
Abstract
Over the past 25 years, the average life expectancy for men has increased almost 4 years, and the age of prostate cancer detection has decreased an average of 10 years with diagnosis increasingly made at early-stage disease where curative therapy is possible. These changing trends in the age and extent of malignancy at diagnosis have revealed limitations in conventional curative therapies for prostate cancer, including a significant risk of aggressive cancer recurrence, and the risk of long-term genitourinary morbidity and its detrimental impact on patient's quality of life (QOL). Greater awareness of the shortcomings in radical prostatectomy, external radiotherapy, and brachytherapy has prompted the search for alternative curative therapies that offer comparable rates of cancer control and less treatment-related morbidity to better preserve QOL. High-intensity focused ultrasound (HIFU) possesses characteristics that make it an attractive curative therapy option. HIFU is a noninvasive approach that uses precisely delivered ultrasound energy to achieve tumor cell necrosis without radiation or surgical excision. In current urologic oncology, HIFU is used clinically in the treatment of prostate cancer and is under experimental investigation for therapeutic use in multiple malignancies. Clinical research on HIFU therapy for localized prostate cancer began in the 1990s, and there have now been ∼65,000 prostate cancer patients treated with HIFU, predominantly with the Ablatherm (EDAP TMS, Lyon, France) device. Neoadjuvant transurethral resection of the prostate has been combined with HIFU since 2000 to reduce prostate size, facilitate tissue destruction, and to minimize side effects. Advances in imaging technologies are expected to further improve the already superior efficacy and morbidity outcomes, and ongoing investigation of HIFU as a focal therapy in salvage and palliative indications is serving to expand the role of HIFU as a highly versatile noninvasive therapy for prostate cancer.
The Clinical History of High-Intensity Focused Ultrasound
C
HIFU Mechanisms and Technology
Mechanism of action of HIFU
The first reported use of HIFU in local tissue destruction was made in 1944 by Lynn and Putman. 4 The use of high-energy parabolic-focused ultrasound results in the mechanical alteration and changes in the biologic structure of targeted cells (Fig. 1). 5 During the application of focused ultrasound, two different physical mechanisms account for its treatment effect: thermal and mechanical.
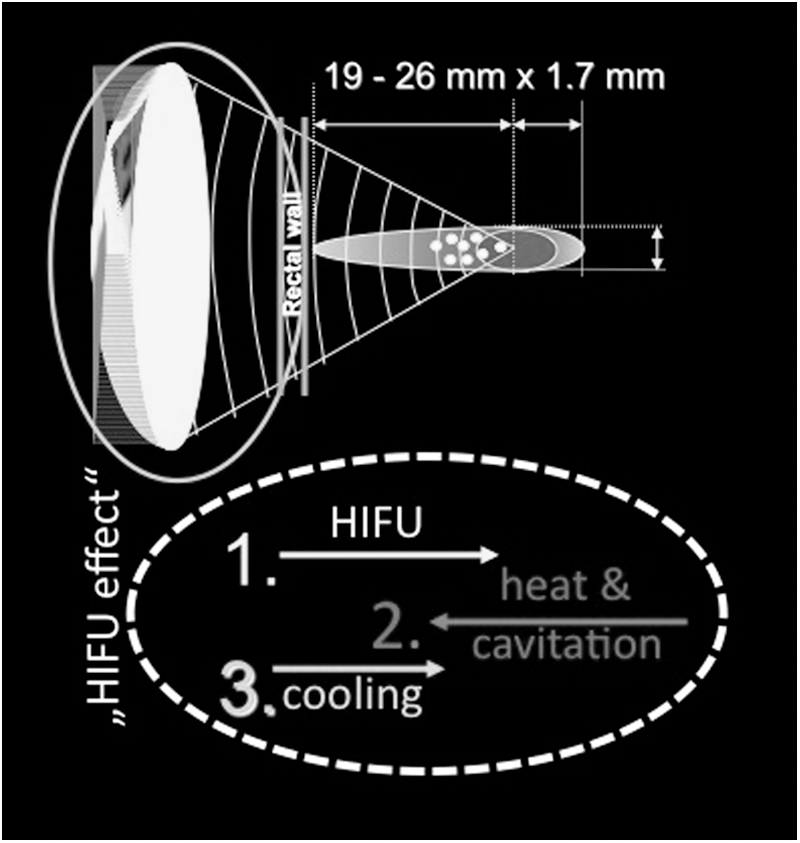
Physical principle of focused energy application. HIFU = high-intensity focused ultrasound.
Thermal
The ultrasound energy produced by HIFU is absorbed by the targeted tissue and converted into heat. The extent of temperature increase in the tissue depends on the absorption coefficient of the tissue, and the size, shape, and temperature sensitivity of the heated area. 5 Biologic changes caused by the heating depend on the temperature level and duration of exposure. A “thermal dose,” which exceeds a certain threshold, causes tissue coagulation and leads to irreversible tissue damage through coagulative necrosis. 6 The focused ultrasound waves of HIFU are capable of inducing sharp increases in temperature (around 70°C–100°C/160°F–210°F) in a few seconds. During the clinical use of HIFU, the tissue-sensitive adjacent structures such as the rectum, external sphincter, and the neurovascular bundles are spared from destruction due to the steep temperature gradient between the focal tissue and surrounding region. 6,7
Mechanical
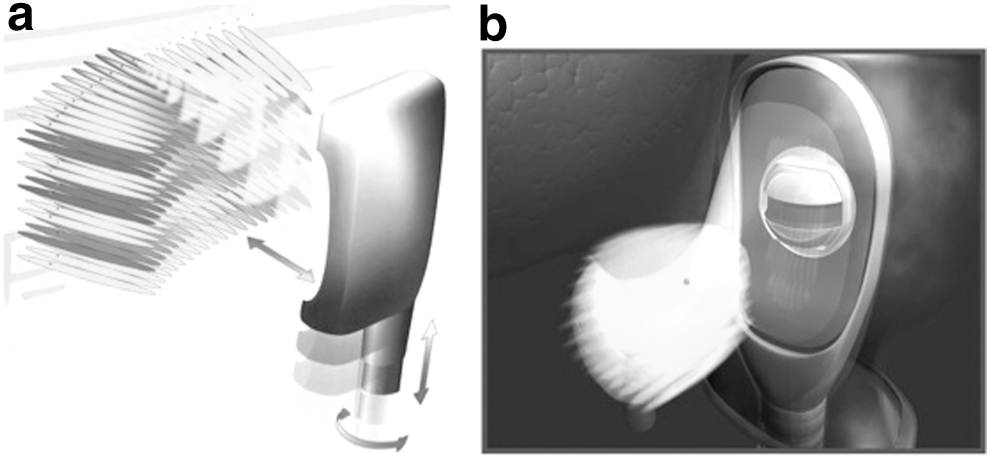
The mechanical effects of HIFU are induced by the effects of negative pressure of the ultrasound wave on the targeted tissue. 5 The negative pressure causes bubbles to form inside the targeted cells, which increase in size to the point at which resonance is achieved. High pressure of 20,000 to 30,000 bars develops when these bubbles suddenly collapse, causing damage to nearby cells. 8 The primary single lesions are small (1.7 × 19–26 mm) and produce reproducible volumes of sharply demarcated ablation. 4 The small volume of tissue destroyed by a single burst of ultrasound is termed the elementary or primary lesion. To create larger lesions, several elementary lesions are made side by side by adding multiple lesion targets to the algorithm (Fig. 2a, b) and either mechanically moving the transducer or by electronically positioning the focal point if a phased array is available. 6,9 –12
Experimental identification of clinical parameters
In vitro, in vivo, and computer simulation studies were conducted to identify and refine the ultrasound parameters required for the clinical treatment of prostatic disease. The destruction of tumors with HIFU in these studies provided the evidence that cancerous tissues can be destroyed by HIFU without inducing metastases, 13 and that prostatic tissue can effectively be targeted through transrectal delivery of HIFU. 14,15
Indications for HIFU Therapy of Prostate Cancer
The most widespread use of HIFU, and initially the only indication for its use, has been in patients with localized prostate cancer (T1–2N0M0; Gleason sum ≤6) who are not candidates for surgery because of age, general health status, a prohibiting comorbidity, or a preference not to undergo a radical prostatectomy (RPE). 5 However, with the accumulation of clinical experience and expansion of research protocols, these indications have broadened to include partial therapy in unilateral low-volume, low grade tumors (T1–2aNx/0M0; prostate-specific antigen [PSA] ≤20 ng/mL); salvage therapy in recurrent prostate cancer following RPE, radiation therapy, or hormone ablation (all TNx/0M0; all GS/PSA) 16 ; advanced prostate cancer as an additional neoadjuvant debulking process (T3–4Nx/0M0; all GS/PSA) 17 ; and in castration-resistant prostate cancer (CRPCa).
The diagnosis of prostate cancer is based on the histopathologic examination of biopsies in cases of suspicious PSA findings, digital rectal examination, magnetic resonance imaging, transrectal ultrasound (TRUS), or unexpected findings in resected tissue after open adenomectomy, holmium, or transurethral resection. 18
Combining TURP and HIFU
The use of neoadjuvant TURP with HIFU became routine practice in 2000 as a means to reduce post-HIFU urethral sloughing and obstruction, and offers several other advantages over HIFU alone. The combined procedure of TURP before HIFU in patients with localized prostate cancer allows the instant removal of any reflecting or deviating calcifications of the transitional zone that would prevent HIFU treatment, as well as abscesses, intravesical middle lobes, and large (>30 cc) adenomas. 5 The generation of a cavity and its subsequent compression by the rectal balloon increases the accessibility of the HIFU waves to the remaining gland (Fig. 3), fixes the residual prostate behind the symphysis, avoids movement artifacts, and allows the complete treatment of the peripheral zone in a single HIFU session. The penetration depth of the Ablatherm Integrated Imaging device is maximum 26 mm. Without a TURP, a total gland ablation of a larger gland (>30 cc) is not possible. TURP decreases the size of each prostate gland to ∼25 mL to eliminate size restriction with HIFU. 1,19 The increase of invasiveness by neoadjuvant TUR is compensated clearly by the beneficial effect in regard to higher efficacy and lower side effects; furthermore, it expanded the indication range for HIFU. 18,19

Compression and retropubic fixation of transurethrally resected prostate. TURP = transurethral resection of the prostate.
Efficacy of HIFU as Primary Therapy
Efficacy in localized disease
Similar to efficacy studies with external beam radiotherapy (EBRT), brachytherapy, and cryoablation, biochemical markers and biopsy findings have been used as indicators of long-term cancer control with HIFU. To date, there is no universal consensus on the definition of biochemical failure in patients treated with HIFU. 5 With ongoing refinements in execution and outcome measurement, the efficacy of HIFU in locally confined prostate cancer is now comparable to those of radiotherapy and RPE, which according to the CaPSURE database are characterized by failure rates of 63% at a mean of 38 months post-treatment and 30% at a mean of 34 months post-treatment, respectively 20 (Tables 1 and 2).
ASTRO = American Society for Therapeutic Radiology and Oncology; Nx = lymph nodes not tested; PSA = prostate-specific antigen; Tx = T grading unknown.
Ganzer R. BJU Int 2013;112:322–329; Thüroff S, Chaussy C. J Urol 2013;190:702–710; Crouzet S. Eur Urol 2014;65:907–914.
Incidental disease
Histologic examination reveals prostate cancer in up to 8% of the patients who undergo adenomectomy/holmium-laser enucleation or TURP because of symptomatic benign prostatic hyperplasia. 18
Results have been reported in 65 patients treated with HIFU for incidental prostate cancer.
The PSA nadir of 0.07 ng/mL and the PSA velocity of 0.01 ng/mL/year indicated that HIFU can be used as a curative therapy in patients with incidental prostate cancer.
HIFU-related morbidity
The most common side effects of primary HIFU therapy include prolonged voiding dysfunction and retention caused by edema, necrosis, or bladder outlet obstruction, as well as erectile dysfunction 21 (Table 3).
CA = postoperative catheter duration; ED = erectile dysfunction; F = foley catheter; FIS = fistula; GI = incontinence grade I, which is loss of urine under heavy exercise requiring 0–1 pad/day; GII = incontinence grade II, which is loss of urine under light exercise requiring >1 pad/day; GIII = incontinence grade III, which is loss of urine under any exercise requiring >2 pads/day; INC = incontinence; NR = not reported; PR = postoperative retention; SP = suprapubic catheter; S&S = stricture and stenosis; TURP = transurethral resection of the prostate; UTI = urinary tract infection.
HIFU therapy in locally advanced, hormone-refractory, and advanced disease
In contrast to most published trials of HIFU therapy that report the outcomes in patients with Stage T1–T2 disease or radiation failure, the results of a trial that enrolled 113 patients with Stage T3–T4 disease followed for a median of 4.6 years were recently presented. 22 The median PSA velocity of this cohort was 0.19 ng/mL/year and the cancer-specific survival was 96.4%. Another study reported the outcomes of 55 men with PSA progression and local biopsy-proven tumor recurrence during definitive hormonal ablation therapy who received HIFU for hormonal-resistant prostate cancer. 23 With a mean follow-up of 21 months, the prostate cancer-specific survival was 87.3%.
Preliminary results of palliative treatment with HIFU in patients with advanced prostate cancer showed promising findings based on reductions in local morbidity such as rectal compression, infravesical obstruction, hydronephrosis, hematuria, and pelvic pain syndromes. Unpublished data from several large patient groups (n > 70) with Stage T3 and CRPCa with follow-up of 10 years have shown a post-HIFU PSA velocity of 0.19 ng/mL/year in T3 disease without additional hormone ablation. Local tumor ablation with HIFU has also resulted in a PSA reduction of 80% in CRPCa cases. There was also evidence of a synergistic effect with hormone ablative therapies that was reflected in the delay of onset of hormone resistance. 10,24
HIFU as Salvage Therapy
Rationale
HIFU can be used as salvage therapy for locally recurrent disease following almost every curative prostate cancer modality, including external radiation, low-dose rate and high-dose rate brachytherapy, cryoablation, primary HIFU, biochemically progressing PSA, and after combined pretreatment including RPE. One of the factors accounting for the attractiveness of salvage HIFU is related to the extremely limited treatment options for men with recurrent disease following curative therapy. According to CaPSURE data, 20 63% of the patients treated with EBRT experience disease recurrence. For these patients, Androgen deprivation therapy was used as salvage therapy in 93.5%, and definitive local therapy in only 3.9% (salvage RPE 0.9% and cryoablation 3.0%). The appeal of salvage RPE and cryoablation following local radiation failure is more theoretical in nature; in practice, their use represents a complex procedure associated with extremely high morbidity rates and procedural costs. 7
Salvage of radiotherapy failure
Salvage HIFU represents a viable treatment option for men experiencing recurrence after radiation therapy. Although the tissue alteration from radiation therapy results in a higher postoperative morbidity rate than is seen in primary HIFU therapy alone, 7 this does not alter the favorable risk/benefit ratio with the use of salvage HIFU treatment relative to the other available options. 25
Extremely limited experience exists with salvage HIFU following brachytherapy, but it appears that this approach is not associated with a significant increase in complications compared with primary HIFU. 5
Salvage of RPE failure
Therapeutic options for local recurrence following RPE are limited. HIFU offers a treatment option when local recurrence can be identified through TRUS and verified with biopsy. After a small number of patients with postprostatectomy failure were treated with HIFU, the treated areas showed negative biopsies in 77% of cases. During follow-up of 5 years, 91% of the patients showed no biochemical progression. 24 Nevertheless, salvage HIFU after RPE depends on a TRUS visible biopsy-proven target and cannot be used as “post-RPE radiation therapy” in case of R1 resection.
Salvage RPE following HIFU failure
RPE was performed in seven patients experiencing failure following treatment with HIFU between 1996 and 2000 in our institution. Prior treatment with HIFU created severe fibrotic adhesions between the rectum and Denonvilliers fascia, and although this made salvage RPE more technically demanding, it did not result in higher morbidity compared with a standard prostatectomy.
Focal and Partial HIFU Therapy
Over the past 25 years, the average life expectancy of men has increased almost 4 years, while the average age of prostate cancer diagnosis has decreased 10 years. 26 Prostate cancer is also detected at a much earlier stage than two decades ago, with the majority of patient candidates for curative whole-prostate therapy. A sizable number of patients with small-volume monofocal tumor are being overtreated with whole-gland approaches that surgically remove or irradiate the entire prostate, and a great need exists for a focal approach to the treatment of small-volume single-lobe prostatic tumor.
The goal of focal HIFU therapy is to provide a partial treatment that is limited to the tumor and a safety margin in patients with noninvasive, monofocal, localized prostate cancer. Such an approach would preserve normal genitourinary function while treating the malignancy with sufficient efficacy. 27 Different focal treatment approaches with HIFU are currently being evaluated. A precise focal therapy that treats a maximum 25% of prostate volume without TURP (hemiablation without TURP) and a potency-preserving partial therapy that excludes the contralateral lobe/capsule and neurovascular bundle by sparing 5 mm of tissue on the contralateral lobe and treating up to 90% of the prostate. 15
Immunologic Response with HIFU Therapy
Several recent studies have examined the potential of HIFU to initiate an immune response. Wu and colleagues studied the effect of HIFU on systemic antitumor immunity, particularly T lymphocyte-mediated immunity in cancer patients. 28
It has been suggested that endogenous signals from HIFU-damaged tumor cells may trigger the activation of dendritic cells, playing a critical role in a HIFU-elicited antitumor immune response. 29 Results showed that HIFU elicited a systemic antitumor immune response that was related closely to dendritic cell activation, and that dendritic cell activation was more pronounced when tumor cells were mechanically lysed by HIFU.
Future Directions of HIFU for Prostate Cancer
The efficacy in cancer control of HIFU and other focal therapies will depend less on the development of therapeutic tools than on diagnostic technologies that can more accurately image and localize tumor lesions and foci. When this goal is reached, HIFU will be the ideal therapeutic tool for focal prostate cancer treatment. The efficacy in cancer control of HIFU and other focal therapies will depend on precise diagnostic technologies as well as on accurate, safe, and easy applicable technologies to localize and ablate tumor foci. 30 Today, already available serial HIFU devices show significant technologic and applicable differences, as shown in Table 4, in handling and efficacy; besides picture fusion, several advancements are being investigated, including multiparametric MRI, high-resolution TRUS, contrast-enhanced ultrasound, elastography, and Doppler for precise lesion targeting.
HIFU = high-intensity focused ultrasound; OR, patients treatment position; TRUS = transrectal ultrasound.
Conclusion
Prostate cancer is now diagnosed at an earlier disease stage in younger patients with a longer life expectancy than it was 20 years ago before widespread PSA screening. As a result, the window for curative therapy has been extended, and with patients living longer after definitive therapy, a greater emphasis is now placed on treatment-related morbidity and its impact on patient's quality of life. Local recurrence occurs in 10% to 50% of patients regardless of curative approach, and the treatment of prostate cancer has evolved from a singular treatment to a multimodal, sequential approach that greatly accommodates the use of minimally invasive therapies such as HIFU.
In addition, HIFU can be repeated in cases of local recurrence, which is not an option with other treatment modalities for localized prostate cancer such as external radiation, cryosurgery, and brachytherapy.
The use of HIFU should not be viewed as a substitute or replacement for classical therapy, but instead as a therapeutic first choice in monofocal well-differentiated disease. The initial use of HIFU can help postpone the need for invasive therapies associated with greater morbidity such as surgery or radiation, allowing the patient a longer period without the risk of living with treatment-related genitourinary side effects. 31
Transrectal HIFU should be given serious consideration as a curative therapy in localized disease as well as a palliative adjuvant therapy in all other tumor stages. Ongoing improvements in imaging technologies are expected to further enhance the efficacy of HIFU.
Footnotes
Author Disclosure Statement
No competing financial interests exist.