
Abstract
Purpose:
To properly use the Ureteric Symptom Score Questionnaire (USSQ) to evaluate, in a randomized control study, the effect of tamsulosin, solifenacin, and their combination in improving symptoms and quality of life in patients with indwelling ureteral stents.
Materials and Methods:
After institutional review board approval, 260 patients with a ureteral stent were randomly assigned to receive tamsulosin 0.4 mg, solifenacin 5 mg, or placebo and further randomized to receive their combination. The validated USSQ was completed 1 and 4 weeks after stent insertion and 4 weeks after stent removal. Kruskal-Wallis test, chi-squared test (or Fisher's exact test), one-way analysis of variance, and T-test (or Wilcoxon rank-sum test if not normal data) were used for statistical analysis. The results were considered significant at p < 0.05.
Results:
Patients receiving tamsulosin or solifenacin expressed significantly lower urinary (p < 0.001), pain (p < 0.001 with stent in situ), and general health index (p = 0.002 in first and p < 0.001 in fourth week with stent in situ) scores. Sexual life and quality of work were also positively influenced. Patients on combination therapy expressed lower urinary (p < 0.001) and pain (p < 0.001) scores in the fourth week with stent in situ and work performance in the first week and with stent in situ (p = 0.001) and after stent removal (p = 0.005). No patients had to discontinue medication due to side effects.
Conclusions:
Stent-related morbidity is a reality in the majority of patients. Simple medication, such as tamsulosin and solifenacin alone or in combination, improves stent-related symptoms and has a positive impact on quality of life.
Introduction
U
The efficacy of several pharmaceutical agents has been evaluated, in general, in several recent studies, with many of them being randomized controlled trials as well as meta-analyses. Interestingly, almost all aforementioned studies are not uniformly designed; however, we should underline that although they used the only validated stent-related symptom questionnaire (USSQ), unfortunately the vast majority did not report or did not evaluate all aspects of USSQ. Furthermore, in most of them, the USSQ has been assessed at several time points instead of the first and fourth week with the stent in situ and fourth week after stent removal, as has been suggested by Joshi and colleagues. 5 The aforementioned facts deliberately impede the proper data evaluation as well as underpower their statistical significance, since their results cannot be compared with similar studies.
In the present randomized placebo-controlled study, we set out to overcome aforementioned limitations, to properly use USSQ to evaluate simultaneously the efficacy of tamsulosin with solifenacin compared with placebo, and to further compare for the first time in the literature the aforementioned agents with a combination of tamsulosin plus solifenacin. The proper use of USSQ should be underlined for the sake of accuracy and objectivity.
Materials and Methods
After institutional review board approval and verbal informed consent were obtained, 260 patients, 131 men and 129 women, aged 17 to 84 (median 48 years), with a unilateral Double-J ureteral stent were included in this randomized controlled study. All patients underwent insertion of a Double-J ureteral stent, routinely placed for 4 weeks. The indications for stent placement were extracorporeal shockwave lithotripsy (SWL) (124 patients), ureteroscopic stone treatment (URL) (69 patients), and unilateral hydronephrosis or any reason (67 patients). All patients were prospectively randomized with a box with random numbers into three groups (groups 1, 2, and 3) from April 2012 to March 2015. In group 1, 60 patients (30 men and 30 women, median age 48 years) received 0.4 mg of tamsulosin once daily for 4 weeks. In group 2, 60 patients (27 men and 33 women, median age 49 years) received 5 mg of solifenacin once daily for 4 weeks. In group 3, 60 patients (32 men and 28 women, median age 45 years) received placebo once daily for 4 weeks. At this point of our study, after institutional review board approval, we decided to add group 4, where patients received a combination of tamsulosin 0.4 mg plus solifenacin 5 mg once daily again after verbal informed consent was obtained; whereas groups 1, 2, and 3 continued to receive their medication as originally set. From March 2015 to March 2016, we randomized patients into four groups: group 1 with 20 patients (12 men and 8 women, median age 53.5 years), group 2 with 20 patients (10 men and 10 women, median age 55 years), group 3 with 20 patients (9 men and 11 women, median age 53.5 years), and group 4 with 20 patients (11 men and 9 women, median age 44 years), respectively. At the end of our study, we had randomized 80 patients in group 1, 80 patients in group 2, 80 patients in group 3, and 20 patients in group 4 (Fig. 1).
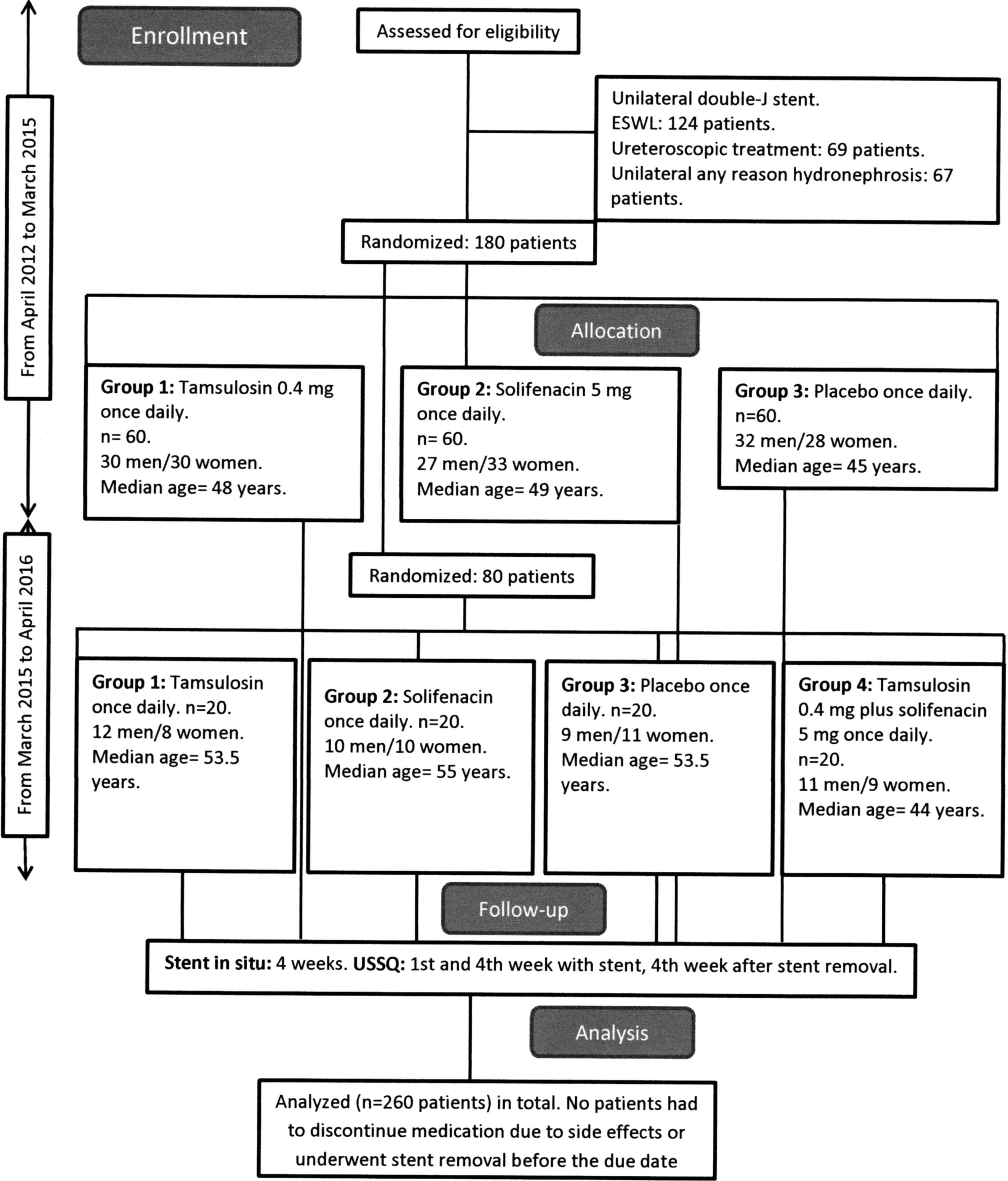
CONsolidated Standards of Reporting Trials (CONSORT) diagram for study cohort.
The inclusion criteria were cases with ureteral stones <10 mm with or without concomitant dilation of renal pelvis, calices, or ureter and cases with dilation of ureter and/or pelvicaliceal system or any other reason. The exclusion criteria included patients with renal stones, pregnancy, patients with bilateral or “forgotten” stents, stent placement during percutaneous, laparoscopic or open transperitoneal procedures, patients with history of pelvic irradiation and/or surgical procedures in the minor pelvis, and patients with history of reconstructive ureteric surgical procedures. During the stenting period, analgesic intake was standardized with 4 weekly prescriptions of paracetamol (500 mg when needed, up to four times per day, total of 28 tablets). The overall analgesic intake was registered at the end of the 4-week period, with the total tablet intake documented and compared. The same Double-J ureteral stent was used (Percuflex plus, Boston Scientific, Natick, MA) in all patients. The stent size varied (6F/24 cm or 6F/26 cm); it was selected according to the patient's somatometric characteristics and was inserted under fluoroscopic control in all cases.
All consenting patients were fully informed regarding the potential side effects of tamsulosin and solifenacin. To assess the stent-related morbidity, patients completed the validated USSQ 1 and 4 weeks after stent insertion and 4 weeks after stent removal, as it was originally set by Joshi and colleagues. 3 Given the fact that the USSQ validation process in Greek language is ongoing, all questionnaires were translated at the time of assessment by the same non-medical professional person with professional English language skills. The end of the study was 4 weeks after the stent removal with the final USSQ completed.
The USSQ is a self-administered multidimensional measure designed for use in clinical and research settings. It evaluates stent-related morbidity in six sections, including urinary symptoms, body pain, general health, work performance, sexual matters, and additional problems with each section calculated score providing the urinary index score (UIS), pain index score (PIS), general health index score (GHIS), work performance score (WPS), and sexual matters score (SMS), respectively.
Statistical analysis
We chose a sample size of 60 patients in each group to have an 80% power at 5% significance level to detect a 4% difference in UIS, a 4% difference in PIS, a 9% difference in GHIS, a 9% difference in WPS, and a 23% difference in SMS. Later, we chose a sample size of 20 patients in each group to have an 80% power at 5% significance level to detect a 7%, 7%, 14%, 14%, and 35% difference, respectively. Statistical analysis was performed by using the Kruskal-Wallis test for independent samples for non-normally distributed variables and the chi-squared test (or Fisher's exact test in cases with small numbers in cells) to check for independence between categorical variables. One-way analysis of variance (ANOVA) for independent samples was applied to compare for differences in case of normally distributed continuous variables, and the T-test (or Wilcoxon rank-sum test if not normal data) was used to test the hypothesis that two independent samples are from populations with the same distribution. The results were considered significant at p < 0.05. Descriptive statistics, including mean, median, and range for continuous variables, and number and percentage for categorical variables were obtained for each study variable. All analyses were carried out in STATA/SE 14.1 (Copyright 1985–2015 StataCorp LP).
Results
Patient characteristics are detailed in Table 1. There were no statistical significant differences between patients' characteristics among groups. After adding the group 4 in our randomization, a significant difference regarding intervention was observed (p = 0.002). In total, 124 patients underwent SWL, with 89 (71.8%) of patients being stone free, 69 had URL (all of them stone free), and 67 patients had an indwelling stent inserted because of ureteral and/or pelvicaliceal system dilation or any other reason.
ANOVA.
Chi-squared test.
Fisher's exact test.
SWL = extracorporeal shockwave lithotripsy; URL = ureteroscopic lithotripsy.
Our overall results are listed in Table 2. All of our patients were divided into two cohorts: the first with initial randomization in three groups of patients (tamsulosin, solifenacin, and placebo groups, respectively) and the second with further randomization after the addition of group 4 (patients with tamsulosin plus solifenacin combination).
ANOVA.
T-test.
Wilcoxon rank-sum test.
Kruskal-Wallis test.
In the first cohort, patients on either tamsulosin or solifenacin expressed a significantly lower UIS, PIS, and GHIS (overall p < 0.001, p < 0.001 with stent in situ and p = 0.002 and p < 0.001 with stent in situ, respectively), with the latter reflecting better general health. SMS was also positively influenced in the post-stenting period (p = 0.006), whereas there was a marginally non-significant change in the first week (p = 0.057). As far as WPS is concerned, it was positively influenced significantly only in the fourth week (p = 0.021). Interestingly, when the p-value is adjusted for intervention (cases with SWL and URL and cases with simple stent insertion), our results were similar, apart from SMS. This fact shows that the positive impact of agents is significant, irrespective of any kind of intervention. There was no significant difference among the groups on tamsulosin or solifenacin, favoring the one or the other regimen as better in relation to stent symptom relief.
In the second cohort, patients on combination of drugs expressed a significant improvement in UIS and PIS in the fourth week with stent in situ (p < 0.001 and p < 0.001, respectively) and WPS after stent removal (p = 0.001) compared with patients on tamsulosin, solifenacin, or placebo, with no significant improvements in other USSQ sections. Solifenacin significantly improved GHIS in the fourth week (p = 0.012) and SMS in the first week (p = 0.009). Both tamsulosin and solifenacin significantly improved SMS in the first week (p = 0.009), whereas both aforementioned regimens and their combination significantly improved WPS in the first week (p < 0.003). When the p-value is adjusted for intervention in this cohort, our results showed the same fluctuations, a fact showing that the positive impact of agents and their combination is significant, irrespective of any kind of intervention. There was no significant difference among the groups on tamsulosin, solifenacin, or their combination, favoring the one, the other, or their combination as better in relation to stent symptom relief, although our sample was relatively small. What is of importance in this cohort of patients is that combination therapy showed a marginally significant improvement when administered to male patients (p = 0.048) in UIS in the fourth week.
No patients had to discontinue medication because of side effects or underwent stent removal before the due date.
Discussion
This study is the first in the literature to evaluate the effectiveness of two commonly used pharmaceutical agents, tamsulosin and solifenacin, either sole or in combination compared with placebo in relieving stent-related symptoms. Tamsulosin is an already known agent with proven effectiveness in stent-related morbidity, 6 whereas solifenacin has been used to overcome symptoms caused by the involuntary contraction of the bladder due to the distal end of the stent in the urinary bladder, with encouraging results. 7 We planned to use the combination of the two agents in an attempt to combine their activity and to compare the combination effectiveness with tamsulosine, solifenacin, and placebo.
This comparison constitutes the originality of our work, since it is evaluated with the proper use of USSQ in the first and the fourth week with the indwelling stent in situ and 4 weeks after stent removal. 5 The use of such a validated questionnaire facilitates the uniform evaluation of different stents and the efficacy of medication for stent-related morbidity. In the literature, although there are numerous prospective studies using several agents, they do not assess the USSQ as it is suggested by its inventors in their vast majority. As a result, we cannot properly evaluate or compare their results nor can we earn safe conclusions regarding effectiveness issues.
The initial concept of a α-blocker administration in patients with indwelling stents was that these patients were suffering of symptoms mimicking benign prostatic hyperplasia-related symptoms. In the pioneering study of Deliveliotis et al., 8 it was the first time where alfuzosin, a competitive antagonist of α1-receptors, was used in clinical practice to improve stent-related symptoms. In their prospective randomized placebo-controlled study, the authors concluded that alfuzosin improved symptoms and quality of life, whereas sexual life and general health were better preserved. The pitfall of that study was that they only administered the USSQ 4 weeks after stent insertion. After the aforementioned study, there have been several other trials that are prospective in nature, evaluating orally administered agents and dosages, but with considerable heterogeneity in design and methodology. Even the most recent of them 6,7,9 –20 (Table 3), although the USSQ is the only validated questionnaire for the assessment of stent-related symptoms per se with established accuracy, failed to uniformly use it in the stent morbidity evaluation. Apart from that, only almost half of them were placebo controlled, 6,7,10,13,14,16,19,20 four studies had a control group, 11,15,17,18 and two studies were not controlled at all. 9,12
Compared with placebo.
Improper USSQ assessment.
GHIS = General Health Index Score; IPSS = International Prostate Symptoms Score; OABq = Overactive Bladder Questionnaire; PIS = Pain Index Score; Proper = first and fourth week with stent in situ, fourth week post-stenting; QoL = quality of life; QoW = quality of work; SL = sexual life; UIS = Urinary Index Score; USSQ = Ureteric Symptom Score Questionnaire; VAPS = Visual Analogue Pain Scale; VAS = Visual Analog Scale.
Furthermore, several meta-analyses have been published during the past 5 years 21 –26 (Table 4). The common conclusion of all of them is that α-blockers significantly improve UIS and PIS. In all other meta-analyses' end-points, there is a wide spectrum of conclusions from significant to insignificant improvements of other USSQ sections, whereas there are cases where a meta-analysis could not be performed due to insufficient or unavailable data on relevant USSQ sections. 22,23
Our study is very important for several reasons. First of all, it is the first and sole study with a direct comparison of an α-blocker, an anticholinergic, and their combination with placebo and it was designed to overcome all aforementioned limitations regarding diversity of data assessment. Although in the literature there were several studies comparing the impact of α-blockers with anticholinergics or combination therapies on stent-related urinary symptoms, work performance, or sexual life, there were no published data comparing an α-blocker with an anticholinergic, with their combination and placebo. In addition, we have to underline that our study is one of the very few in the relevant literature where the validated USSQ is properly assessed for all included patients as it has originally been introduced by Joshi and colleagues. 3 The rationale for questionnaire administration to determine baseline symptoms after stent removal is that many patients before stent insertion will have significant pain from a ureteral stone, whereas some of them might have complaints because of the intervention as well. Furthermore, for the first time, it is evaluated whether SWL or the endoscopic intervention influences the effectiveness of administered agents. This could be used to better cover our patients with painkillers or a combination of agents in any case of intervention, especially complicated ones or SWL in cases of larger stone burdens.
Of course, our study has several drawbacks. First, our sample size, although the second biggest in the recent literature, was statistically small to detect small differences, especially between the isolated agents and their combination. We evaluated the impact on patients' life for certain agents only, not for new agents, such as silodosin or mirabegron. Although the USSQ is self-administered, since there is no validated translation of USSQ in Greek, we were forced to translate all questionnaires at the time of assessment. No patients discontinued medication or their combination because of side-effects; however, we did not formally evaluate any side effects caused by their use. The fact that we included and compared different interventions might be reserved as a limitation, but since the intervention per se is proved statistically insignificant we retrospectively consider this variety an advantage. Finally, although we tried to evaluate and compare the combination of tamsulosin and solifenacin with tamsulosine, solifenacin, and placebo, the fact that we further randomized patients in a second cohort perhaps weakens our study's statistical power.
Conclusions
Adopting the proper use of USSQ, apart from confirming tamsulosin and solifenacin's positive impact on several aspects of patients' lives, it seems that their combination is further more efficient compared with each one of them and placebo in certain USSQ aspects, although larger populations are needed to strengthen statistical power. Interestingly, combination therapy seems to have a marginally significant positive impact on men UIS. Since new agents have already shown up and added in our armamentarium in the α-blockers family as well as mirabegron, further research is needed to determine whether these new agents or their combination with already existent formulas could offer more in stent-related symptoms management. Randomized controlled studies with larger patient populations, even multicenter ones, could earn more accurate and safe conclusions regarding benefits or pitfalls in the field of ureteral stent-related symptom relief.
Footnotes
Author Disclosure Statement
No competing financial interests exist.