
Abstract
Objectives:
Registry-based clinical research in nephrolithiasis is critical to advancing quality in urinary stone disease management and ultimately reducing stone recurrence. A need exists to develop Health Insurance Portability and Accountability Act (HIPAA)-compliant registries that comprise integrated electronic health record (EHR) data using prospectively defined variables. An EHR-based standardized patient database—the Registry for Stones of the Kidney and Ureter (ReSKU™)—was developed, and herein we describe our implementation outcomes.
Materials and Methods:
Interviews with academic and community endourologists in the United States, Canada, China, and Japan identified demographic, intraoperative, and perioperative variables to populate our registry. Variables were incorporated into a HIPAA-compliant Research Electronic Data Capture database linked to text prompts and registration data within the Epic EHR platform. Specific data collection instruments supporting New patient, Surgery, Postoperative, and Follow-up clinical encounters were created within Epic to facilitate automated data extraction into ReSKU.
Results:
The number of variables within each instrument includes the following: New patient—60, Surgery—80, Postoperative—64, and Follow-up—64. With manual data entry, the mean times to complete each of the clinic-based instruments were (minutes) as follows: New patient—12.06 ± 2.30, Postoperative—7.18 ± 1.02, and Follow-up—8.10 ± 0.58. These times were significantly reduced with the use of ReSKU structured clinic note templates to the following: New patient—4.09 ± 1.73, Postoperative—1.41 ± 0.41, and Follow-up—0.79 ± 0.38. With automated data extraction from Epic, manual entry is obviated.
Conclusions:
ReSKU is a longitudinal prospective nephrolithiasis registry that integrates EHR data, lowering the barriers to performing high quality clinical research and quality outcome assessments in urinary stone disease.
Introduction
H
Data entry for traditional registries is time-consuming and labor intensive. We hypothesized that by designing a registry tied to an electronic health record (EHR), we could significantly decrease the time of data extraction. Our goal was to design the Registry for Stones of the Kidney and Ureter (ReSKU™) as a longitudinal, observational prospective registry of patients with urinary stone disease to address the limitations of traditional registries. To do so, inpatient and outpatient data in all phases of care would be extracted from the EHR prospectively in an automated manner and then organized in a secure, web-based application portal designed to support data capture for research studies. This approach will improve the quality of care for patients with urinary stone disease by prospectively tracking data regarding patient characteristics, surgical outcomes, follow-up management, and stone recurrence. One primary aim for ReSKU is to lower the barriers to participating in and maintaining a registry for urinary stone patients for any practice setting. In this study, we describe the design approach and initial experience with building and implementing ReSKU.
Materials and Methods
Evaluation of registry options
In developing ReSKU, it was important to first recognize how current registries operate and how an ideal modern registry would compare since traditional registry design and data entry are accompanied by challenges that hinder their implementation. These include labor-intensive data entry, cost of registry maintenance, patient confidentiality with meeting Health Insurance Portability and Accountability Act (HIPAA) requirements and human subjects research regulations, manpower for maintaining and organizing a database, concerns for how data will be stored and used, and interference with day to day clinical care 3 –6 (Table 1).
EHR = electronic health record; HIPAA = Health Insurance Portability and Accountability Act; REDCap = Research Electronic Data Capture.
A modern registry should ideally be easy to populate through integration with existing EHR systems and have a low maintenance cost, all while recording accurate, detailed patient clinical information, documenting surgeon outcomes, and tracking quality of care. 7 By leveraging the EHR, many of the challenges facing patient registries can be overcome.
Secondarily, the EHR would ideally be coupled with a data warehouse to allow information to be extracted from the EHR and housed securely in an easily accessible manner. For ReSKU, we elected to utilize a Research Electronic Data Capture (REDCap) database. REDCap is a mature, HIPAA-compliant, secure web application for building and managing online surveys and databases. It provides the following: (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources. 8 The Epic platform (Verona, WI) was the initial system selected to build the EHR tools for ReSKU, given that it has consistently had the largest market share of any EHR vendor. 9 These two software systems were selected as they are widely utilized in the medical and research communities and contain native features that make integration readily achievable. 10
Selecting measures to collect for the ReSKU study
The determinants of patient-centered outcomes were broadly conceptualized, relying on both urologist practice patterns and the existing literature to build a framework of variables for collection. To maximize the validity, reproducibility, and quantitative nature of the data collected, current AUA and European Association of Urology guidelines for urolithiasis management were referenced. 11 –13 Where possible, validated clinical instruments, including American Society of Anesthesiologists score, 14 Clavien–Dindo score, 15 and modified Guy's stone score, 16 were integrated. Variables were divided into broad categories: sociodemographic characteristics, clinical and biometric characteristics, stone characteristics, operative factors, process characteristics, and outcomes. The next design phase focused on feasible implementation of ReSKU into daily clinical practice.
While the ideal prospective observational registry would record all potential stone-related determinants of health, this approach is impractical given the time constraints intrinsic to clinical visits. Therefore, we narrowed the measures to be collected down to the most critical variables that could be feasibly gathered in the usual course of clinical care. After a comprehensive list of measures was constructed, we performed collaborative interviews of 11 academic and community endourologists based in the United States, Canada, China, and Japan to determine which of these clinical variables to collect. This resulted in a condensed set of variables for inclusion in the ReSKU database, separated into instruments specific to each patient encounter (Table 2). The registry design process evolved over the course of 1 year, involving multiple rounds of data instrument pretesting and revision. Particular attention was paid to structuring variables into queries that could be collected in the course of routine patient care with minimal disruption to the clinical encounter. Pretesting included piloting data collection at two medical centers with assessment of compliance for accuracy of data collection.

Data points listed demonstrate conceptualizing the determinants of stone patient outcomes. Included variables in bold are readily collected as part of each patient clinical encounter.
ASA = American Society of Anesthesiologists; BMP = Basic metabolic panel; ReSKU™ = Registry for Stones of the Kidney and Ureter.
Patient selection
After obtaining appropriate institutional review board (IRB) approval, all patients of any age presenting to the urology clinic for evaluation of stone disease who had clinical evidence of nephrolithiasis were included. Clinical evidence of nephrolithiasis was defined as any upper tract urinary stone demonstrated by imaging performed within the 12 months before clinic presentation or adjudicated passage (i.e., the patient brought their stone to their clinic visit). Patients were included into the registry after providing informed consent for participation. No patients who met these inclusion criteria were excluded from participation in ReSKU.
Results
ReSKU registry variables were incorporated into the REDCap database by dividing all of the variables into four specific data collection instruments to parallel patient encounters: New Outpatient, Surgery, Postoperative, and Follow-Up visits (Table 2). Instruments were structured in a patient-centered manner by following the patient's phases of care. An encounter is created each time the patient is seen. Within the EHR, clinical note templates related to each encounter were created: “New patient history and physical,” “Operative report,” “Postoperative progress note,” and “Follow-up progress note.” Within each template, dropdown lists were created for each of the registry variables. Using these dropdown lists facilitates storing note data in a structured format, which allows information extraction directly into the registry database, thereby bypassing manual data entry (Fig. 1). During the pilot phase, compliance with accurate coding of clinical encounters into each of the note templates was assessed by three urologists independently, and where variables were perceived as possibly introducing uncertainty into coding accuracy, templates were adjusted to meet agreement between the three adjudicating urologists.
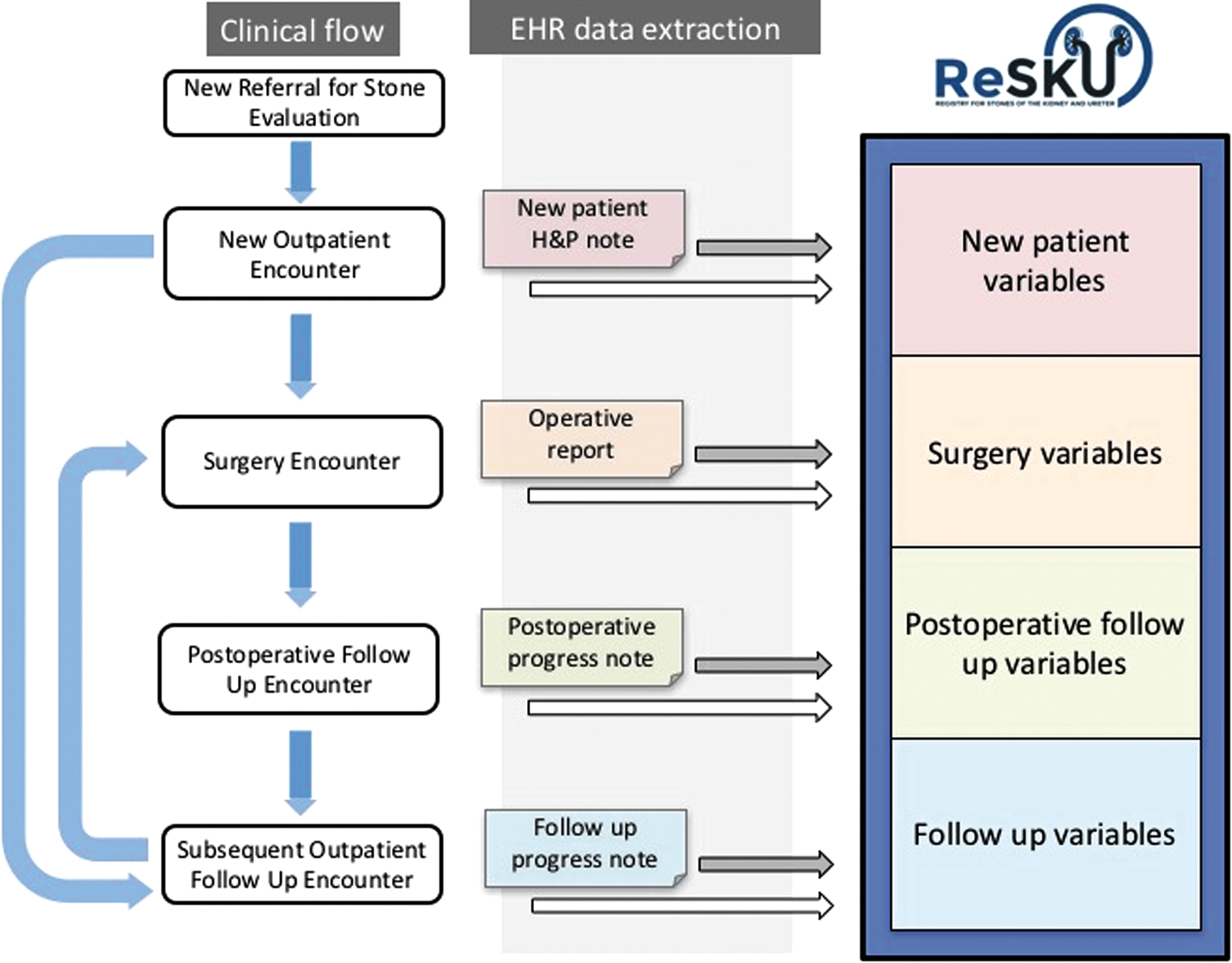
ReSKU™ database structure is based on clinical flow for patient care. Light blue arrows indicate clinical flow. White boxes represent the type of patient encounter. The light gray box represents the EHR. Under “EHR data extraction,” the colored boxes indicate structured clinical note templates with dropdown lists of variables for data capture. The arrows portray how automated data integration occurs within ReSKU™. The white arrows delineate discrete data extraction from the EHR into ReSKU™ (e.g., laboratories and vital signs). The gray arrows represent data (e.g., stone symptoms and stone size) extracted from dropdown list selections within the EHR clinic note templates. Under “ReSKU,” the blue box represents the collection and storage of data into different variable categories using REDCap. EHR, electronic health record; REDCap = Research Electronic Data Capture; ReSKU™, Registry for Stones of the Kidney and Ureter.
A total of 268 variables across all encounter types were implemented in ReSKU, with 60 New Patient, 80 Surgery, 64 Postoperative follow-up, and 64 Follow-up variables. Using conventional registry data population (i.e., a research assistant abstracting data from the provider's clinical note into ReSKU), manual data entry into REDCap required 12.06 ± 2.3 minutes for New patient, 7.18 ± 1.02 minutes for Postoperative follow-up, and 8.10 ± 0.58 minutes for subsequent follow-up clinical encounters. By using ReSKU structured clinical note templates in Epic to document each encounter, the manual data entry times decreased to 4.09 ± 1.73 minutes for New patients, 1.41 ± 0.41 minute for Postoperative follow-up, and 0.79 ± 0.38 minute for subsequent Follow-up patients, respectively. With full EHR integration, use of ReSKU templates to document clinic encounters facilitated automated data extraction, and no added manual data entry time was required (Table 3).
Manual extraction from conventional unstructured clinic notes (third row) compared with manual extraction from ReSKU™ Epic clinic note templates (fourth row), and lastly implementation of ReSKU™ Epic clinic note templates along with automated data abstraction (fifth row). p-Values were calculated with unpaired Student's t-test using Stata 14.1 (StataCorp, College Station, TX).
Discussion
Clinical research in nephrolithiasis most often relies on retrospective clinical data collection. 17 The resultant quality of studies is dependent on the thoroughness of retrospective chart review, accuracy of visit coding, and accuracy of patient records. Prospective high quality registries linked to clinical outcomes are critical for forward progress in understanding the natural history of kidney stones.
Some prospective registries exist in urinary stone disease, but differ from ReSKU in that they are limited to specific procedures, have limited follow-up, or include only patients with rare kidney stones. Examples include the Clinical Research Office of the Endourological Society percutaneous nephrolithotomy and ureteroscopy global registries, the Brushite Kidney Stone Registry, the Rare Kidney Stone Consortium registries, the Percutaneous Nephrolithotomy Registry, the Health-Related Quality of Life in Rare Kidney Stone Registry, and the Vietnam Era Twin Registry. 18 –21 By design, each of these registries has a narrow focus with the intention of bringing attention to particular stone types or interventions. The aim of ReSKU is to capture the larger scope of stone disease burden across all stone types in order for study results to be more generalizable to a broader population of nephrolithiasis patients.
ReSKU's approach is unique in that it captures longitudinal clinical data already being collected by providers during the course of a patient encounter. The ReSKU data collection instruments were designed based on current stone management guidelines, quality care metrics, and endourologist interviews to identify the data points that any provider ought to be asking patients at each clinic visit. By tapping into the power of EHRs, ReSKU eliminates the burden of data entry, making prospective comprehensive inpatient and outpatient data collection on all stone patients a sustainable endeavor.
ReSKU's automated data extraction process drives several key advantages compared with traditional registries that rely on manual data entry. Since manual entry often relies on a research assistant or third party interpreting the provider's clinical notes to extract data, human data entry problems such as typographic errors and variable definition interpretation errors are common. These databases require significant time to rid the data set of erroneous entries. In contrast, ReSKU minimizes these errors since templates are populated by consistent dropdown menus. Moreover, the urologist is the one performing data collection directly into the clinic note, which then populates the data registry. Since the provider is best positioned to understand the patient's clinical status, registry data quality can be expected to be at least as good as the data collected for clinical care. In addition, data collection instruments in both clinic and operative note templates were designed with clinical care as well as billing charge capture in mind. This allows ReSKU to reflect real world practice with minimal impact on provider documentation time.
Understanding that different practices will have their own set of time and available resources, ReSKU was designed so that providers can participate at different levels of data integration. While the optimum implementation of ReSKU includes full integration with the EHR for automated data capture, this is not the only available option. Based on experience with piloting ReSKU in medical centers without an EHR in place, implementation can still yield excellent data quality results with designated, trained research team members to collect and upload clinical data directly into REDCap (Table 3, row 1). REDCap data capture has been proven to be a robust way to manage instrument design and secure data collection across institutions. 8 For practices with an EHR present but no infrastructure for automated data capture, ReSKU clinical templates can be built into the EHR and research team members can extract data from the template note into REDCap (Table 3, row 2). As seen by our results, the use of templates significantly reduced data entry time into REDCap. Therefore, any clinical provider who is interested in implementing ReSKU at their institution can do so. ReSKU's implementation strategy is flexible in that it can be modified for different practice settings to account for unique EHR environments and personnel.
Additional benefits of ReSKU will be realized with future clinical and translational research. As a longitudinal, prospective observational registry, ReSKU was designed to reveal patterns in clinical outcomes and practice as well as quality outcomes. However, once data collection is implemented into a provider's daily routine, clinical information will be continuously collected and managed in a HIPAA- and IRB-compliant manner. Such demographic and generalized nephrolithiasis-related clinical data provide a baseline framework on which to layer additional IRB-approved clinical studies. As new clinical and translational research questions arise surrounding validation of biomarkers, clinical endpoints, and technologies over time, ReSKU data can support project aims without the need for additional retrospective data extraction. For example, patients could be randomized into different groups for an interventional study. New data collection instruments can be easily integrated so that only specific data points related to the randomized trial need to be collected in addition to ReSKU data, thereby decreasing the amount of work needed to complete the clinical study. This could be performed on a single- or multi-institutional scale. By lowering the resources needed to effectively complete clinical trials, ReSKU can expand data collection networks and lower the cost of multicenter trials.
While ReSKU has several advantages over traditional registries, it is not without its own associated challenges. For automated data extraction to be implemented, an upfront investment is required for programming both structured data capture into clinical notes and data extraction from the EHR. Collaboration between the urologist and data analysts at each site is essential to optimize the quality of the data being extracted and verify that the captured data points correspond to the desired data. Meanwhile, ReSKU is also limited in that long-term data collection may be limited by patients lost to follow-up. This is an inherent limitation given ReSKU's infrastructure and reflects the nature of registry studies in general. In addition, ReSKU was designed to integrate with Epic, given its marketshare and relatively widespread use in the United States. This integration relies on tools built specifically for the Epic EMR system. To broaden its applicability to other EMR systems, both within the United States as well as globally, these tools could be adapted for automated data extraction in non-Epic environments. However, in its current state, ReSKU is designed for use with Epic as a data source.
Finally, in the current ethos of the Affordable Care Act and accountability for quality and healthcare value, ReSKU may also be of practical value for providers. EHRs, as mandated by the American Reinvestment and Recovery Act in 2009, provide an opportunity to automate aspects of data entry that were previously accomplished only through labor-intensive chart review and manual data entry. 6 Participation in the Physician Quality Reporting System (PQRS) through qualified clinical data registries (QCDR) can help providers maintain compliance with Medicare and Medicaid Services requirements. 22 Responding to increasing pressure from the federal government and private insurers to report on quality and to meet PQRS reporting, the AUA has led efforts to launch nationwide clinical data registries with the AQUA Registry. Initial efforts for AQUA have focused on urologic oncology, highlighting the importance of physician participation in registries for tracking of quality metrics. Continued AQUA efforts and registries such as ReSKU can help to reduce the burden of participation in QCDR and keep urologists aligned with Centers for Medicare & Medicaid Services mandates.
Conclusions
As a longitudinal, observational prospective registry of patients with urinary stone disease that automates data extraction from EHRs, the ReSKU and Ureter represent an evolution from traditional registries. ReSKU provides a research infrastructure that decreases the burdens of quality metric reporting and lowers the barriers to performing high quality clinical research for urolithiasis.
Footnotes
Acknowledgments
This study was supported by the NIH K12-DK-07-006 (TC), P20-DK-100863 (MLS and TC), and R21-DK-109433 (TC).
Author Disclosure Statement
No competing financial interests exist.