
Abstract
Objectives:
To perform a prospective study to evaluate the renal protective effects of ramping protocol and pause protocol for extracorporeal shockwave lithotripsy (SWL) in human subjects.
Patients and Methods:
Three hundred twenty patients with solitary renal stone <15 mm were randomized to receive one of four protocols: (1) 80% power from beginning until the end of treatment; (2) the first 100 shockwaves (SWs) at 40% power, and then 80% power until the end of treatment; (3) the first 100 shocks at 40% power, followed by a 3-minute pause, and then further SWs at 80% power until the end of treatment; and (4) the first 100 shocks at 80% power, followed by a 3-minute pause, and then further SWs at 80% power until the end of treatment. The primary endpoint was the incidence of renal hematoma assessed by imaging on day 2. Spot urine samples were also collected before and after treatment for acute renal injury marker measurement.
Results:
The baseline information and treatment parameters of the four groups were comparable. The overall incidence of hematoma formation was 7.69% (24 patients). The number of patients developing hematoma in the four groups was 8 (10.26%), 7 (8.97%), 6 (7.59%), and 3 (3.90%), respectively, and the incidence of hematoma among the four groups was not significantly different. Only patient's body mass index and mean blood pressure during treatment were predictors for hematoma formation. There was also no significant difference in changes in the levels of all markers and complication and hospitalization rates between the four groups.
Conclusion:
Comprehensive assessment of clinical parameters, imaging results, and urinary markers showed no obvious improvement in post-SWL renal insult by either protocol.
Introduction
A
Later, Connors et al. performed another set of experiments to determine whether a pause during power ramping might help to protect against SWL-induced renal injury. 4 The size of vascular lesions formed after standard treatment (2000 SWs, 24 kV) and ramping protocols (first receiving 100 SWs at either 18 or 24 kV, followed by a 3- to 4-minute pause, and then 2000 SWs at 24 kV) was compared. For porcine kidneys treated with the standard clinical treatment, the mean vascular lesion size was 1.29% functional renal volume (FRV). However, the mean lesion sizes for the two ramping groups were both about 0.01% FRV. These data suggest that a short pause after the first 100 SWs is important for renal protection, and the initial voltage used for the first 100 SWs does not correlate with renal damage, as the lesions produced by either a low or high starting voltage were of similar size. They also suspected that the advantage shown by the ramping protocol might actually be attributed to the effect of a short pause during the readjustment of voltage and targeting during voltage ramping.
However, there are currently no clinical data to confirm these animal data, and discrepancies between animal and clinical data can occur. 5,6 Therefore, we carried out a prospective clinical study to assess the effect of these treatment protocols, the ramping protocol and the pause protocol, on renal injury and complication rates during SWL for renal stones. As it was impossible to assess the histological changes in human subjects after SWL, we decided to use a panel of assessment, including clinical, imaging, and laboratory tests, for the assessment of adverse effects of SWL.
Patients and Methods
This was a prospective randomized study to assess the effects of the low-energy SW pretreatment and pause protection protocols on the degree of renal injury in patients with renal stones receiving SWL. The study involved 320 subjects receiving SWL at a single center from January 2011 to July 2013. The study was approved by the local institutional ethics review board and conducted in accordance with good clinical practice guidelines and the Declaration of Helsinki. The clinical trial registration was ChiCTR-TRC-10001134.
Participants
The study subjects were patients diagnosed with having renal stones and scheduled for primary SWL in our unit. The inclusion criteria were adult patients (aged ≥18 years) with a solitary radiopaque stone less ≤15 mm and who were scheduled for SWL.
As the objective of this study was to assess the effects of different treatment protocols on renal injury, any patient with an increased risk of hematoma formation and renal scarring was excluded. Therefore, we did not include patients with known bleeding tendency, positive urine culture, or uncontrolled hypertension during SWL, whose risk of hematoma formation would be higher. 7 Patients with previous major procedures to the same kidney, chronic renal impairment (defined as a serum creatinine level 1.5 times the upper limit of normal), or having previously undergone more than two SWL sessions were excluded from the study due to the potential risk of an increased likelihood of renal fibrosis. Patients with ureteral stent or nephrostomy tube in situ were also excluded. Finally, patients with SWL, nephrostomy tube insertion, or history of ureteral stenting within 90 days of the current SWL procedure were excluded to avoid the carry-on effect of the abovementioned procedures on acute renal injury markers.
Intervention protocols
After informed consent had been obtained from all patients, their background information was collected. Spot urine (50 mL) was collected one day before SWL for the measurement of baseline levels of urine markers. All patients received treatment with an electroconductive lithotripter (Sonolith Vision; Edap-Technomed, France) in our center. The maximal power recommended by the manufacturer for renal stone treatment was the 80% energy level (14.5 kV). The basic acoustic parameters for the generator according to International Electronic Commission (IEC) 61846 standard are listed in Table 1. Patients were then randomized to receive one of the four treatment protocols (Fig. 1). The four treatment protocols were follows:
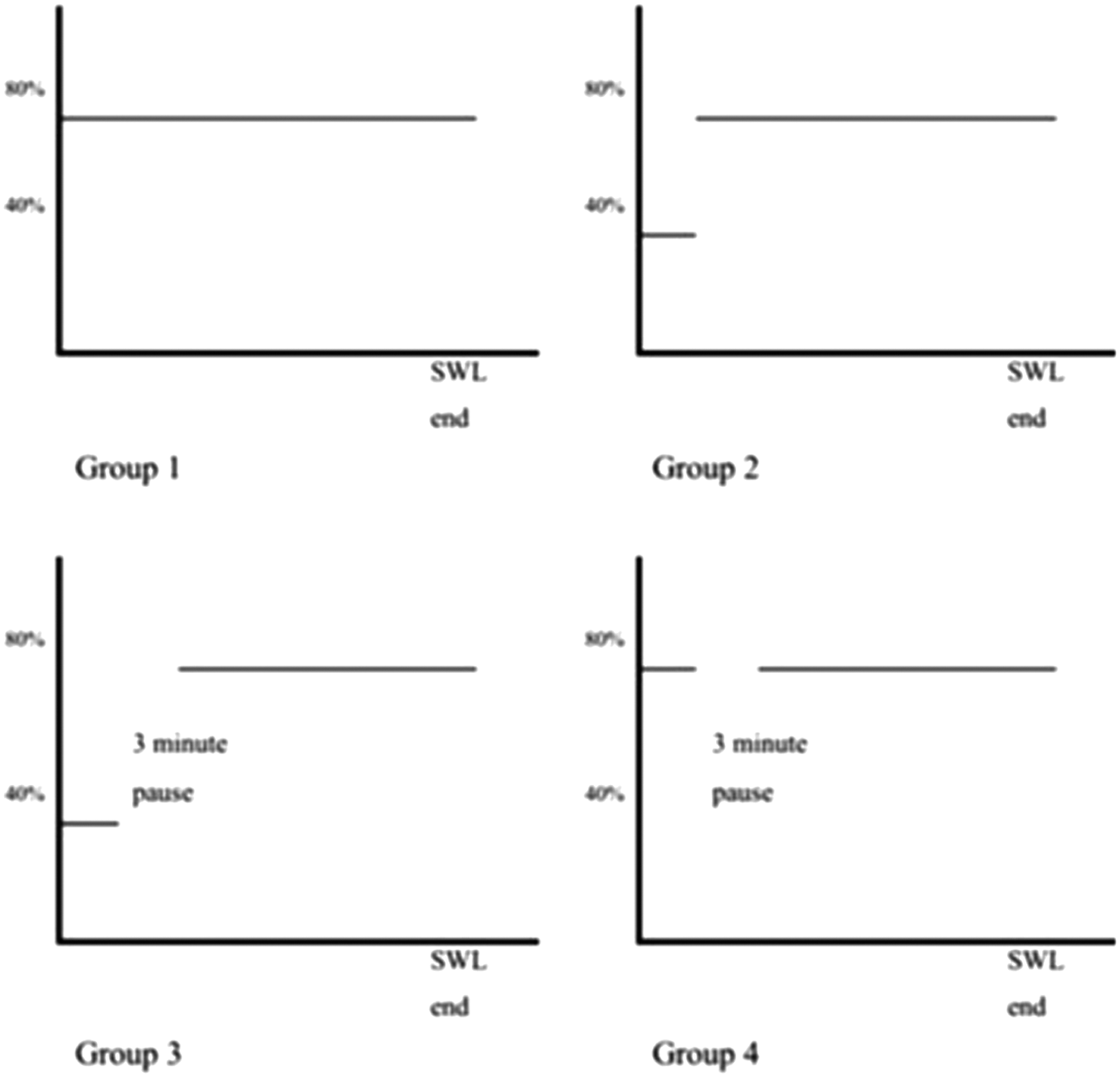
Graphical presentation of the four treatment protocols.
This was the information related to IEC61846 standard and was not related to the power setting (40% and 80%) used in the study.
Group 1: Patients would receive 80% power (14.5 kV) comprising 20 SWs from the beginning to the end of treatment (control).
Group 2: Patients would receive the first 100 shocks at 40% power (9.2 kV), followed by SWs at 80% power until the end of treatment (ramping protocol).
Group 3: Patients would receive 100 shocks at 40% power, followed by a 3-minute pause, and then further SWs at 80% power until the end of treatment (ramping and pause protocol).
Group 4: Patients would receive 100 shocks at 80% power, followed by a 3-minute pause, and then further SWs at 80% power until the end of treatment (pause protocol).
All power ramping, that is, increasing the power from 40% to 80%, was done within 20 SWs. All patient treatments were designed to administer a maximum energy of 1000 energy units (as recommended by the manufacturer) 8,9 unless the stone had become difficult to be localized or the patient could not tolerate the procedure, either due to pain or to physical conditions such as hypertension or bradycardia. The stone was localized and regularly monitored during the whole treatment by fluoroscopy. For all treatments, SW was delivered at a rate of 2 Hz. Vital signs were monitored regularly during the entire procedure. Patients received one dose of 0.5 mg alfentanil at the beginning of the study unless they refused. If they experienced pain during treatment, an additional 0.5 mg alfentanil was given.
At the end of treatment, the total number of shocks and energy received, duration of the treatment, total amount of analgesics consumed, and pain score at the end of treatment (by pain intensity verbal rating scale tool) were recorded. Immediately after treatment, a 50-mL spot urine sample was collected for the measurement of post-treatment urine markers.
Further follow-up was performed on postprocedure day 2, at week 6, and week 12 unless the patients received other additional treatment for the stone. During each follow-up examination, any symptoms and complications occurring after SWL were asked about and recorded. Spot urine samples were collected for monitoring of urine markers. Plain radiography was performed during follow-up to assess treatment outcome.
Cross-sectional renal imaging was performed on day 2 in all patients for the assessment of possible perirenal and intrarenal hematoma. For those patients with no contraindications for magnetic resonance imaging (MRI), MRI was performed in a 3T scanner (Philips Achieva 3.0T, X series, Quasar Dual MRI System; Philips Medical Systems, Best, The Netherlands). Standard T1-weighted, T2-weighted, and gradient-echo sequences (sensitive to blood products) were performed in both the axial and coronal planes of the kidneys. The following features were specifically looked for: (1) subcapsular hemorrhage, (2) hemorrhage into a renal cyst, (3) perirenal fluid collection, and (4) loss of corticomedullary demarcation in cases of diffuse renal parenchymal injury. For those patients with contraindications for MRI, noncontrast computed tomography (NCCT) was performed as an alternative imaging assessment. We expected MRI or CT scan would provide more operator-independent assessment of the renal injury than ultrasound assessment. Two radiologists blinded to the clinical information reviewed all of the images. The incidence of renal hematoma for each group was then compared.
A panel of urine markers were also measured for the assessment of renal injury and renal fibrosis. As previously mentioned, spot urine samples were collected before and immediately after SWL. During follow-up, patients were also required to collect a random urine sample between 6 a.m. and 9 a.m. excluding their first void after sleep. Markers used for the assessment of acute renal injury included N-acetyl-β-
Outcome assessment
The main outcome assessed in the study was SWL-related injury to patients. The primary outcome was the incidence of renal hematoma developed after SWL and was defined as the presence of renal hematoma (perirenal and intrarenal) after one session of lithotripsy, as assessed by MRI or NCCT performed on day 2 after SWL.
Secondary outcomes included changes in urine markers for acute kidney injury after SWL. Incidences of unplanned hospital visits and complications within 30 days after SWL, and considered to be related to the treatment, were recorded, and complications were graded according to the Dindo-Clavien system. 16 The pain score at the end of treatment and analgesic usage were also assessed.
Sample size estimation
Three hundred twenty patients were recruited for this study, with 80 assigned to each arm. Calculation of the sample size was based on the data from previous studies on the incidence of post-SWL hematoma by assuming the incidence of hematoma after SWL to be about 35% 17 –19 and the modified treatment protocols to be able to reduce the incidence to 15%, a 60% reduction in hematoma incidence based on the animal data from Willis et al. 20 With these assumptions, it was estimated that at least 80 patients would be needed for each arm to provide a power of 80% with a significance level of 5% and a dropout rate of 10%.
Randomization process
An independent staff statistician using the permuted block design with random block sizes of 4, 8, and 12 generated the randomization list with the aid of a computer program before the commencement of recruitment. The random allocation sequence was then placed in identical preset numbered envelopes. Before commencement of SWL, a duty urologist performed the randomization by opening the consecutively numbered, identical preset envelopes after confirming the eligibility of the subject and the stone site.
Blinding
A designated team of urologists and radiologists who were unaware of the treatment assignment managed the follow-up of the patients, including imaging assessment. The research staff member involved in laboratory measurement of the urine markers was also blinded to the intervention assigned to each patient in the study. Treatment allocations were known only by the independent statistician, who was only involved in preparation of the randomization list and data analysis and was not involved in data collection or direct patient care.
Data treatment and statistical analyses
All analyses were performed with SPSS version 23.0 (Chicago, IL). Treatment outcomes were analyzed using an intention-to-treat approach. Baseline and treatment parameters were compared using one-way ANOVA for continuous variables and chi-square test or Fisher's exact test for categorical variables, where appropriate. The incidence of renal hematoma developed after SWL by the different protocols was compared by logistic regression, with the consideration of other potential factors of hematoma formation. Crude and adjusted odds ratios from the logistic regression models and their 95% confidence intervals (CIs) were reported. The changes in urine markers for acute kidney injury were assessed with repeated measures ANOVA. A two-sided p-value <0.05 was considered statistically significant.
Results
From January 2011 to July 2013, 344 patients were eligible for this study; however, 10 patients declined entry into the study for personal reasons. Among the 334 patients consenting to the study, 14 patients were eventually excluded for various reasons: no stone was found in pre-SWL imaging (n = 7), the renal stone had dropped into the ureter (n = 4), and SWL was withheld due to medical reasons (n = 3). Eventually, 320 patients fulfilled all inclusion criteria and were then randomized into one of the four groups, with 80 patients in each group (Fig. 2).
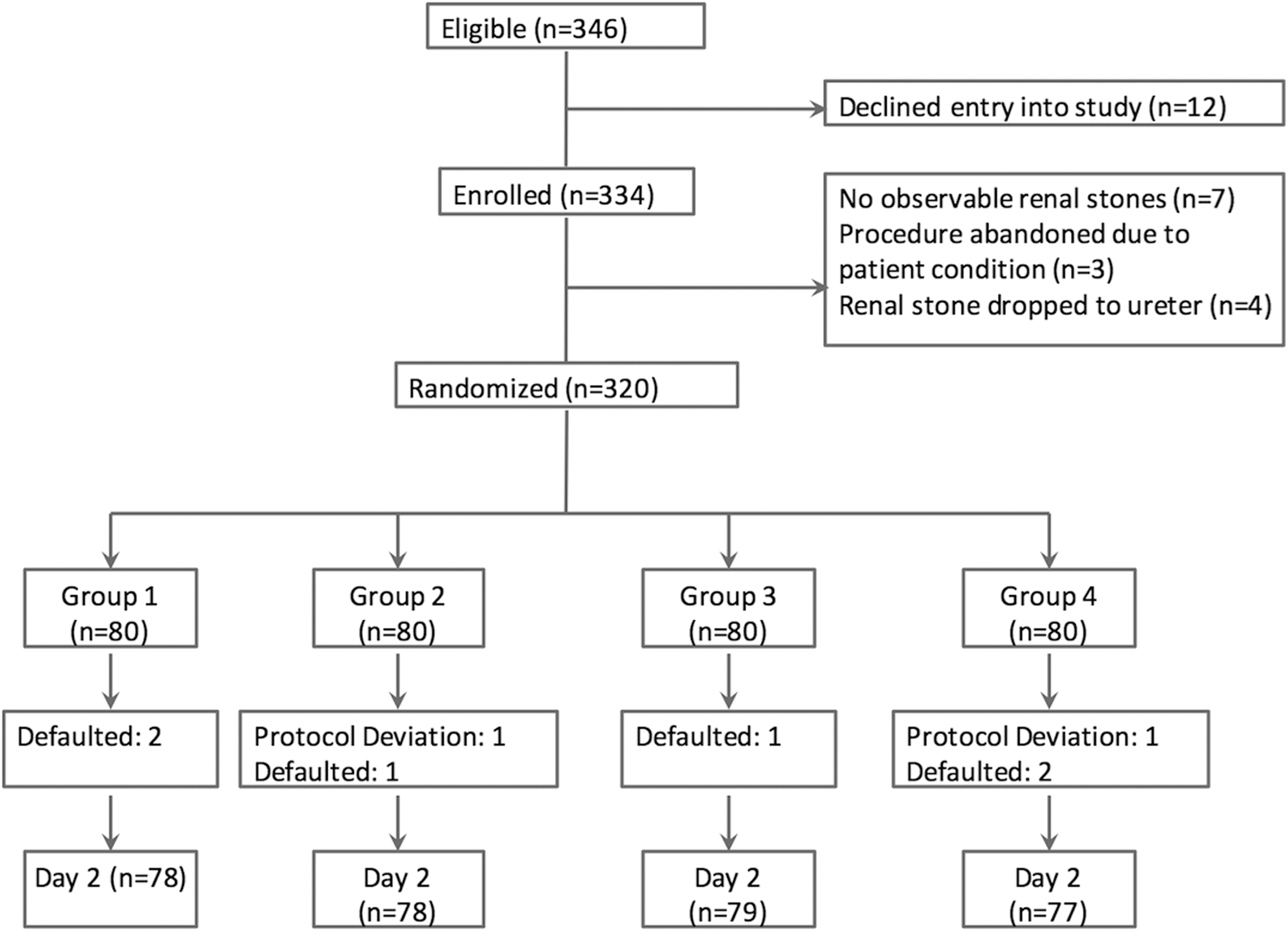
Flow diagram of the progress of patients through the study until day 2 (performance of imaging for renal hematoma assessment).
Patient clinical characteristics and stone parameters were comparable between the four groups (Table 2). Data on treatment parameters are also shown in Table 3. All patients were preplanned to receive the same maximum power (1000 energy units) for their treatment. However, two patients (one in Group 2 and one in Group 4) were excluded from the study due to protocol deviation because they both received 1400 energy unit during their treatment, which was 40% more than the protocol, which might affect the interpretation of renal injury and complications. Otherwise the treatment parameters of the four groups were comparable. All subsequent analyses were based on the remaining 318 patients. The average dose of alfentanil received by the recruited patients was 0.43 ± 0.22 mg, and no significant difference was observed between groups. Mean verbal pain score of patients during SWL in this study was 2.2 (0–10), indicating far from severe pain. The overall treatment rate, as defined as stone free or stone fragments less than 4 mm after one section of SWL, was 36.16%. There was no difference observed between the groups.
Data are shown as number and percent unless otherwise noted.
Chi-square test.
ANOVA test.
Fisher's exact test.
BMI = body mass index; SD = standard deviation.
Treatment success rate included patients either stone free or with renal fragments <4 mm.
ANOVA test.
Chi-square test.
For determination of the incidence of post-SWL hematoma, 6 patients declined the imaging assessment on day 2 after SWL, and thus 312 patients were available for assessment (Table 4). MRI and CT were performed in 197 (63.14%) patients, and CT scanning was performed in the remaining 115 (36.86%) due to contraindications for MRI. Hematoma was detected in 24 (7.69%) patients on day 2 imaging. Most of the hematomas (n = 20) detected were either subcapsular or perinephric, with three parenchymal hematomas and one bleeding in renal cyst detected. Eleven subcapsular hematomas were less than or equal to 10 mm in thickness and the remaining nine hematomas had thickness that ranged from 13 to 38 mm. For the three parenchymal hematomas, two were less than 10 mm and the other was 12 mm. The location and extent of these hematomas and their relationship to the original targeted stone site are listed in Supplementary Table S1 (Supplementary Data are available online at
Data are shown as number and percent.
Chi-square test.
Fisher's exact test.
MRI = magnetic resonance imaging.
DM = diabetes mellitus; MAP = average of mean arterial blood pressure at the beginning and the end of treatment.
Complications developed immediately after SWL in 12 (3.77%) patients (Table 4) and all were managed conservatively, with no inpatient management required (Grade 1). Unplanned hospital attendance related to SWL was made by 17 (5.35%) patients, with 6 (1.89%) patients requiring in-hospital care. Although the majority of the complications were Grade 1 or 2, one patient suffered from symptomatic perinephric hematoma leading to acute renal failure and required temporary hemodialysis (Grade 4a) (Table 6).
Urinary levels of the acute renal injury markers, NAG, MA, and IL-18, were significantly elevated after SWL (Fig. 3). The levels of both NAG and MA returned to baseline level on day 2 in Groups 3 and 4 (both included pause protocol), whereas those of Groups 1 and 2 remained significantly elevated compared with baseline level. The levels of both markers in all four groups had returned to baseline level by 6 weeks after treatment. The levels of IL-18 in all four groups returned to baseline level on day 2 after treatment. However, at all time points after treatment, there were no statistically significant differences between the levels of these three markers between the four treatment groups. In contrast, there was no significant change in the urinary levels of NGAL when compared with the baseline level in all four groups over the different time points after SWL.
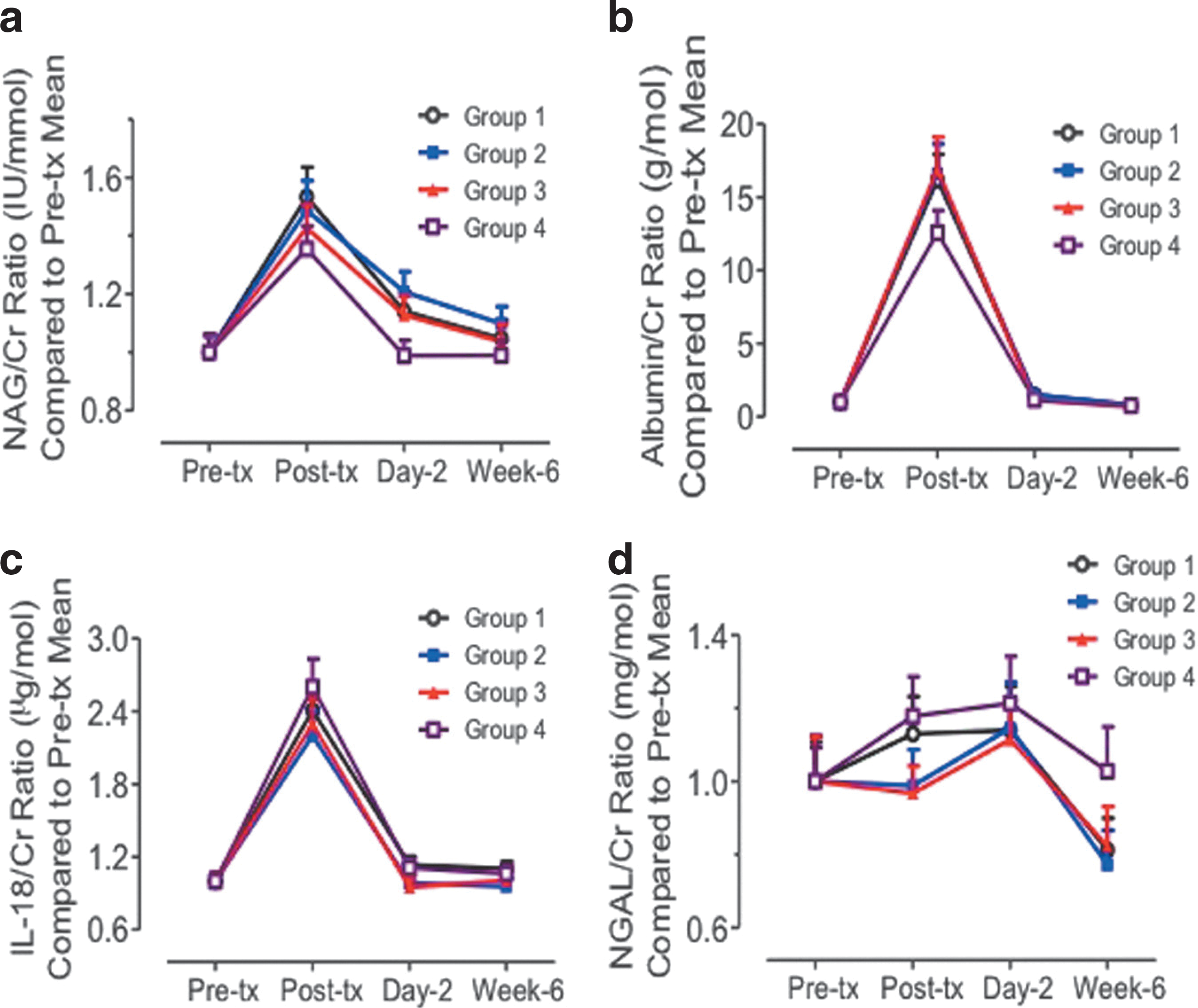
Change in urinary levels of acute renal injury markers during the treatment and follow-up periods.
Discussion
In this prospective randomized study of 320 patients receiving SWL, neither the ramping protocol nor the pause protocol led to significant decreases in the incidence of post-SWL hematoma. Furthermore, there were no significant differences in the incidences of acute complications and unplanned hospital attendance. The urinary levels of acute kidney injury markers were also similar between the groups.
The rapid growth in popularity of SWL during its early development was partly related to the perception that it was entirely safe. However, with the accumulation of clinical experience, it is now clear that SWL can cause various short- and long-term complications, relating in particular to the kidney. 1,21,22 Immediately after SWL, cellular damage and also vascular trauma secondary to small vessel damage occur. 1 Clinically, patients may develop hematuria and subcapsular and perinephric hematoma. Although the reported incidence of symptomatic renal hematoma is less than 1%, 7,18 imaging-detected renal hematomas are much more common, reportedly ranging around 30% to 40%. 17 –19
Many treatment protocols have been proposed to minimize renal injury based on animal studies. 2 –4 From these studies, ramping and pause protocols had shown to decrease the size of hemorrhagic lesions in the renal parenchyma. However, there were no clinical studies verifying these findings and also comparing the effects of these protocols. Therefore, we decided to carry out this study. As it was impossible to assess the histological changes in human subjects after SWL, we decided to use a comprehensive assessment of the effects of SWL on the subjects, including clinical, imaging, and laboratory assessments.
Our results did not show any statistically significant difference between the four patient groups in the incidence of renal hematoma formation. When comparing our study with the previous animal studies, there were some differences between them. In animal studies, size of hemorrhagic lesion in histology was used as their endpoint. We used the development of post-SWL hematoma, as detected by imaging (either MRI or CT), as our primary endpoint, which is the most sensitive clinical method to be applicable in human subjects. In our study, most hematomas detected were subcapsular and perinephric hematomas. This might be related to the relatively lower sensitivity of imaging modalities to detect intraparenchymal hemorrhagic lesions compared with histological diagnosis. The endpoints of our study were different from porcine studies, as we were studying the incidence of renal hematoma rather than the size of hematoma. As a result, it might be difficult to directly compare our results with those findings from porcine models. 2,3 Last, in our opinion, either hematoma size or incidence could only provide a cross-sectional assessment of renal injury at one time point, with uncertain overall clinical significance. We believed that the inclusion of other assessments, such as serial monitoring of renal injury markers and also clinical parameters (such as other complications and unplanned hospital admissions), would provide a more comprehensive and clinically relevant overview of the role of these treatment protocols.
The overall incidence of hematomas formed was only 7.69%, and the incidence of symptomatic hematomas was 1.3% (four patients), similar to those of other clinical reports. 7,18 Multivariate analysis showed that higher BMI and also higher mean blood pressure during treatment were the only two predictors for imaging-detected hematoma formation. From the literatures, patients with known hypertension, in particular with unsatisfactory control, had increased risk of developing post-SWL hematoma. 7,23,24 Obesity was also identified as a risk factor for hematoma formation. 23,24 The exact mechanism for obesity and hematoma formation was unknown. However, it was proposed that the increased risk of atherosclerosis in these patients, which leads to decrease in vascular tensile strength, might account for the increased risk of post-SWL hematoma formation. 23,24
Urinary markers have frequently been used for the assessment of renal injury in various clinical situations and can provide earlier and more sensitive detection of renal injury, with good correlation to clinical outcomes. 10 We used a panel of markers to assess post-SWL renal injury as in other studies. NAG and MA are traditional markers used in the assessment of SWL injury, and IL-18 and NGAL are newer markers shown to be useful for assessing acute renal injury, including that by SWL. The urinary levels of NAG, MA, and IL-18 were significantly increased immediately after SWL and then decreased on day 2. Although there were no significant differences between the levels of urinary acute kidney injury markers between the four groups, the use of the pause protocol resulted in earlier return of urinary NAG and MA to baseline level on post-SWL day 2. However, all markers returned to baseline levels at week 6 after SWL, and so the clinical significance for earlier return of marker levels to baseline in patients treated by pause protocol was uncertain.
Furthermore, there was also no significant difference in other clinical parameters, such as patient analgesic demand, immediate post-SWL complications, unplanned hospital attendance, and incidence of worsening blood pressure control between the four groups. The overall complication rate was 9.12% (29 patients) and except for one patient, all complications were mild (Clavien Grade I and II), with no long-term consequences. Therefore, the two protocols did not appear to lead to any significant difference in the clinical endpoints after SWL when compared with the controls.
Notwithstanding the importance of its findings, there are some limitations to our study. In our initial sample size calculation, we assumed the incidence of renal hematoma in the control arm to be around 35% based on our own data and previous reports. 17 –19 However, the overall incidence of hematoma in the study was only 7.69%. We do not know the reason for this relatively lower incidence of imaging-detected hematoma in our series. The lithotripter involved in this study was an electroconductive lithotripter, which was a modified type of electrohydraulic lithotripter with a more precise focal zone and lower peak pressure than the HM3 lithotripter used in most of the reference literature on hematomas. 17,25 This might be a partial reason for the lower incidence of hematomas detected in our series. As a result, our sample size might not have enough power to detect the actual effect of the two protocols on the formation of renal hematomas. For example, there seemed to be a trend suggesting a difference in the incidence of hematoma in Group 1 (standard protocol, 10.26%) and Group 4 (pause protocol, 3.9%), although it was not statistically significant. If we also take into account the earlier recovery of urinary NAG and MA level on day 2, pause protocol might have some benefit in protecting the kidney during SWL, as suggested from animal studies. Nevertheless, if we also take into consideration the overall data, including other clinical and laboratory endpoints, in these 320 patients, the clinical effect of the two protocols on renal protection might be less substantial than those suggested in porcine models. Further large-scale studies, preferably multicenter trials, may help to verify our results.
We did not include treatment outcome as an endpoint because the main aim of the study was to assess the effect of different protocols on the complications and side effects related to SWL. Therefore, we included treatment of some residual stones (about 43.5% of all stones treated in this study) after other treatments, such as previous SWL. Moreover, a relatively higher proportion of patients in the cohort (more than 50%) had lower caliceal stones, which are well known to have lower stone clearance. Hence, the treatment success might be lower due to these factors. Again, further studies would be helpful to address the effects of these treatment protocols on the treatment outcome.
Conclusion
In this prospective randomized study involving the assessment of post-SWL renal insult using imaging, clinical parameters, and measurement of urinary markers in 320 patients, the ramping protocol and the pause protocol were shown to have similar outcomes, including hematoma formation rate, complication rate, and change in acute renal injury markers compared with the control. Further studies would be needed to identify a better approach to minimize the potential complications of SWL.
Footnotes
Acknowledgment
The study was supported by the Hong Kong RGC General Research Fund (Grant No. 472111) of the Research Grants Council, Hong Kong.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.