
Abstract
Prostate cancer (PCa) is stratified into different risk categories based on the patient's prognosis. High-risk disease was formerly characterized by an increased risk of metastasis and lethality, requiring complex treatments. Surgery was recently highlighted to have a pivotal role for the treatment of such cases, even as monotherapy. In the past, open radical prostatectomy was performed for most patients with high-risk PCa; however, robot-assisted radical prostatectomy (RARP) emerged as a reasonable option because it provided optimal outcomes for low- and intermediate-risk PCa. Robust studies are lacking to properly assess the role of RARP for high-risk PCa. We summarize this knowledge and present a literature review on the perioperative recovery and functional and oncologic outcomes of RARP for the treatment of patients with high-risk PCa.
Introduction
W
The risk of biochemical recurrence (BCR) and cancer-specific mortality is 3.3 and 11.5 times greater, respectively, in patients with high-risk vs low-risk PCa. 1 For this reason, patients with high-risk disease are currently treated with a complex multimodal approach that includes surgery. However, evidence has emerged that supports surgery as monotherapy and has revealed optimal outcomes. 4,5
Robot-assisted radical prostatectomy (RARP) was introduced in the last decade and has become more common as its oncologic and functional outcomes have proved to be at least similar to open radical prostatectomy (ORP) in organ-confined disease. 6,7 The use of RARP was reported in patients with high-risk PCa to assess if the outcomes and benefits of this technique would be the same as seen in early and less aggressive disease. This report reviews the available studies evaluating the role of RARP in the setting of high-risk PCa.
Evidence Acquisition
A review was performed in June 2016 using the PubMed database to identify studies that reported RARP outcomes for high-risk PCa in English and with no specific period limitation. Search words comprised prostate cancer, high risk, locally advanced, prostatectomy, robot, and robotic. Reviews, editorial comments, and case reports were excluded. We found 167 references; 27 original articles were selected. Studies included addressed the use of RARP to treat high-risk or locally advanced PCa. Oncologic, functional, and surgical outcomes were extracted. Cross-references were used to complete the search.
Background
Controversies in stratification of high-risk PCa
D'Amico and colleagues stratified PCa in three risk categories according to the oncologic outcome. High-risk PCa, defined as a prostate-specific antigen (PSA) ≥20 ng/mL, Gleason score (GS) ≥8, and clinical stage T2c or higher, had a chance of posttherapy BCR >50% after 5 years. 8 Other definitions for high-risk PCa were proposed, comprising different values of PSA, percentage of core involvement in prostate biopsy, and distinct clinical staging (Table 1). In Europe, ∼70% of urologists adopt the National Comprehensive Cancer Network classification that differs from D'Amico's in including clinical T3 disease or greater. 9 Such heterogeneity impairs the comparison of outcomes between articles that may have uneven oncologic results due to different patient selection.
Limited template for PLND: comprise the obturator fossa lymph nodes. Extended template for PLND: comprise the obturator fossa and external and internal iliac lymph nodes.
Mean value.
Template = Obturator fossa and external iliac lymph nodes.
BCR = biochemical recurrence; BCRFS = biochemical recurrence-free survival; EXT = extended template; LIM = limited template; N = number of patients; NI = noninformed; PLND = pelvic lymph node dissection; PSM = positive surgical margin.
The classifications are susceptible to bias, and two considerations must be taken into account. Both upstaging and downstaging may occur, considering that clinical staging is subjective because digital rectal examination may be discordant between different examiners. 10,11 Another concern is the possibility of downgrading or upgrading. Lavery and colleagues reported a 28% chance of upgrading from biopsy GS 7 to GS 8 or 9. In the same series, 37% of the biopsies GS 8–10 were downgraded to a GS ≤7. 12 Category change has devastating consequences regarding the choice of an optimal treatment.
Among the most used risk parameters, high GS proved to be the most reliable predictor of outcome, followed by elevated PSA. The 10-year BCR-free rate is 24.1%, 26.4%, and 43.8% for GS ≥8, PSA ≥20 ng/mL, and cT3 cases, respectively. The prognosis is even worse when two of these risk factors are associated, with the BCR-free survival of ∼18% in 10 years. 3
Radical prostatectomy for high-risk PCa
The gold standard treatment for high-risk PCa has not been settled, and multimodal therapy has been adopted in most cases. Radical prostatectomy (RP) is often part of the treatment, but its role as monotherapy is not well established because the scientific literature still lacks prospective studies. Nonetheless, recent series reported encouraging results. In a study with 7538 patients, Cooperberg and colleagues concluded that patients treated with surgery as monotherapy had a significant reduction in mortality rate when compared with external-beam radiation therapy (EBRT) or androgen-deprivation therapy (ADT) for high-risk cases with a clinical stage of T3a or lower. The hazard ratio (HR) for cancer-specific mortality was 2.21 and 3.22 when comparing RP with EBRT and ADT, respectively. 4 A population study performed using the Prostate Cancer Data Base, which has matched >1800 high-risk patients per treatment modality, found an HR for PCa-specific mortality rate of 1.52 that also favored surgery over radiation therapy. 13
In another study, Boorjian and colleagues reported that surgery in high-risk PCa is followed by a greater cancer-specific survival (CSS) than EBRT alone and equivalent compared with EBRT combined with ADT (10-year CSS of 92%, 88%, and 92% for ORP, EBRT, and EBRT plus ADT, respectively). Nevertheless, the overall mortality rate of patients who received combined EBRT and ADT was higher, 14 perhaps due to increased cardiovascular morbidity and mortality rate associated with the androgen-suppressing drug. 15 More recently, Petrelli and colleagues performed a meta-analysis assessing 17 articles specifically for high-risk PCa and revealed cancer-specific mortality and overall survival (OS) odds ratios (ORs) of 0.56 and 0.51, respectively, favoring surgery over radiotherapy. 5
Other important aspects should be mentioned. First, when surgery is chosen as the first approach, salvage EBRT is possible. The reverse is feasible, but salvage RP after EBRT is a challenging intervention and followed by elevated surgical complication rates. 16 Second, with surgical treatment, we obtain the surgical specimen for pathologic analysis that is valuable to predict the patient's prognosis and the need for complementary therapy. Third, surgery offers a unique benefit for the high-risk patient: lymph node dissection to assess lymph node metastasis.
In this scenario, RARP emerged as an ideal treatment option for high-risk PCa, offering optimum oncologic and functional outcomes, with less postoperative pain, quicker convalescence, and even better aesthetic results. A literature review of early series comparing RARP and ORP showed that they provide similar clinical results considering both the functional and oncologic outcomes and these variables depend more on the ability of the surgeon than the surgical approach. 17 RARP for high-risk PCa thus became a reasonable option for skilled surgeons.
Evidence synthesis
The role of lymphadenectomy
Pelvic lymph node dissection (PLND) remains a topic of controversy when considering PCa surgery. There is an emerging consensus of its benefits for oncologic purposes, but it lacks high-level evidence. Nevertheless, PLND is considered the best method for lymph node staging, while efforts are ongoing to develop a precise preoperative imaging examination that could help in this setting.
Extended PLND (ePLND) plays an important role in addressing high-risk PCa. It includes the removal of the external iliac and hypogastric and obturator fossa lymph nodes; is time-consuming; and subjects patients to more related complications than limited PLND restricted to obturator fossa lymph node dissection. The extended technique prolongs the RARP by 30–45 minutes, and 19.8% of procedures had complications vs 8.2% of the limited PLND. 18 However, some findings support an extended template. Yuh and colleagues 19 found 13% of patients with lymph node metastasis in ePLND for RARP; 78% were from the obturator fossa. In another study, Briganti and colleagues 20 found twice as many positive lymph nodes when comparing ePLND with limited PLND (26% and 12%, respectively), similar to the preliminary results of one of the few randomized controlled trials performed (4.4% vs 10.7% of lymph nodal metastasis for limited PLND and ePLND, respectively). 21 Thus, a broad dissection seems appropriate to maximize the excision of affected lymph nodes.
Even with the uncertain therapeutic role of PLND, other evidences reinforce the use of the extended template when aiming for the best possibilities of cure for aggressive disease. Bader and colleagues analyzed PCa progression after ePLND. The HR for PSA relapse and cancer-related death for each positive lymph node resected was 1.36 and 1.31, respectively. The more advanced the pathologic stage, the higher the number of positive lymph nodes that were encountered. 22
Regarding lymph node yields, different studies have demonstrated that they are similar when comparing the robotic and open technique, depending more on the experience of the surgeon and pathologist than the surgical method. 23 For instance, Ploussard and colleagues in a systematic review found a median yield ranging from 7 to 24 lymph nodes resected when performing ePLND in RARP. 23 It was also shown that extraperitoneal access for RARP does not limit the lymph node resection yield. Therefore, the PLND extension and yield are feasible with the robotic approach (Table 1).
Postoperative morbidity
Some of the known advantages of minimally invasive surgery compared with ORP are rapid convalescence, less bleeding, and decreased analgesic intake. The risk of blood transfusion is 7.5 times higher in ORP than in RARP. 24 Tewari and colleagues conducted a systematic review and meta-analysis comparing ORP and RARP in all risk categories and found a 7% greater risk of perioperative complications for ORP and twice as many postoperative hospitalization days. 25
Concerning high-risk PCa, Ham and colleagues compared the outcomes of RARP performed in organ-confined and locally advanced PCa and found no statistical difference between these two groups in many perioperative features such as duration of surgery, blood loss, length of hospital stay, and intraoperative complications. 26 Another study addressing RARP for high-risk PCa demonstrated similar convalescence compared with ORP in the elderly population, in which surgery complications were expected to be higher. 27
Thromboembolism may be more frequent in high-risk patients as a consequence of mandatory PLND. A multicenter study that analyzed >3500 patients undergoing RP showed that PLND increased the risk of deep vein thrombosis and pulmonary thromboembolism by eight and sixfold, respectively. Despite this worrisome finding, PLND during ORP was associated with more thrombotic events compared with RARP (relative risk of 12.6 vs 7.5, respectively), likely favoring RARP for better convalescence. 28
A few contemporary RARP series for high-risk PCa reported rates of total and major complications that ranged between 4% and 29% and between 0% and 9.1%, respectively. 11,26,27,29 –33 In light of heterogeneous results and a lack of robust studies, the benefits of minimally invasive surgery on perioperative recovery can be expected to be the same for RARP in the high-risk setting (Table 2).
Mean value.
Complications recorded until 30 days after surgery.
Bil = Bilateral; EA = erectile aid; PDI = phosphodiesterase inhibitor; PEN = penetration; MAST = capability to masturbate; SHIM = Sexual Health Inventory for Man questionnaire; Uni = unilateral.
Oncologic outcomes
A criticism of RARP is the lack of haptic interface that could impair the effort to obtain negative margins over functional preservation. The visual enhancement of the three-dimensional image and the magnification of the robotic system help overcome this problem. A systematic review and meta-analysis assessed the positive surgical margins (PSMs) of series comparing ORP and RARP in all risk categories, demonstrating no differences between surgical methods. 34
When addressing high-risk PCa, the PSMs reported for RARP vary from 16% to 58%. 10 –12,26,27,29 –33,35 –49 Such heterogeneity of PSMs is also seen in contemporary ORP series, ranging approximately from 18% to 48%. 1,50,51 Suardi and colleagues recently evaluated the PSMs of >1900 patients with high-risk PCa undergoing surgical treatment and found an OR of 0.69 favoring RARP over ORP (p = 0.04). 52 Despite the former study, most series comparing surgical methods among high-risk patients found no difference in the rate of PSMs. Harty and colleagues compared PSMs among high-risk patients who underwent ORP, RARP, and laparoscopic prostatectomy, reporting no significant difference among surgical methods (53%, 41%, and 50%, respectively; p = 0.13). 40 After a propensity score match, Lee and colleagues reported PSM rates of 36% and 34% (p = 0.76) for patients undergoing ORP and RARP, respectively. 49 Another propensity score that matched a cohort from the Surveillance, Epidemiology, and End Results database found PSMs in 18% of ORP cases and in 22% of RARP cases (p = 0.4). 32 Table 3 summarizes the PSMs after RARP.
NCCN criteria: PSA ≥20 ng/mL, clinical stage ≥T3, and Gleason Score ≥8; D'Amico criteria: PSA ≥20 ng/mL, clinical stage ≥T2c, and Gleason Score ≥8.
Median values.
Bx = percentage of biopsy cores involved; GS = Gleason score; PSA = prostate-specific antigen; pT = pathologic stage.
Current RARP studies for high-risk PCa report the BCR rate ranging from 13% to 35%. 11,12,27,28,31,33,38,43,44,48 Although some of the reviewed articles did not mention the PSA cutoff used, most considered PSA ≥0.2 ng/mL as a marker for disease recurrence. However, most series lack a long follow-up, which might explain discrepant results (Figs. 1 and 2).
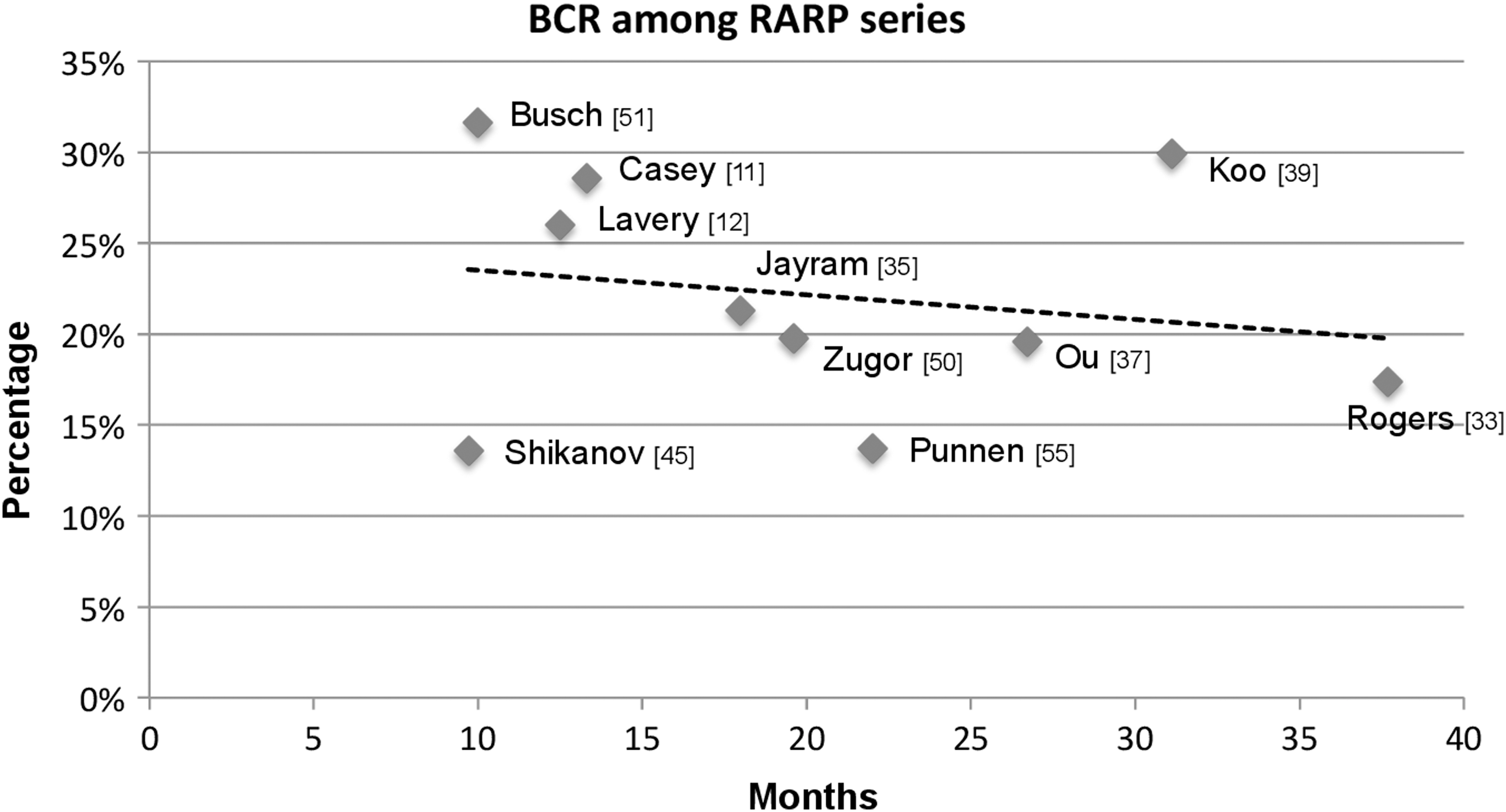
Biochemical recurrence reported by RARP series. RARP = robot-assisted radical prostatectomy.
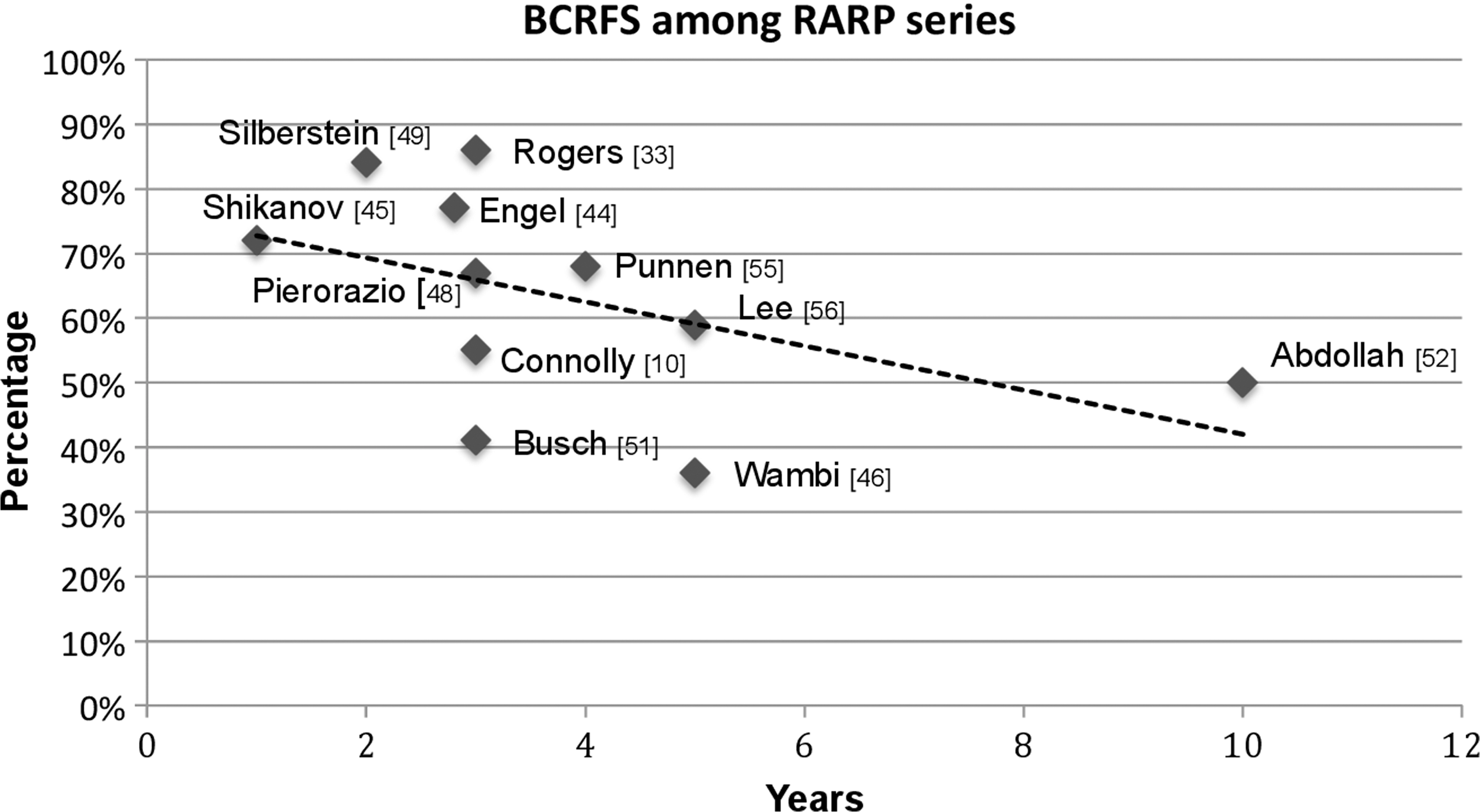
Biochemical recurrence-free survival reported by RARP series.
Survival analysis comparing RARP and ORP showed equivalent disease recurrence rates. In an ORP study published by Walz and colleagues with 887 high-risk PCa cases, the BCRs for 2, 5, and 10 years of follow-up were 35.2%, 52.6%, and 64.3%, respectively. 51 In another study from the Mayo Clinic, the BCRs at 5 and 10 years after ORP were 32% and 45%. 1 Concerning the RARP series, Abdollah and colleagues assessed the biggest cohort to date including 1100 patients and found a 10-year BCR-free rate of 50.4%. 45 Randomized studies comparing RARP and ORP for high-risk PCa are lacking. Existing retrospective series analyzing different surgical approaches found a similar BCR-free rate for ORP and RARP 41,42,44,48,49 (Table 4).
p value for comparison between RARP and ORP.
LAP = laparoscopic radical prostatectomy; NA = nonapplied; ORP = open radical prostatectomy.
Estimates of CSS and OS are a major concern for high-risk patients; however, they were scarcely reported in current series. Two studies found 100% of CSS in their high-risk PCa cohorts treated with RARP. 10,41 Busch and colleagues compared the OS between patients treated with RARP and ORP and found no difference between methods (RARP 95% vs ORP 100%; p = 0.09). 44 In summary, to the best of our knowledge, the surgical method does not influence the oncologic outcomes.
Functional outcomes
The complex anatomy of the pelvic muscles and their innervation have been broadly scrutinized, generating several surgical maneuvers during RP to improve urinary continence recovery. In this scenario, the motion and visual advantages of RARP were initially regarded with enthusiasm. Different case series studies demonstrated early continence recovery (<90 days) after RARP when performing careful apex dissection, anterior and posterior reconstruction, and bladder neck preservation. 53 –55 However, a prospective nonrandomized trial analyzing 12-month continence in all risk categories revealed similar results between RARP and ORP (OR: 1.08; 95% confidence interval [CI], 0.87, 1.34). 7 Studies contemplating high-risk PCa patients demonstrated heterogeneous continence outcomes after RARP. Rogers and colleagues reported that 82% of his cohort used one or no pad daily 12 months after RARP. 27 Koo and colleagues had inferior results using a no-pad definition (33% of continence at 12 months). 33 However, both studies addressed the elderly population (aged >70 years), and age is a known paramount variable for continence recovery. Other series for RARP in high-risk PCa reported satisfactory outcomes, ranging from 92% to 100%. 11,29,35,41
Potency preservation is challenging in high-risk patients who are more likely to have the neurovascular bundle (NVB) sacrificed during surgery. Bilateral NVB sparing may be performed for organ-confined disease, and unilateral NVB sparing is feasible in selected patients with T3 PCa. Jayram and colleagues reported 80% nerve sparing during RARP in a high-risk cohort, of which 29% were bilateral. Potency rate was 51% (capability to masturbate) with 6 months of follow-up and PSMs was 20%. 29 Lavery and colleagues achieved greater rates of bilateral NVB preservation (58%), performing an intraoperative frozen section of the NVB in selected cases to assure negative margins. Within a median follow-up of 12 months, 56% of the patients were potent (Sexual Health Inventory for Men ≥16), and no association was found between NVB sparing and PSM. 12 Casey and colleagues performed bilateral NVB sparing in 57% of pT3 or higher patients and reported 20% PSMs. 11 Although the potency rate was not mentioned, the author obtained satisfactory PSM rates in locally advanced disease. Articles regarding RARP for high-risk PCa reported potency rates ranging from 20% to 60% (Table 5). 12,29,31,46 Accordingly, the functional outcomes seem to depend on surgeon diligence and PCa population characteristics rather than surgical approach.
Erectile Aid: Phosphodiesterase inhibitor, intraurethral Alprostadil, intracavernous Papaverine injection and vacuum pump.
Mean value.
Institutional experience
We reviewed our PCa database retrospectively. Since 2003, 5695 minimally invasive RPs were performed at our institution, of which 199 were RARP in patients with D'Amico criteria for high-risk PCa. Table 6 lists the demographic characteristics of our cohort. The median duration of surgery was 130 minutes (range: 90–390), and the rate of blood transfusion was 3.5%. Median hospitalization time and bladder catheter time were 4 days (range: 2–18) and 8 days (range: 5–25), respectively, following institutional guidelines. PLND, metastatic lymph nodes, and lymphocele were seen in 80.4%, 8.1%, and 3% of the cohort, respectively. Complications were observed in 12.1% of the patients (4.5% of major complications per the Clavien classification). NVB sparing was performed in 80.9% of the RARPs (unilateral in 36.6% and bilateral in 44.3%), and the rate of PSMs was 25%. With a median follow-up of 23 months (interquartile range: 12–34), 31% of the patients had BCR (two measurements of PSA ≥0.2 ng/mL). Five-year BCR-free survival was 34.5% estimated with Kaplan–Meier curves (Fig. 3). Cox proportional hazards regression was used to evaluate variables associated with BCR. GS ≥8, PSA ≥20 ng/mL, and PSMs were not predictors of BCR. A positive correlation of pathologic stage T3 or higher and BCR was found (HR: 2.9; 95% CI, 1.2, 6.9).

Kaplan–Meier Curve of BCRFS for patients with high-risk prostate cancer treated with RARP at our institution. BCRFS = biochemical recurrence-free survival.
Our cohort exhibited poor rates of BCR and BCR-free survival compared with a former series. Nevertheless, the rates of PSMs were satisfactory, particularly in a population in which 55% had stage pT3. Conversely, patients with pT3 disease had a threefold greater risk of having BCR. The assurance of negative PSMs could not preclude patients from recurrence. These findings emphasize the severity of high-risk PCa, which in many cases requires a complementary treatment.
Conclusions
The available literature regarding the role of RARP for high-risk PCa is still limited and lacks studies with a high level of evidence. The great majority of published articles include a relative small number of patients, with different high-risk PCa criteria and with follow-up.
Early data on RARP for high-risk PCa are appealing, however, and suggest that oncologic and functional outcomes are similar to those of ORP. Nerve sparing appears to be feasible in selected cases without affecting the rate of PSMs. RARP offers unquestionable perioperative recovery advantages. Regarding PLND, its therapeutic role is still uncertain, but evidence shows that it is not a limitation for the robotic technique, no matter the extension. In conclusion, RARP as monotherapy or as the first step of a multimodal approach offers optimum therapeutic performance with advantages in perioperative recovery for patients with high-risk PCa.
Footnotes
Author Disclosure Statement
No competing financial interests exist.