
Abstract
Introduction:
To investigate whether ureteroscopic biopsy (URS-Bx) for upper tract urothelial carcinoma (UTUC) before radical nephroureterectomy affects intravesical recurrence (IVR).
Patients and Methods:
Of the 515 patients receiving radical nephroureterectomy for UTUC between 1998 and 2012, 387 patients were included for the analysis. URS-Bx was performed in 69 patients (17.8%). Patients were stratified according to tumor location, and the impact of URS-Bx on IVR was evaluated after adjusting for other clinicopathologic variables.
Results:
IVR occurred in 163 patients (42.1%). The postoperative 5-year IVR-free survival was not significantly different according to URS-Bx in the overall patient group (54.0% vs 39.3%, p = 0.056). In patients with renal pelvic tumor, IVR-free probability was lower in patients with URS-Bx than in patients without URS-Bx (39.6% vs 62.2%, p = 0.012), although IVR-free survival in patients with ureteral tumor was equivalent (36.7% vs 45.8%, p = 0.946). In multivariate analysis, previous bladder tumors (hazard ratio [HR], 1.65; p = 0.016) were a significant risk factor for IVR in all patients and ureteral tumor location (HR, 1.35; p = 0.071) was associated with IVR, although statistical significance was not achieved. In patients with renal pelvic tumor, URS-Bx HR, 1.98; p = 0.020 was the only risk factor for IVR. However, URS-Bx was not associated with IVR in patients with ureteral tumor, although previous bladder tumor HR, 1.74; p = 0.028 was a risk factor for IVR.
Conclusion:
URS-Bx is a significant risk factor for IVR in patients with renal pelvic tumor and should be performed after sufficient consideration in these patients if other examinations are uncertain.
Introduction
I
Current imaging studies, including CT and intravenous and retrograde pyelography, cannot accurately detect flat or small lesions in the upper urinary tract. 4 Ureteroscopic examination is regarded as a suitable diagnostic modality for detecting UTUC when other studies are ambiguous because it can offer direct visualization of the upper urinary tract. 5 Moreover, it can obtain biopsy specimens during the procedure and confirm the tumor histology, grade, and stage. 6,7
However, ureteroscopic biopsy (URS-Bx) before radical nephroureterectomy in UTUC patients can theoretically increase the risk of IVR. Large amounts of tumor cells can become detached during URS-Bx and shed into the urine. Moreover, the irrigation fluid used during URS-Bx might intensify tumor cell detachment and shedding. These detached tumor cells can settle down in the urinary bladder after URS-Bx. However, the impact of URS-Bx on IVR in UTUC patients remains poorly identified, although some previous studies have assessed the relationship between ureteroscopic procedures and IVR. 8,9
Tumor location was reported to be associated with IVR in patients with UTUC. 10,11 In addition, the impact of URS-Bx on IVR can vary according to the tumor location because the procedure time, amount of irrigation fluid, and devices for URS-Bx generally depend on tumor location. In this regard, we hypothesized that the impact of URS-Bx on IVR might be modified by tumor location and, thus, assessed the impact of URS-Bx on IVR after stratifying patients according to tumor location.
Patients and Methods
The Institutional Review Board of our institute approved and is responsible for overseeing this study. The medical records of 515 UTUC patients who underwent radical nephroureterectomy at our institute from 1998 to 2012 were initially eligible for this study. Of these patients, 44 without preoperative cystoscopic examination, 25 with a positive urothelial resection margin on pathologic examination, and 59 who underwent neoadjuvant and/or adjuvant chemotherapy were excluded from the analysis. Finally, 387 patients were included in this study. Immediate intravesical chemotherapy after radical nephroureterectomy was not performed in any patient.
URS-Bx was selectively performed to confirm tumor histology before definitive surgery based on the clinician's judgment regarding preoperative imaging studies and urine cytology. URS-Bx was performed under general anesthesia. In general, a 31-cm-long semirigid ureteroscope with a 6/7.5F diameter (Richard Wolf, Knittlingen, Germany) was selected to inspect the distal ureter and a 43-cm-long semirigid ureteroscope with a 6/7.5F diameter (Richard Wolf) was selected to evaluate the upper ureter or renal pelvis. For URS-Bx, biopsy forceps were used to obtain suspicious tissues. If a suspicious lesion was inaccessible using the semirigid ureteroscope, a 68-cm-long flexible ureteroscope with a 6/9.9F diameter (Richard Wolf) was selected for the procedure. During URS-Bx, sufficient tissues were obtained using multiple biopsies.
Preoperative cystoscopic examination was performed before radical nephroureterectomy in all patients. If any suspicious mucosal lesions in the urinary bladder were identified during cystoscopic examination, cystoscopic biopsy of the lesion was performed. Based on the cystoscopic and pathologic findings, subsequent transurethral resection of the bladder tumor was performed before nephroureterectomy and these patients were regarded as the patients with a previous bladder tumor. Radical nephroureterectomy was performed using standard procedures with bladder cuff excision. Open surgery was performed in 182 patients (47.0%), as well as hand-assisted laparoscopic surgery in 71 patients (18.3%), laparoscopic surgery in 129 patients (33.3%), and robotic surgery in 5 patients (1.3%). The kidney, ureter, and bladder were excised en bloc regardless of the operative method. Bladder cuff excision was performed extravesically regardless of the surgical method.
Cystoscopic examination and voided urine cytology were performed at least every 6 months for the first 5 years after surgery and then every year thereafter. If a suspicious lesion was identified on cystoscopic examination, cystoscopic biopsy and subsequent transurethral resection of the bladder tumor followed if clinically required. IVR was defined as any pathologically diagnosed urothelial carcinoma in the urinary bladder on cystoscopic biopsy or transurethral resection of the bladder tumor. Other examinations including chest radiography and CT were also performed every 6 months for the first 2 years and then annually to detect locoregional and/or distant metastasis. Median follow-up duration was 62 months (range; 2–214 months).
Patients were divided into two groups according to URS-Bx. In patients who underwent URS-Bx, the duration between URS-Bx and radical nephroureterectomy was calculated. The clinicopathologic characteristics of the patients were compared between the two groups using Pearson's chi-square test for categorical variables and Student's t-test for continuous variables. Quantitative data are expressed as mean ± standard deviation and qualitative data are expressed using frequency tables. Patients were additionally stratified according to tumor location, and pathologic characteristics were compared according to URS-Bx. Tumor location was determined based on preoperative imaging studies. A Kaplan–Meier curve and log-rank test was performed to evaluate and compare the impact of URS-Bx on IVR in all patients, those with renal pelvic tumor and those with ureteral tumor. The impacts of URS-Bx and other variables on IVR were evaluated using multivariate Cox proportional hazard analysis. Risk factors for IVR in patients with ureteral tumor and pelvic tumor were also separately assessed using multivariate analysis. Following univariate analysis, factors with p < 0.2 were entered into the multivariate model, followed by backward elimination to determine the factors most associated with the recurrence-free survival (RFS) and overall survival (OS). All statistical comparisons were performed using IBM SPSS Statistics Version 21 (IBM Corporation, Somers, NY). A p-value of less than 0.05 was considered to indicate a statistically significant difference.
Results
Among 387 patients, URS-Bx was performed in 69 patients (17.8%), 59 of whom underwent the semirigid ureteroscopic procedure and 10 of whom underwent the flexible ureteroscopic procedure. The median duration from URS-Bx to radical nephroureterectomy was 20 days (IQR, 9–30). The mean age of all patients was 63.8 years and 284 patients (73.4%) were male (Table 1). The tumor was located at the renal pelvis in 185 patients (47.8%) and at the ureter in 202 patients (52.2%). Bladder tumors were diagnosed before radical nephroureterectomy in 58 patients (15.0%). The pathologic stage of UTUC was as follows: 207 patients (53.5%) had Ta or T1 disease, 68 patients (17.6%) had T2 disease, and 112 patients (28.9%) had T3 or greater disease. Lymph node invasion was pathologically identified in 26 patients (6.7%). The tumor grade was high in 190 patients (49.4%). There were no significant differences in patient characteristics according to URS-Bx.
SD = standard deviation; URS-Bx = ureteroscopic biopsy.
When patients were stratified according to tumor location, there were no differences in pathologic characteristics in patients with renal pelvic tumor according to URS-Bx, including pathologic stage, lymph node invasion, tumor grade, and presence of lymphovascular invasion and carcinoma in situ (Table 2). In addition, pathologic characteristics were also equivalent according to URS-Bx in patients with ureteral tumor.
IVR occurred in 163 patients (42.1%) and 13 patients (8.0%) progressed to muscle-invasive bladder cancer during follow-up. In Kaplan–Meier analysis, the postoperative 5-year IVR-free survival in all patients was 51.4%. Although statistical significance was not achieved, the 5-year IVR-free survival was marginally inferior in patients who underwent URS-Bx compared with patients who did not undergo URS-Bx (39.3% vs 54.0%, p = 0.056) (Fig. 1). In patients with renal pelvic tumor, the postoperative 5-year IVR-free survival was 39.6% in patients with URS-Bx and 62.2% in patients without URS-Bx (p = 0.012). However, there was no difference in the 5-year IVR-free survival according to URS-Bx in patients with ureteral tumor (36.7% vs 45.8%, p = 0.946). In entire patients, 5-year overall survival was 73.9% and there was no difference in overall survival according to URS-Bx (75.1% vs 70.4%, p = 0.219).
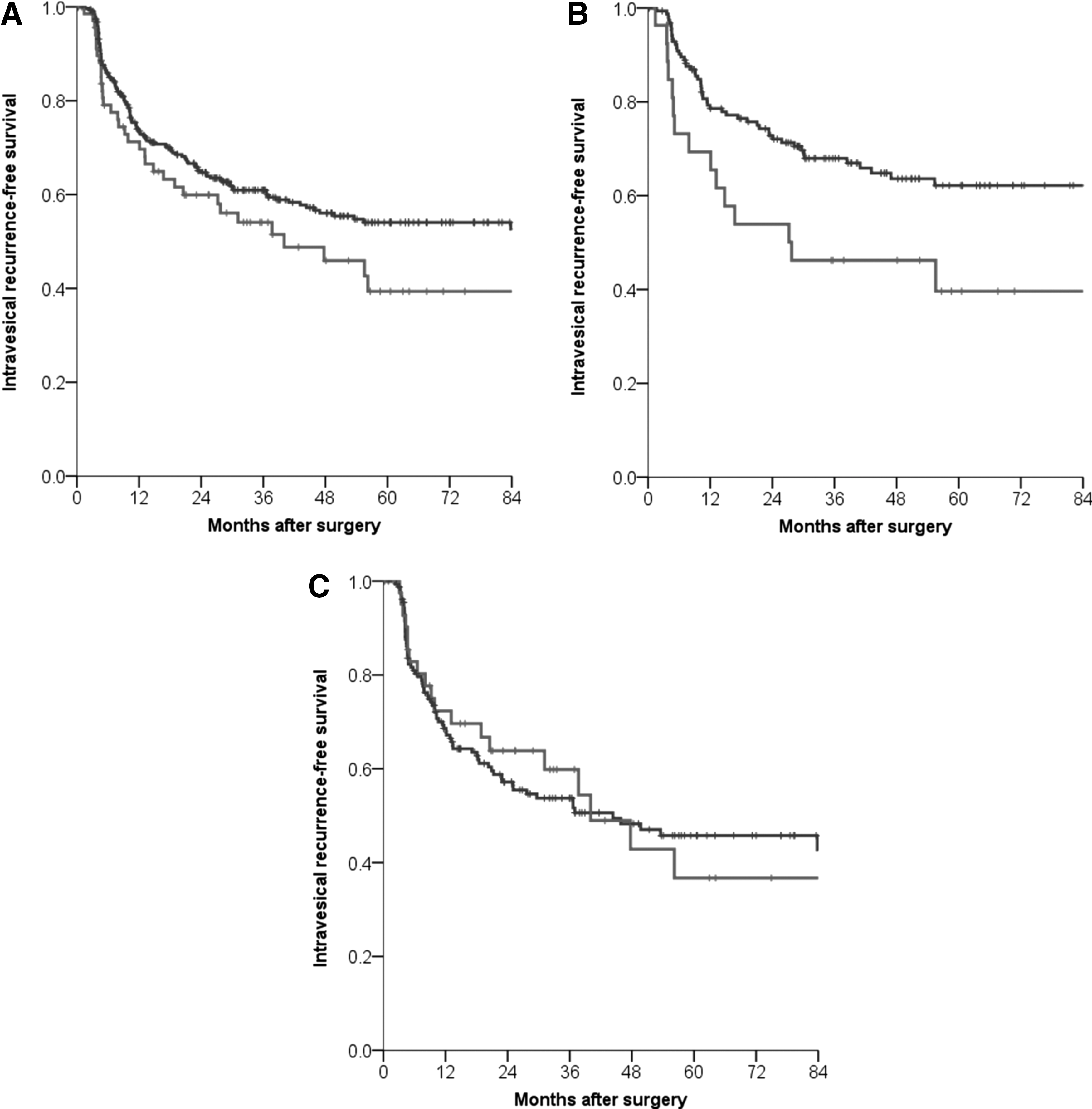
Intravesical recurrence-free probability according to ureteroscopic biopsy.
In multivariate analysis, previous history of bladder tumor (hazard ratio [HR], 1.65; p = 0.016) was a significant risk factor for IVR and ureteral tumor location (HR, 1.35; p = 0.071) was marginally associated with IVR in all UTUC patients (Table 3). In patients with renal pelvic tumor, URS-Bx HR, 1.98; p = 0.020 was the only independent risk factor for IVR. However, URS-Bx was not associated with IVR in patients with ureteral tumor. In patients with ureteral tumor, previous history of bladder tumor HR, 1.74; p = 0.028 was the only risk factor for IVR (Table 4).
Discussion
In this study, IVR occurred in about half of UTUC patients within 5 years after nephroureterectomy. Moreover, about half of the intravesically recurred patients had a repeat IVR, even though transurethral resection of the bladder tumor was performed. 12 Although IVR was reported to not be related to distant metastasis and survival, about 5% to 10% of tumors that recurred intravesically in a previous study progressed to muscle-invasive bladder cancer, which is in accordance with the findings in this study. 12 –14 It is important to avoid IVR after radical nephroureterectomy and several large studies have determined the risk factors for IVR. 8,9 In UTUC patients who underwent nephroureterectomy, gender, tumor location, tumor stage, and previous bladder tumor were reported to be risk factors for IVR. 8,9
Nonetheless, the impact of URS-Bx on IVR has not been clearly identified. Although there is still controversy about the impact of the preoperative ureteroscopic procedure on IVR, URS-Bx could theoretically intensify tumor cell detachment and shedding compared with ureteroscopic examination without biopsy. 8,9,15 However, to our knowledge, no study to date has revealed the impact of URS-Bx on IVR. Although some previous studies identified the impact of ureteroscopic procedures, including URS-Bx, on IVR in UTUC patients, this aspect remains controversial.
In this study, the probability of IVR was not significantly different according to URS-Bx after adjusting for other variables when all patients, irrespective of tumor location, were enrolled in the analysis. However, we found in these analyses that the effects of URS-Bx on IVR could vary according to tumor location. These results might help to explain the continuing controversy surrounding this topic. Tumors located in the ureter have previously been reported to have a higher risk of IVR than those located in the renal pelvis. 11,16 We speculate that these results might be due to the short distance from the tumor to the bladder and the faster urine flow in the ureter than in the renal pelvis. Because sufficient tumor cells are thought to have already been shed into the bladder in patients with ureteral tumor, URS-Bx might not induce an additional increment in IVR probability in these patients. In contrast to ureteral tumors, fewer tumor cells are thought to reach the urinary bladder in patients with renal pelvic tumor if URS-Bx is not performed. In other words, URS-Bx might offset the protective advantages of renal pelvic tumors over ureteral tumors from the perspective of IVR.
Regarding the results of this study, the indications for URS-Bx should vary according to tumor location. If ureteral tumor is suspected on other preoperative examinations, URS-Bx should not be avoided and pathologic confirmation of the tumor before definite treatment could be considered. Although a recent meta-analysis reported that CT urography has a sensitivity of 96% and specificity of 99%, one concern about CT urography is that small or flat ureteral masses have to be detected by intraluminal filling defects alone because full ureteral opacification cannot be achieved using current protocols. 17,18 In addition, thickening of the ureter on CT is less predictive of UTUC than thickening of the renal pelvis. 4 In this regard, URS-Bx is thought to play a more crucial role in patients with ureteral tumor than in those with renal pelvic tumor. However, URS-Bx should be more selectively performed after sufficient consideration in patients with suspicious renal pelvic tumor on imaging studies because of the increased risk of IVR after URS-Bx. Moreover, additional treatment such as immediate intravesical chemotherapy could be considered if URS-Bx is performed in patients with renal pelvic tumor.
The value of URS-Bx before radical nephroureterectomy is still debated. Some clinicians prefer to perform URS-Bx because it permits histologic confirmation before definite therapy. In a previous study, about 3% of patients with suspected UTUC who underwent radical nephroureterectomy were reported to have a benign pathology on surgical specimens. 19 Moreover, preoperative ureteroscopic examination has been reported to not be related to oncological outcomes in terms of metastasis and cancer-specific survival, although URS-Bx resulted in a delay in the definitive treatment. 20,21 However, other clinicians argued that care should be taken when URS-Bx is performed because of an increased risk of IVR and delay of definite treatment. 9,15,22 In addition, URS-Bx cannot be regarded as a definitive diagnostic examination because false negatives cannot be excluded, even when pathologic results are negative for malignancy. 23,24 During the study period, the incidence of benign pathology after radical nephroureterectomy was 3.1% in patients who did not undergo URS-Bx. This was similar to that of our previous study, which showed an incidence of 2.9%. 19 In this regard, clinicians need to carefully consider the pros and cons of URS-Bx in suspected UTUC patients, particularly in those with a suspected renal pelvic tumor.
If URS-Bx is imperatively performed for renal pelvic tumor, postoperative intravesical chemotherapy can be considered. Single-dose intravesical chemotherapy is reported to reduce the relative risk of IVR without serious adverse events and meta-analysis revealed that immediate intravesical instillation was effective for preventing IVR in patients with UTUC. 2,25,26 Moreover, a recent study suggested that intravesical instillation of chemotherapy at the time of nephroureterectomy was a safe and feasible method to reduce the risk of IVR. 27 In this regard, postoperative intravesical chemotherapy could be regarded as a possible option for patients with renal pelvic tumor who undergo URS-Bx, although the optimal regimen and timing of the intravesical chemotherapy remain to be determined. However, intravesical chemotherapy should be performed only in patients with flawlessly repaired bladder without any suspected leakage because extravasation could induce varying degrees of damage. 28
This study had several limitations of note, in addition to its retrospective design. The first was that a semirigid ureteroscope was used in most patients with tumors located in the upper ureter and renal pelvis. Thus, differences in IVR according to the type of ureteroscope could not be assessed. This study was also limited by the fact that impacts of other ureteroscopic procedures were not assessed. These data cannot be compared with those of ureteroscopic examination without biopsy. In addition, differences between URS-Bx and ureteroscopic examination without biopsy should be assessed in a future study. Another limitation was the small number of patients. In our study population, URS-Bx was performed in a limited number of patients, particularly in those with renal pelvic tumor. In this regard, the results of this study should be interpreted with caution, and they need to be verified in a large multicenter study, although other studies that assessed the impact of ureteroscopy on IVR enrolled a similar number of patients. In addition, differences in the IVR of ureteral tumor according to tumor location (proximal vs mid vs distal ureter) were not assessed in our current analyses because of the small number of patients and should be assessed in future studies. Nonetheless, these results do provide some important insights into selecting the diagnostic procedure in UTUC patients.
Conclusion
In patients with renal pelvic tumor, URS-Bx is a significant risk factor for IVR, although it is not associated with IVR in patients with ureteral tumor. Considering the impact of URS-Bx on IVR in patients with a renal pelvic tumor, URS-Bx should only be performed for suspected renal pelvic tumor that remains ambiguous when other examinations have been performed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.