 0.089 mg/s, p < 0.001) than the 0.6 J/5 Hz setting (Table 2).
Force of retropulsion
The mean peak retropulsive force generated by the 0.6 J/5 Hz setting was significantly higher than that generated by either of the lower pulse energy settings (p < 0.001 for both comparisons). Additionally, retropulsive forces generated by the 0.2 J/15 Hz setting and the 0.2 J/50 Hz setting were comparable (p = 0.509) (Table 3).
Bold values indicate p < 0.05.
Discussion
The holmium laser is a pulsed solid-state laser that operates at a wavelength close to the peak absorption of water (2120 nm vs. 1940 nm), thus making it safe and highly effective for lithotripsy of all types of calculi within the urinary tract. 5,6 Unlike earlier generation pulsed dye and switch Q lasers that primarily produced photomechanical fragmentation, 7 the holmium laser delivers emission pulses of longer duration predominantly resulting in photothermal fragmentation. 2,8,9 Photomechanical fragmentation is accomplished by introducing plasma bubbles that create shockwaves as they collapse, while photothermal fragmentation is accomplished by conversion of light into heat that causes the stone to melt as well as crack due to the rapidly expanding vapor within the stone. 5,7,10
Thus, due to less reliance on the highly retropulsive photomechanical forces for fragmentation, the holmium laser minimizes stone retropulsion and improves lithotripsy efficiency. 11 Furthermore, holmium laser lithotripsy yields smaller stone fragments compared with pulsed laser, electrohydraulic lithotripter, or pneumatic devices, thus reducing the need to basket stone fragments upon completion of lithotripsy. 12
The effects of pulse energy, pulse frequency, and retropulsion on lithotripsy efficiency have been previously investigated with in vitro models and stone phantoms or mixed composition stones. These studies have shown that as the pulse energy of the laser increases, more photons are delivered for stone ablation, thus increasing stone fragmentation. 2,3,13 However, retropulsion also increases due to the higher forces delivered, 14 thereby decreasing fragmentation efficiency. 15 Furthermore, lithotripsy at higher pulse energy settings produces larger fragment sizes, 3,13 which may require basket removal upon completion of lithotripsy or may make targeting these smaller fragments more difficult as they bounce around with each laser pulse.
Other studies have increased the frequency to 40 Hz while holding the pulse energy constant and demonstrated that this does not result in higher retropulsion. 2 Our study demonstrated that increasing the frequency to 50 Hz does not significantly increase retropulsion. Unlike previously published studies, which used calculi of various compositions, our study is unique, in that all calculi were pure calcium oxalate monohydrate stones, thereby limiting variations of stone composition upon fragmentation rates within the experiment.
The surgical environment of laser lithotripsy can be dichotomized into the intrarenal collecting system and the ureter, each with unique properties that affect laser lithotripsy efficiency. Our study is the first to investigate this efficiency using surgical settings with common ureteroscopic surgical instruments, uniform human urinary stones, and models that closely approximate the renal calix and the ureter. Thus, this study integrates the physical properties of the holmium laser, the chemical properties of human stones, and the biological properties of the urinary tract to provide a more accurate depiction of lithotripsy efficiency. Understanding the optimal settings for laser lithotripsy will help endourologists achieve higher stone-free rates with minimal retropulsion and less operative time.
In our renal caliceal study, we used a model similar to that previously described by Finley and colleagues. 15 The 0.92-mm sieve mimicked the renal papilla that provides the backboard against which lithotripsy is commonly performed. All stones were fragmented into pieces less than 0.92 mm to ensure passage through the ureter after completion of treatment. 16
In this model, retropulsion is not a factor as the stones are treated within the closed confines of the calix. For the ureteral model, the farm pig ureter was selected based on previous studies demonstrating its close resemblance to human ureter histology and diameter 17 and its validity as an ex vivo model to investigate ureteroscopic properties. 18 In the ureteral trials, each pair of stones was fragmented using standard (0.6 J/5 Hz) and stone dusting (0.2 J/15 Hz) settings within the same ureter. A previous study controlled for total energy used 2 ; however, in our study, the time of lithotripsy was controlled instead, as this is the factor of utmost concern to urologists.
Several findings of previous in vitro experiments were confirmed. In agreement with previously published literature, we determined that increasing the pulse energy while holding the power constant increased stone fragmentation and vaporization rates. 2,3,13,19 The dusting trials using 0.2 J/50 Hz in the caliceal model also demonstrated that the decrease in fragmentation rate with lower pulse energy can be overcome by increasing the pulse rate. Similar results were obtained in the study by Sea and colleagues that used a 0.2 J/40 Hz setting. 2
In the ureteral model, retropulsion was increased by increasing pulse energy, as was previously shown using stone phantoms and mixed composition stones. 2,11 Over a 12 cm distance, this reduces the potential fragmentation time by more than 5 minutes. Our in vitro model was designed to precisely quantify these retropulsive forces. As was previously shown using a secondary force measuring pendulum model, we demonstrated that the highest forces of retropulsion occurred with the highest pulse energy. 2,4 The current study demonstrated the effect that dusting settings have upon stone migration. Other factors may also affect stone migration. Kronenberg and Traxer have shown that the larger caliber laser fibers increase stone retropulsion. 20 Subsequently, the effects upon stone migration would only be increased with larger laser fiber diameters.
In contrast to previous studies that separately analyzed fragmentation and retropulsion rates, our porcine ureteral trials allowed comparison of total stone fragmentation weights and incorporated both fragmentation and retropulsion rates associated with various lithotripsy settings. Although fragmenting at a slower rate, the dusting setting was able to achieve a higher fragmented weight due to the lower retropulsive forces and longer lithotripsy time. Because of the lower retropulsion rate, the dusting setting allowed on average 5.4 minutes of additional lithotripsy time for ureteral stones.
The current study has potential limitations. Only one type of stone (COM) was tested; however, COM stones are common and our clinical experience has demonstrated that stone migration is most problematic when treating hard COM calculi. Additionally, we did not test energy settings above 0.6 J because previous studies have shown increased 200-μm laser fiber tip damage at levels higher than 0.6 J. 20 In addition, the laser fiber was cleaved before a set of three trials with different laser settings in the renal caliceal model or before a pair of trials in the ureteral model, with the order of laser settings picked at random to balance any possible discrepancy in power output due to fiber tip damage. 21
Another limitation of our study was the use of nonvascularized porcine ureters, which are smaller in caliber than human ureters. For this reason, 4-mm stones, which could be placed into the ureter, were used for these trials. Furthermore, lithotripsy trials in the ureteral model were stopped short when the stone reached the opposite end of the ureter. Although seemingly inflating stone fragmentation time for the stone dusting setting, this protocol accurately reflects the concern for retropulsion of the ureteral calculus into the kidney, with the potential need for a longer operative time to exchange surgical instruments, perform renoscopy to find the stone, and reposition the stone to a more favorable location before restarting lithotripsy. In addition, when semirigid ureteroscopy is being employed, migration of the stone into the kidney may require conversion from a semirigid to a flexible ureteroscope.
The 0.2 J/50 Hz setting was not included in the ureteral trials as lithotripsy with this setting produced the unfavorable endoscopic snowstorm appearance 13 and ureteral damage to our model. It is not known if this is just a limitation of the nonvascularized porcine ureter or if the injury to the ureter resulted from an interaction between the model and the laser settings employed during high-frequency dusting. Finally, all trials were performed using one laser device and a 200-μm laser fiber. Future studies, using laser fibers of increasing caliber and different laser generators could further elaborate upon various factors influencing stone migration.
Conclusions
This study demonstrates that laser lithotripsy of calcium oxalate monohydrate stones in the ureter was most efficient at the 0.2 J/15 Hz setting to minimize retropulsion and maximize stone fragmentation. In the renal calix, the low-energy high-frequency setting performed similarly to the high-energy low-frequency setting. Clinical trials should be performed to confirm these results.
Footnotes
Acknowledgment
The authors would like to thank Udochukwu Oyoyo for his assistance and expertise with statistical analysis.
Author Disclosure Statement
This study was funded by an unrestricted grant from Lumenis Surgical.