
Abstract
Introduction:
Literature suggests that the percutaneous punctures for percutaneous nephrolithotomy (PCNL) must be performed at the papilla of the renal calix and a puncture at the infundibulum or the direction of the pelvis is not advisable because of increased hemorrhagic risk. A prospective randomized study was conducted to investigate the safety in terms of blood loss of the infundibular approach for PCNL.
Materials and methods:
Patients with renal stones with an accumulative size of at least 2 cm were randomly assigned to one of two parallel groups to undergo PCNL with either papillary (Group 1) or infundibular (Group 2) renal access. The primary outcome measures were the reduction in hemoglobin on first postoperative day and the need for transfusion during the first postoperative month. Secondary endpoints included the operative and fluoroscopy time, number of accesses performed, overall complication rate, hospitalization time, and complications up to 3 months.
Results:
In total, 27 and 28 patients were enrolled in Groups 1 and 2, respectively. Patient age, body mass index, and stone size were similar among the groups (p = 0.672, 0.256, and 0.889, respectively). Reduction in hemoglobin and transfusion rate did not differ among Groups 1 and 2 (p = 0.916, p = 1.0, respectively). Operative time was higher in the case of Group 1 (p = 0.027). The overall complications rate was 7.4% for Group 1 and 7.14% for Group 2. Hospitalization time was not significantly different in the study groups (p = 0.724).
Conclusions:
The infundibular approach for PCNL to the posterior middle renal calices is not associated with higher blood loss or transfusion rate in comparison with the respective approach to the fornix of the papilla when the currently described technique is performed.
Introduction
P
Materials and Methods
Inclusion–exclusion criteria, study groups, and randomization process
The study and the surgical intervention took place at the University Hospital of Patras. The details of the study have been registered in a public database (ISRCTN Serial No. 11393/June 16, 2015). Reporting of the investigation was done according to the PRISMA statement.
Patients were randomly assigned to one of two parallel groups to undergo PCNL with either infundibular or papillary renal access. The randomization method employed was that of sequentially numbered opaque sealed envelopes. The envelope was opened before anesthesia of the patient in the operative room. Eligible participants were all patients with renal stones of a cumulative stone size of at least 2 cm and indication for PCNL. The inclusion and exclusion criteria are presented in detail in Table 1. Patients in Group 1 underwent PCNL with access and tract dilatation to the papilla of the desired calix (control) whereas those in Group 2 underwent PCNL with access to the infundibulum of the calix.
Surgical technique
The technique for PCNL and perioperative care protocols has been previously described in detail. 7 The technical details are presented in Table 2.
PCNL = percutaneous nephrolithotomy.
All surgeries were performed by specialist surgeons.
Outcome measures, perioperative care, and follow-up
The patients were discharged on the second to fourth postoperative day based on the presence of clear urine in the Malecot tube. The primary outcome measures were the reduction in hemoglobin till the discharge day and the need for transfusion during the first postoperative month. The outcomes of the study and the recorded parameters are presented in Tables 1 and 3, respectively. Complications were classified according to Dindo et al. 8 The physicians evaluating the patients were blinded regarding the approach. Statistical analysis methods are presented in Table 1.
Results
Patient population
The patient recruitment process is described in Figure 1. In total, 27 and 28 patients were enrolled in Groups 1 and 2, respectively. Patient age, body mass index, and stone size were similar among the groups (p = 0.672, 0.256, and 0.889, respectively) (Table 4).
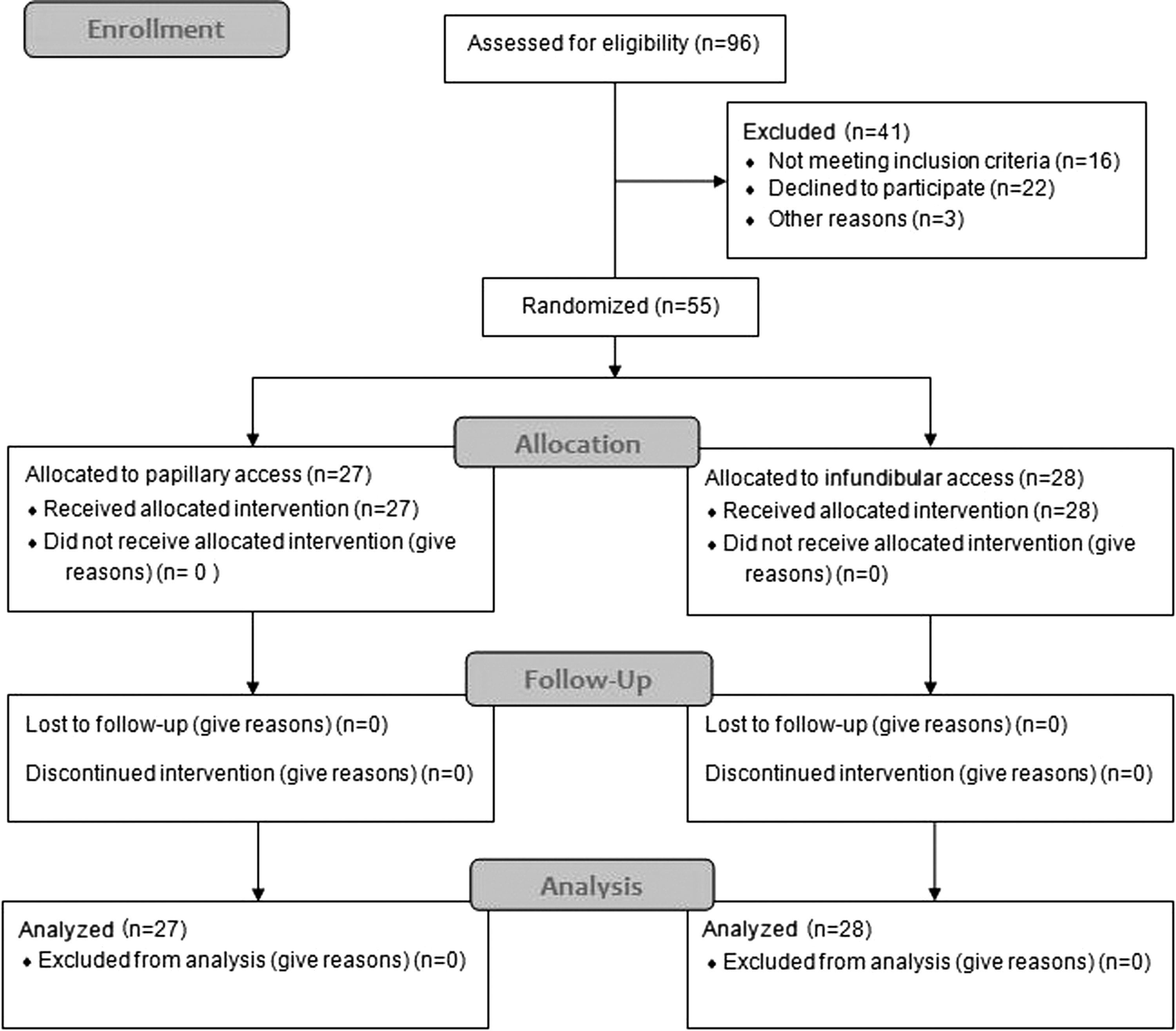
Flow diagram of the recruitment process.
Numerical values are presented as mean values ± standard deviation.
BMI = body mass index, F = female, L = left, M = male, R = right.
Primary endpoints
Reduction in hemoglobin between the preoperative and the discharge day values was similar among the groups of the study (p = 0.916). The reduction in hemoglobin had an average value of 1.54 ± 1.29 and 1.35 ± 0.79, respectively (Table 5). Transfusion rate was similar (p = 1.0) and only one patient of Group 2 required transfusion. Thus, bleeding was not higher in any of the evaluated approaches.
Numerical values are presented as mean values ± standard deviation.
CT = computized tomography nonenhanced; KUB = kidney, ureter, and bladder radiograph, SWL = shock wave lithotripsy.
Secondary endpoints
The patients required an average time of 51.97 ± 16.1 and 43.21 ± 12.38 minutes in Groups 1 and 2, respectively. Operative time was higher in the case of Group 1 (p = 0.027). The number of multiple accesses was higher in the case of Group 1 with four cases of multiple accesses compared with none in Group 2. This trend did not prove to be significant (p = 0.051). The middle infundibular punctures represented 85.7% of the overall patients of Group 2 (26/28). The overall complications rate was 7.4% and 7.14%, respectively. No statistical significance was noted (p = 1). All complications were observed within the first 4 weeks of follow-up. Hospitalization time was not significantly different in the study groups (p = 0.724). The average hospitalization time was 5.57 ± 1.70 and 5.80 ± 2.56 days for Groups 1 and 2, respectively. Tables 4 –6 summarize the data and statistical analysis of the investigation.
Discussion
The fornix of the papilla is the preferred site for a puncture to the collecting system and the principle behind this approach relies on the anatomical distribution of the blood vessels within the kidney. 1,6 Anatomical studies showed that the puncture to the upper infundibulum was related to arterial injury in 67% of the cases. The access through the mid and lower caliceal infundibula was associated with an arterial lesion in 23% and 13% of the studied kidneys. 1,5 The endourologists have embraced the concept that the minimum damage in the domains with ample vascular supply should result in minimum hemorrhagic complications, and a papillary access would be the most appropriate approach.
The mentioned anatomical studies are not associated with clinical evidence, confirming the clinical advantage of the papillary access over other approaches. The only recent study using the modern equipment and instrument for the performance of the infundibular approach to the PCS for PCNL has been recently reported by our group. 7 This retrospective study showed results regarding complications and blood loss similar to the current literature and provided the first clinical evidence that a noncaliceal puncture could be routinely performed with safety. As the retrospective nature of the study was related to limitations, a prospective randomized trial was designed to provide more substantial evidence on the risk of bleeding of the infundibular in comparison with the papillary access.
This study showed that there is no difference in blood loss between the infundibular and the papillary approach because both the reduction in hemoglobin (p = 0.916) and the transfusion rates were similar (p = 0.49). These results show that the blood loss related to the “more aggressive” puncture to the renal infundibulum may not be justified. In fact, the anatomical studies available are based on the evaluation of vascular injuries induced by the puncture of different access sites but have never considered the damage caused by the tract dilatation process. A dilatation of the tract to 30F represents an entirely different degree of invasiveness to the renal tissue in comparison with the needle puncture. Structures such as vessels are avoided during puncturing and could be easily injured with the tract dilatation process. Moreover, anatomical orientation of the kidney and any effect of the surrounding tissue were not considered in the available anatomical studies because the kidneys were removed from the cadavers. 3 –5 Another issue not addressed by the studies already mentioned is the possible impact of the dilatation of the PCS on its anatomical relationships with the intrarenal vessels. As majority of the stone patients have dilated collecting systems, the currently available evidence on the probability of vascular injury could not describe with accuracy these systems. The mentioned considerations question the acceptance of the papillary puncture because of its safety regarding bleeding, and the concept of performing only papillary punctures should probably be revisited.
Access to the infundibulum of the posterior middle calix was performed in majority of patients of Group 2 (24/28 patients) as it is the standard practice for performing infundibular access at our institution (Fig. 2). 7 Access to the infundibulum provides a higher degree of movement for the nephroscope. The lower and middle calices, as well as the renal pelvis, can be approached. Stones in the upper calices are also possible to treat through an infundibular middle caliceal access in some cases (i.e., dilated PCSs). The need for multiple tract dilatations was diminished in Group 1 as none of the patients required additional tract dilatations. The stone size and the location of stones were similar among the groups and may not have biased the selection of the site of access to the PCS (Table 4). The middle caliceal approach is also advocated as a favorable access site by other investigators and may possess advantages over other infundibular punctures. 9,10 Specifically, the posterior segmental artery is in close relationship with the upper infundibulum or the junction of the pelvis is in close relationship with the upper infundibulum in 57% of the cases. 5 The upper infundibulum is practically encircled by the ventral and dorsal branches and probably prone to bleeding complications. 11 In contrast, the lower infundibular access is related to an incidence of arterial injury in 13% of the cases. 1,5 Nevertheless, the accuracy of the mentioned evidence was not adequately addressed by this study because the accesses to the upper or lower infundibulum were limited in number. Still, the patients treated using these approaches were not associated with any complication. Considering the mentioned evidence, access to the infundibulum of the posterior middle calix represents a safe method for reaching the majority of the collecting system at least with the PCNL technique proposed by the authors.

Intraoperative images during the puncture process.
The lower operative time for Group 2 than for Group 1 presented an additional advantage of the approach (p = 0.027). This benefit could be related to the need for establishing additional access tracts in Group 1 (four multiple access tract cases). It could also be proposed that the higher degree of movement of the instrument in the infundibular approach may additionally facilitate the removal of the stones. Specifically, a higher number of cases required the use of flexible nephroscope for removal of stones in Group 1 than in Group 2, whereas fluoroscopy time was similar (Table 4, p = 0.389). Thus, the additional time could be attributed to the establishment of a second tract and to the endoscopic manipulations.
The duration of hospitalization was similar between the groups (p = 0.724). Nevertheless, the average hospital stay times of 5.53 ± 1.64 and 5.82 ± 2.48 days for Groups 1 and 2, respectively, do not compare favorably to those in the literature. 12 –14 This observation is related to the public health system of the country. The patients are admitted the day before surgery and the hospitalization time is increased for at least 1 day. Complications were encountered in 7.4% and 7.14% of the patients of Groups 1 and 2, respectively (p = 1). The complications of patients of Group 1 were of a higher Clavien grade and their management required interventions. This observation is probably a random phenomenon related to a sample calculated to elucidate differences in blood loss and is probably not related to the approach.
A limitation of this study is the number of the included patients, which may not allow for reliable results in parameters other than those considered in the sample size calculation. Nonetheless, the current population showed clear results regarding the blood loss and interesting results on several qualitative and quantitative parameters. Stone-free status did not represent a primary endpoint of the study and was not reported in this study. Further evaluation would elucidate the efficacy of the infundibular approach in the management of renal stones. An additional limitation is the lack of a follow-up extending more than several weeks or even months. The current population represents patients referred to our high-volume urolithiasis center, and the patients are referred to their treating physicians after the procedure. The incidence of long-term complications such as the incidence of infundibular stenosis was not investigated and the study could not provide any evidence on the issue. Nevertheless, a potential infundibular stenosis would produce symptoms because of caliceal dilatation, and all symptomtic cases were followed by radiographic evaluation during the follow-up period. No case of symptomatic infundibular stenosis was observed in the entire cohort. Given the large variation of PCNL access techniques, further evaluation is required to ensure that our favorable outcomes in central punctures are replicated by other access techniques (i.e., ultrasound access) before establishing the nonpapillary access as a safe approach.
Conclusion
The infundibular approach for PCNL to the posterior middle renal calices is not associated with higher blood loss or transfusion rate than the respective approach to the fornix of the papilla.
Footnotes
Author Disclosure Statement
No competing financial interests exist.