
Abstract
Objective:
To assess the current treatment of benign prostatic obstruction (BPO) in patients on ongoing oral anticoagulation (OA).
Methods:
An Internet survey was sent to all active members of the Endourological Society. The survey contained 32 questions regarding transurethral treatment of BPO in patients on ongoing OA, different techniques, and arising complications.
Results:
Out of all members (n = 2000) of the Endourological Society, 133 participated in our survey. Eighty-eight percent of the participants indicated to perform transurethral therapy of BPO on ongoing OA, whereas 60% of this group temporarily pause the OA during the intervention. Sixteen percent perform >30 transurethral interventions of BPO on ongoing OA per year. Most operations are performed under continuation of aspirin (58.2%). The continuation of adenosine diphosphate (ADP)-receptor inhibitors (22.1%), vitamin K antagonists (18.9%), factor Xa inhibitors (15.6%), or the combination of two oral anticoagulants (16.4%) is continued less often. The decision for the operation on ongoing OA is usually approved by the cardiologist (58%) or it cannot be stopped in case of emergency (29%). GreenLight laser (39%) was the most frequently used technique on ongoing OA, followed by monopolar or bipolar transurethral resection of the prostate (35%) as well as other sources of laser [holmium (12%), thulium (12%), diode laser (2%)]. Although OA was continued during the interventions, cardiovascular complications were observed in 31.6%.
Conclusions:
Current practice shows that the majority of a representative group of the Endourological Society members perform transurethral therapy of BPO in patients on ongoing OA. The incidence of perioperative complications under transurethral therapy of BPO on ongoing OA is lower than previously assumed.
Introduction
L
To date, there has not been any controlled randomized study or guideline that provides exact instructions regarding OA during TT. To assess this issue, we designed a questionnaire with the intention to gain insights on how OA is handled in clinical routine.
Methods
Using Survey Monkey®, an online survey was designed and mailed to all active members of the Endourological Society. The items of the survey were constructed to evaluate the contemporary practice in TT of BPO in patients on OA. The survey builds on a questionnaire by Netsch and colleagues, which was used to assess current practice of transurethral surgery for BPO in Germany. 8 Thirty-two questions were asked to evaluate different TT options of BPO and complications in patients on ongoing OA. The survey was sent twice at an interval of 4 weeks. All answers were tabulated and anonymized. SPSS was used for statistical analysis.
Results
Out of ∼2000 active members of the Endourological Society, 133 participated in the survey. As a result, 88% of all participants perform TT of BPO on ongoing OA and were included in further analysis. Sixty percent of the participants performing TT of BPO on ongoing OA strive for a temporary stop of the OA, whereas 30% start a bridging with heparin and 10% continue the OA (Fig. 1). Fifty-nine percent of the participants performing TT of BPO on ongoing OA perform 0 to 10 operations on OA per year, 17% perform 11 to 20 operations, 8% between 21 and 30, and 16% perform >30 operations on ongoing OA per year (Fig. 2). Aspirin was continued in 58.2% of the TTs. Adenosine diphosphate (ADP)-receptor inhibitors (22.1%), factor Xa inhibitors (15.6%), vitamin K antagonists (18.9%), or a combination of two oral anticoagulants (16.4%) was continued less often (Fig. 3). Continuation of OA during TT was most commonly indicated due to cardiologic reasons (58%) or emergency (29%). Other indications included the performance of the surgeon (9%) or the will of the patient (4%) (Fig. 4).
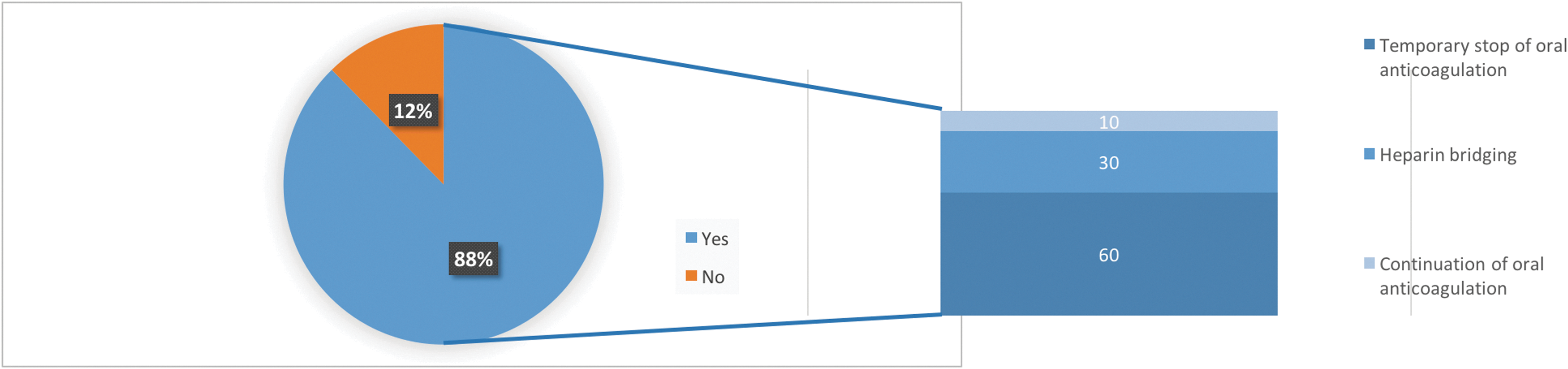
Eighty-eight percent of the participants performed TT of BPO on ongoing OA. Sixty percent of this group strive for a temporary stop of the OA, whereas 30% start a bridging with heparin and 10% continue the OA. BPO = benign prostatic obstruction; OA = oral anticoagulation; TT = transurethral therapy.

Frequency of transurethral interventions of BPO on continued OA per year.
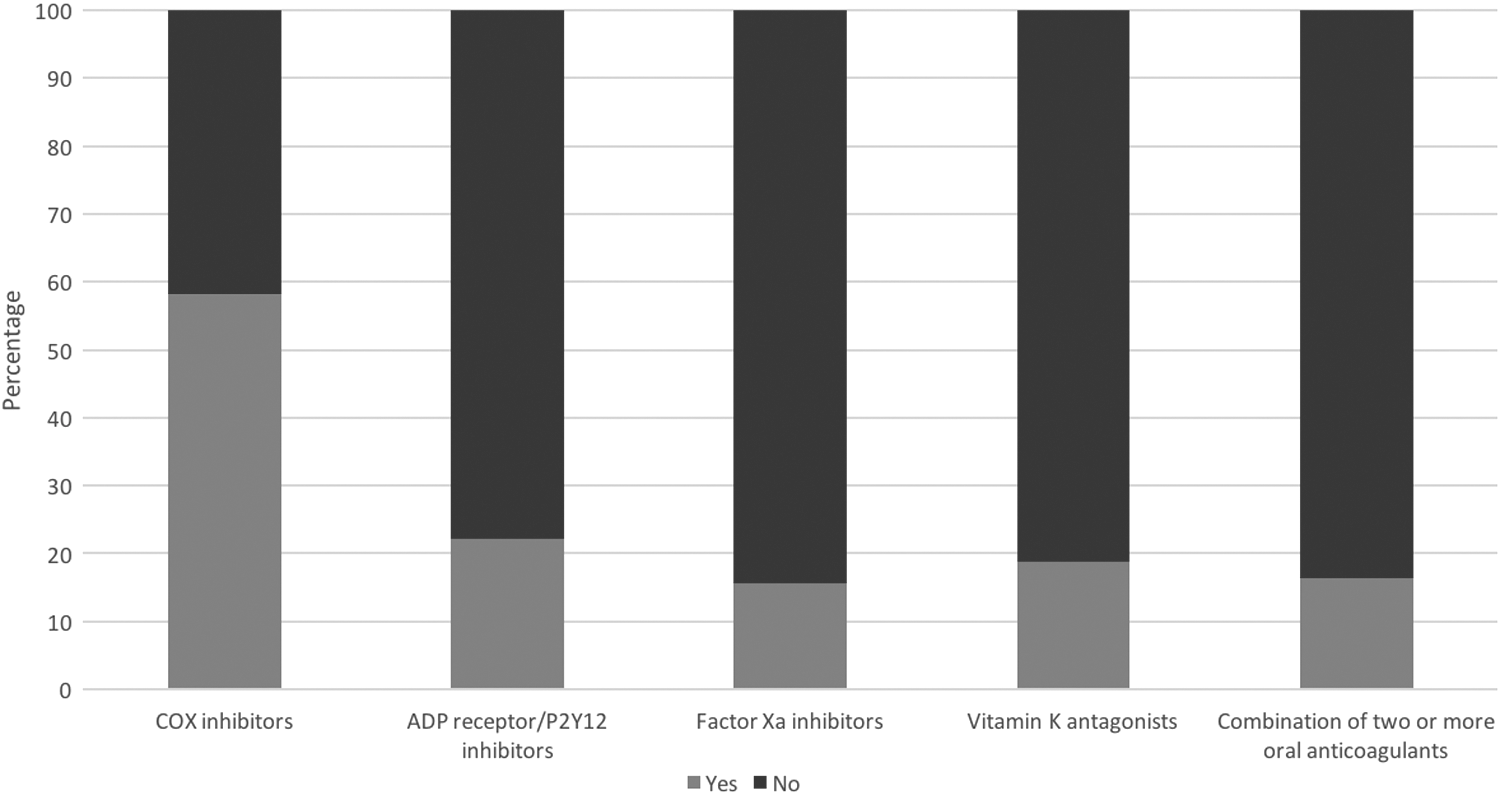
Frequency of used oral anticoagulants for TT of benign prostate hyperplasia.
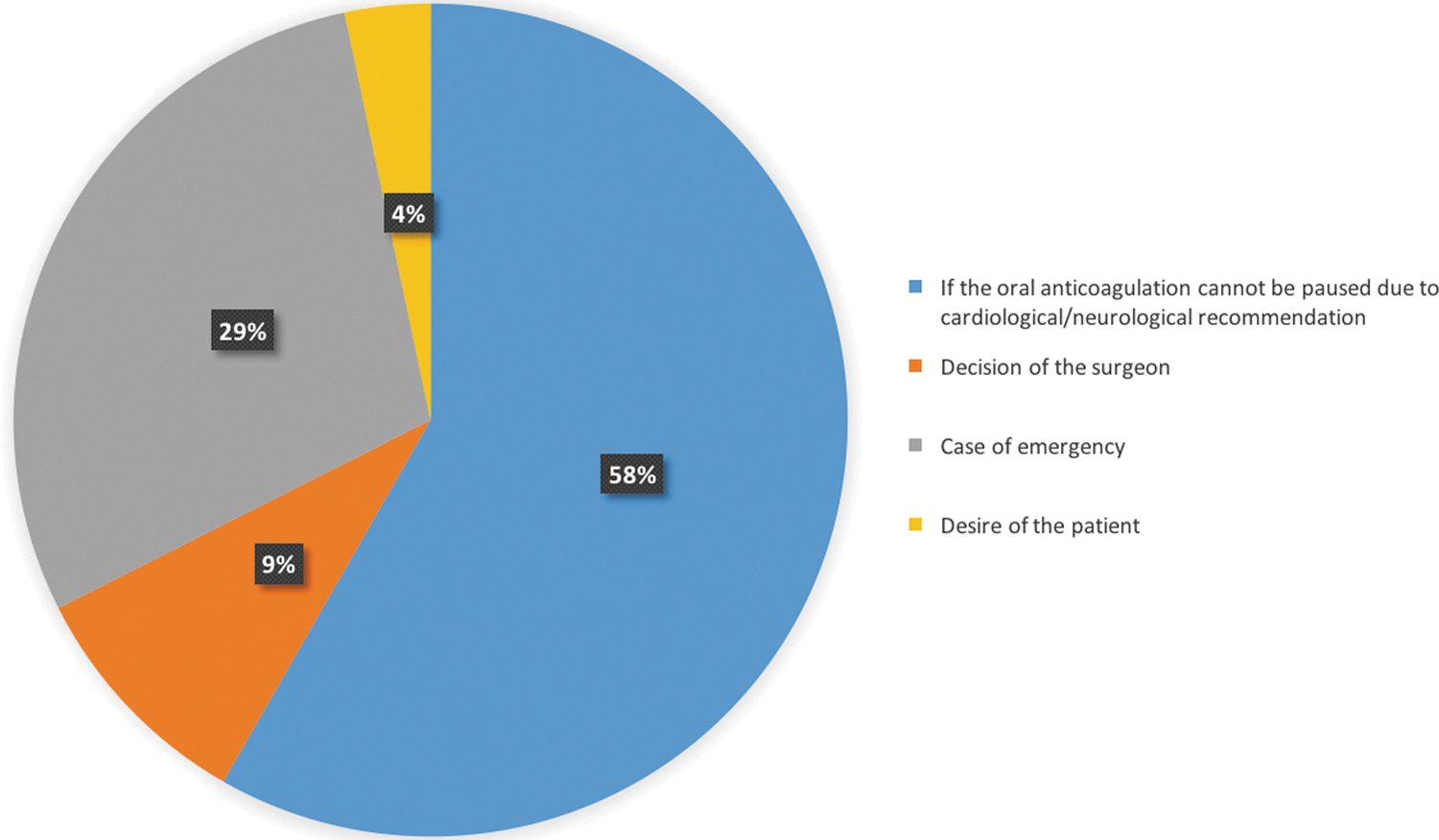
Indication for TT on ongoing OA.
The time until the catheter could be removed was significantly prolonged in the group of ongoing OA compared with the patients without OA. In the latter, the catheter could be removed within the first 2 days in 76% compared with 42.8% in the patients on OA. In average, patients with ongoing OA were catheterized for up to 3 to 4 days, whereas patients without OA were catheterized for 1 to 2 days. 5.8% of the patients without OA and 16.2% of the patients with OA were catheterized for >4 days (Fig. 5). The most frequent technique used for TT of BPO in patients on ongoing OA was the GreenLight laser (39%), followed by mono- or bipolar transurethral resection of the prostate (TURP) in 35%. Less often used were sources of holmium (12%), thulium (12%), and diode laser (2%) (Fig. 6A). The most preferred laser technique was vaporization of the prostate with 61%. One-fifth of the participants preferred an enucleation or a resection of the prostate in patients on ongoing OA with 19% and 20%, respectively (Fig. 6B).
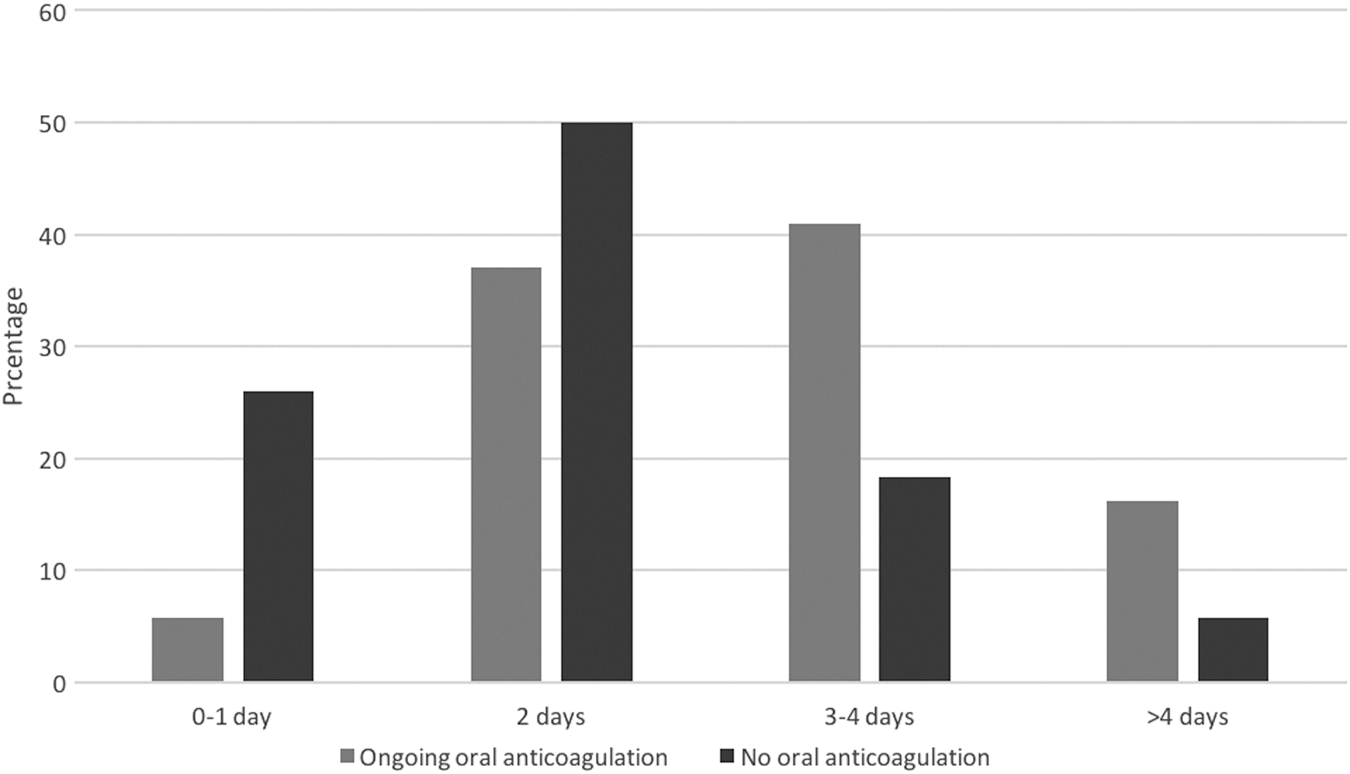
Days until removal of catheter.
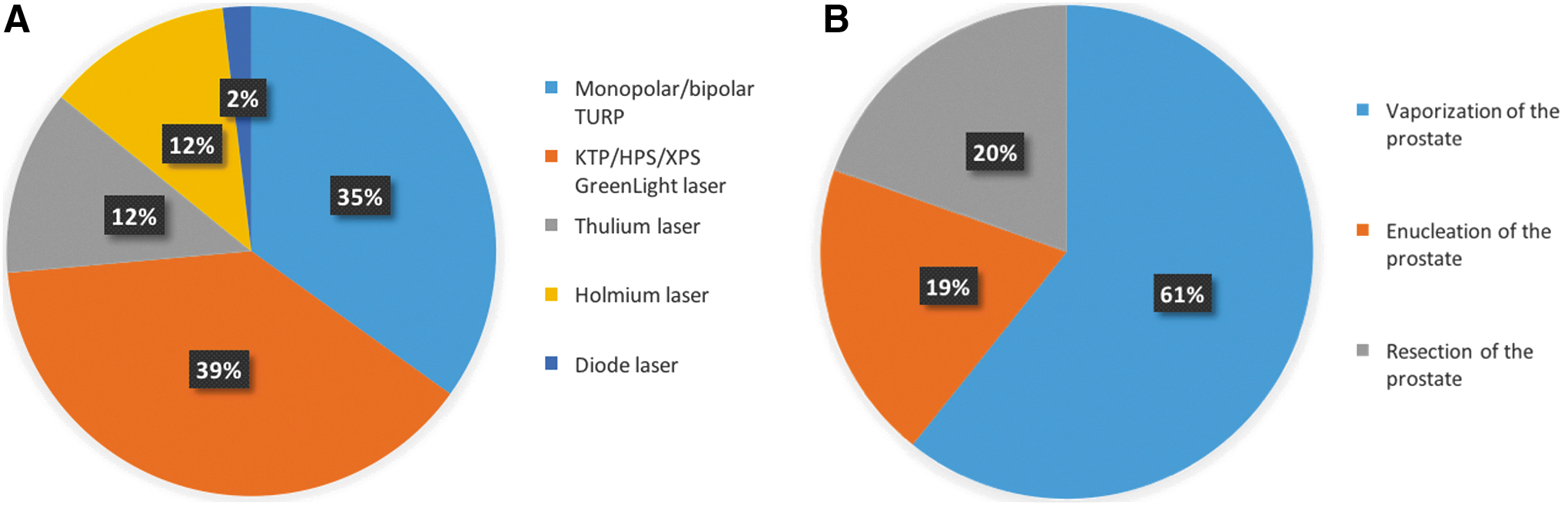
Preferred source of energy
Table 1 shows all estimated rates of perioperative complications. Most urologists estimated a perioperative complication rate lower than 5% for postoperative urinary retention, macrohematuria, rehospitalization, revision surgery, need of blood transfusion due to secondary bleeding, or cardiovascular complications, respectively. Despite a continued use of OA in patients during TT of BPO, cardiovascular complications are declared by 28% of the participants: heart attack (22.8%), stroke (16.5%), embolism (7.6%), and thrombosis (5%) are described perioperatively (Table 2).
BPO = benign prostatic obstruction.
Discussion
TT of BPO has evolved to be the surgery of choice for patients with LUTS. Even though TT of BPO using laser has been well established in the past few years, conventional TURP remains the most commonly used technique in males with LUTS referring to the EAU guidelines. 2 Independent of the technique, the OA impedes the performance of the surgeon. The National Health Interview Survey (NHIS) declared an increase of the use of aspirin from 2005 to 2010 up to 57%. 3 Stopping aspirin before a surgical intervention increases the risk of cardiovascular complications threefold. 4 EAU guidelines do not propose a therapeutic algorithm, although different studies presented promising results due to the TT on ongoing OA. 9 –12
In our study, 88% of the urologists have performed TT of BPO in one or more patients on continuous OA. The majority perform <10 TT on continuous OA per year. The complication rate regarding the required blood transfusions is estimated with 0% to 5% in 77% of the urologists. In the past years, the literature showed a shift in TT strategies of BPO with an increasing use of lasers compared with conventional TURP.
In a preliminary study regarding TT of BPO on OA in Germany, a similar survey was performed by Netsch and colleagues to evaluate the use of OA during transurethral surgery of the prostate. 8 Interestingly, 42.7% of the participants perform >30 prostate surgeries per year on ongoing OA vs 16% in this actual worldwide study. The observed rate of cardiovascular complications was stated with 12%, whereas 31.6% of our respondents mentioned cardiovascular complications. This comparison suggests that pausing the OA leads to more cardiovascular complications, although the cardiologic recommendation was respected previously. It is therefore crucial to ensure the indication of pausing the OA to achieve an optimal outcome for the patient.
Descazeaud and colleagues state a significantly higher rate of blood clots and late hematuria while using TURP, with a greater need of blood transfusions of the patients on continued OA. 13 These data are confirmed in another study, in which Michielsen and colleagues show a clot retention with a rehospitalization rate of 14.2% in patients on OA compared with 5.9% in patients without OA. 14
The use of the GreenLight laser has shown the lowest rates of bleeding incidences and blood transfusion rates in the literature among all laser devices for BPO. In several studies, the GreenLight laser has been proven to be an effective alternative to conventional TURP in patients on ongoing OA. Due to the tissue penetration depth of the GreenLight laser, the hemostatic properties of the photoselective vaporization technique turn out to be more effective compared with other techniques. 15 These findings correspond to our study, in which the most frequently applied technique was the vaporization of the prostate (39%) followed by conventional TURP (35%). The technique of enucleation using the holmium or thulium laser was preferred less often with 12% each.
Only one study showed significant differences between the blood transfusion rate (1.8%) and required reoperation (0.6%) due to secondary bleeding in the group of continuous OA. 16 Most studies did not find any difference between either groups. 12,17,18 In the study of Woo and Hossack, no patient required blood transfusions. Furthermore, they stated a prolonged catheterization time because of postoperative bleeding in 4.7% of the patients. 19 Macchione and colleagues assessed the efficacy of prostate vaporesection using the thulium laser. They did not observe any differences in operation time, hospitalization rate, or days until removal of the catheter comparing two groups, while continuing and pausing the OA 10 days before surgery. 9 These data do not confirm our findings of the survey, where the catheter was removed in 76% within the first 2 days in patients without OA compared with 42.5% of the patients with continuous OA. After literature research and assessing our findings of the survey, the GreenLight laser can be seen as an effective and safe treatment option for patients on ongoing OA. 20,21
In our survey, 12% of the urologists preferred holmium enucleation of the prostate (HoLEP) as the TT of choice in patients on continued OA. Tyson and Lerner compared two groups, in which 50% of the patients were either treated with aspirin or coumarin. They could not reveal any differences between the groups with regard to the blood transfusion rate (0% vs 0%). 22 Most studies state transfusion rates up to 8.4%, which corresponds to our results. 10,23 Only 7% of the urologists estimated a transfusion rate ≥10%. Another corresponding aspect was the hospitalization rate after TT of BPO: patients with ongoing OA were commonly hospitalized for 3 days in average, whereas the patients without OA usually left the hospital after 1 or 2 days. 10
Thulium laser is also used by 12% of the participants with similar results as HoLEP with blood transfusions up to 7.1%. 11,24 The study group of Netsch and colleagues showed further complications such as urinary retention, urinary tract infections, and secondary bleedings after thulium VapoEnucleation of the prostate (ThuVEP) in patients on OA. 11 These complication rates were similar to other studies and techniques used for TT of BPO.
A current review of the American Urological Association (AUA) demonstrates the need for cardiologic consultation before stopping OA. For operations with high risk of bleeding such as TT of BPO, a cardiologist should be informed. Due to these findings, TT of BPO with established laser devices (holmium, thulium, GreenLight) should become first-line therapy due to lower incidences of bleeding compared with conventional TURP. 25 Despite the surgeon's experience, it should be emphasized that TURP is one of the procedures with a high risk of bleeding and hemorrhage. 26
Conclusion
TT of BPO is commonly conducted in patients on ongoing OA. Although the current guidelines only recommend the use of the GreenLight laser on OA, the thulium, holmium, and the diode laser are also used.
Despite the low evidence, conventional TURP is performed on ongoing OA all over the world. The incidence of perioperative complications under TT of BPO on ongoing OA is lower than previously assumed. Cardiovascular complications might appear under TT of BPO, although OA is continued.
Footnotes
Author Disclosure Statement
No competing financial interests exist.