
Abstract
Purpose:
Standardized bench testing of the new ShockPulse™ intracorporeal lithotripter was performed against three commercially available lithotripsy systems to determine differences and nuances in performance.
Materials and Methods:
The ShockPulse intracorporeal lithotripter was tested against the LUS-2™, CyberWand,™ and EMS LithoClast™ in a standardized bench setting using hard (Ultracal-30) and soft (plaster of Paris) stone phantoms. An in vitro kidney model was used to record the time needed to fragment stone samples into retrievable-sized pieces. The time needed to fully comminute and evacuate stone samples was also recorded. The efficacy of each device at various applied pressures was determined using a hands-free apparatus, which was used to apply 1.0, 1.5, and 2.0 pounds of fixed force.
Results:
For hard and soft stones, the time needed to create retrievable fragments was similar among all systems (p = 0.585). The ShockPulse was significantly faster than the LUS-2 and LithoClast at fully fragmenting and evacuating stone samples (p = 0.046), while the CyberWand was significantly slower than all three systems at this task (p = 0.001). When fixed forces were applied to a large stone phantom, the ShockPulse and CyberWand were significantly faster than the LUS-2 and LithoClast (p < 0.0001). When groups of smaller stones were tested, the ShockPulse was significantly faster at 1.0 pound (p < 0.001) and 1.5 pounds (p < 0.002) of force. At 2.0 pounds, no differences were observed (p = 0.09).
Conclusions:
The ShockPulse is equally as effective and, in some circumstances, more effective than the three commercially available devices against which it was tested in an in vitro setting.
Introduction
P
Three commonly used lithotripters include the LUS-2™ (Olympus, Center Valley, PA)—a compact, lightweight ultrasonic device; the CyberWand™ (Olympus)—a concentric, dual-probe ultrasonic device; and the EMS LithoClast™ (Nyon, Switzerland)—a combined ultrasonic and pneumatic system. Although each device offers a perceived advantage over its counterparts, standardized testing has yielded variable results. 5,6 Recently, Olympus introduced the ShockPulse Stone Eliminator™; a combined ultrasonic and pneumatic lithotripter. On behalf of the Endourology Disease Group for Excellence Consortium, we sought to test this novel lithotripter in a standardized benchtop setting with both hard and soft stones. This device was compared with the three aforementioned systems in several tests of in vitro efficiency. Herein, we describe the results of our standardized bench testing of this novel lithotripter as it compares with the LUS-2, LithoClast, and CyberWand. We also sought to examine the clinical performance of ShockPulse in patients undergoing PCNL at the University of British Columbia.
Materials and Methods
The instrument
The ShockPulse intracorporeal lithotripter consists of a handpiece transducer, which houses piezoelectric elements that produce 21,000 Hz of ultrasonic energy. The handpiece also contains a suction control dial, allowing for hand-activated suction control—the first of its kind for an intracorporeal device (Fig. 1). It is also the first intracorporeal lithotripter that does not require a foot pedal, adding valuable floor space adjacent to the operating table. If preferred, foot pedal suction control is also possible.

(1) Suction control dial and (2) mechanical power settings.
The single-probe design employs free mass elements at the proximal end of the probe, which oscillate to produce mechanical shockwaves (Fig. 2). These shockwaves are transmitted to an adjacent return spring, which then propagate down the probe, delivering 300 Hz of mechanical energy. Energy settings are predetermined and can be set to either normal or high intensity. Theoretically, these pneumatic forces produce enough energy to rapidly fragment the hardest regions of the stone, while ultrasonic energy disintegrates the softer components.
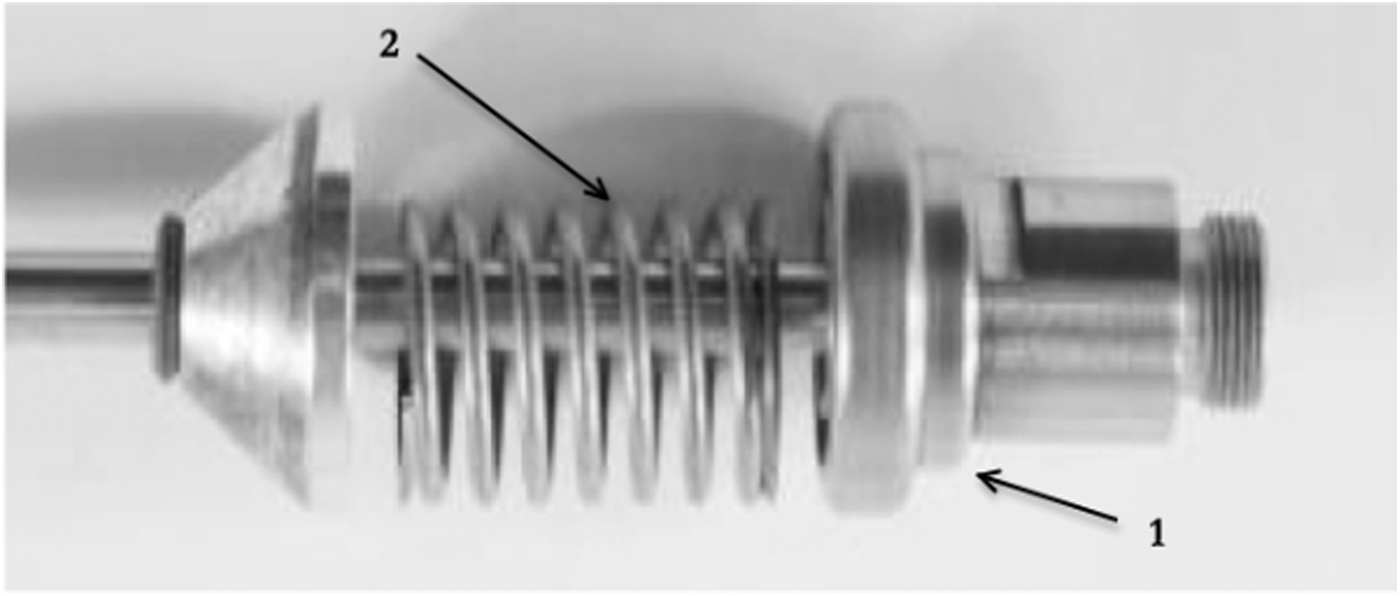
(1) Free mass elements and (2) adjacent return spring.
Probes
The 3.76-mm ShockPulse probe has the largest lumen of any existing device, measuring 3.2 mm. The luminal surface area is 36% and 123% larger than the LUS-2 and CyberWand probes, respectively. Unlike the LithoClast, the only other combination lithotripter in this study, the ShockPulse probe does not feature a luminal pneumatic probe. The absence of this probe affords the ShockPulse a much greater luminal surface area. For the purposes of this study, the pneumatic component of the LithoClast probe was not activated during in vitro testing.
In vitro testing
The in vitro testing protocol simulated hard and soft calculi using Ultracal-30 (U30) and plaster of Paris (POP) stone phantoms, respectively. These were created using a standardized mold, which ensured each stone was identical in mass and surface area. Stones were placed in a simulated kidney model comprising an open rubberized container submersed in a water tank.
The time needed to fragment the stones in retrievable-sized pieces was tested, which was recorded by an observer operating a stopwatch. Stone fragments were deemed retrievable when they were small enough to be extracted through a 30F Amplatz access sheath. Free mass removal was the subsequent measurement that was recorded. This was the time needed to completely disintegrate and evacuate stone fragments using suction. Each device was tested six times using a 26F nephroscope equipped with continuous irrigation and 165 mm Hg of suction. A 3.76-mm probe was used for the ShockPulse and CyberWand systems. A 3.8-mm probe was used for the LithoClast and a 3.7-mm probe was used for the LUS-2.
Fixed force testing was also performed, whereby each device was vertically fastened to a hands-free apparatus with the tip of the probe oriented downward (Fig. 3). To determine the efficacy of each system at various forces, 1.0, 1.5, and 2.0 pounds of force were applied to each probe while in direct contact with U30 stone samples. First, each probe was tested against a single large stone, which simulated a large renal calculus. The probes were then tested against groups of six vertically stacked smaller stones, which simulated multiple small calculi. This process was repeated three times for the large stones and five times for the small stones, respectively. The spaces between the smaller stones offered a more clinically relevant model since it is unusual to completely drill through a large stone from end to end with consistent pressure as the lumen of the lithotripsy probe may become plugged. An automatic timer was started once the tip of the probe came into contact with the stone. The apparatus was arranged in an electronic circuit such that once the tip of the probe penetrated through the stone and came into contact with the metal surface of the test table, the circuit was completed and the timer automatically stopped (Fig. 4).
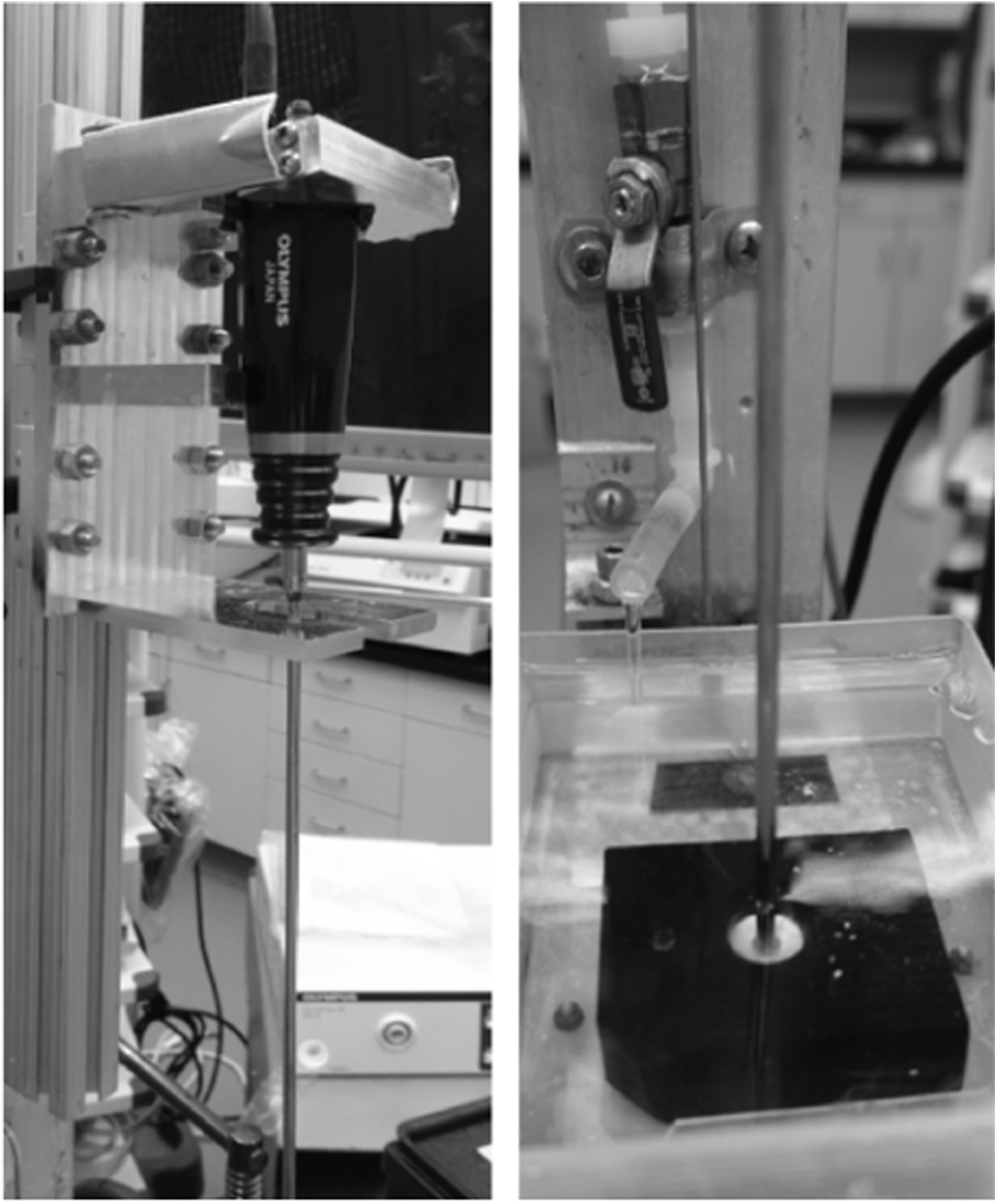
Hands-free apparatus utilized for fixed force testing.

Lithotripter probe in contact with metal surface of test table, thus completing the electronic circuit.
For all in vitro testing, the paired Student's t-test was used for statistical analysis. Univariate and multivariate analyses were performed using standard computerized software. A p-value of less than 0.05 was considered statistically significant.
Clinical testing
Six patients were scheduled for PCNL during the period where the ShockPulse was trialed at our institution. Patient demographic factors, stone size, postoperative stone-free status, and stone analyses were recorded. Pre- and postoperative serum creatinine and hemoglobin were documented. The ShockPulse system was used for all six procedures. Endoscopic graspers and baskets were utilized at the surgeon's discretion. Flexible nephroscopy was carried out and fluoroscopy was utilized to ensure that patients were stone free before terminating each procedure.
Results
Time to retrievable fragments
The time needed to fragment stones into fragments deemed retrievable by endoscopic forceps was recorded for each system. No significant differences were observed (p = 0.585; Fig. 5).
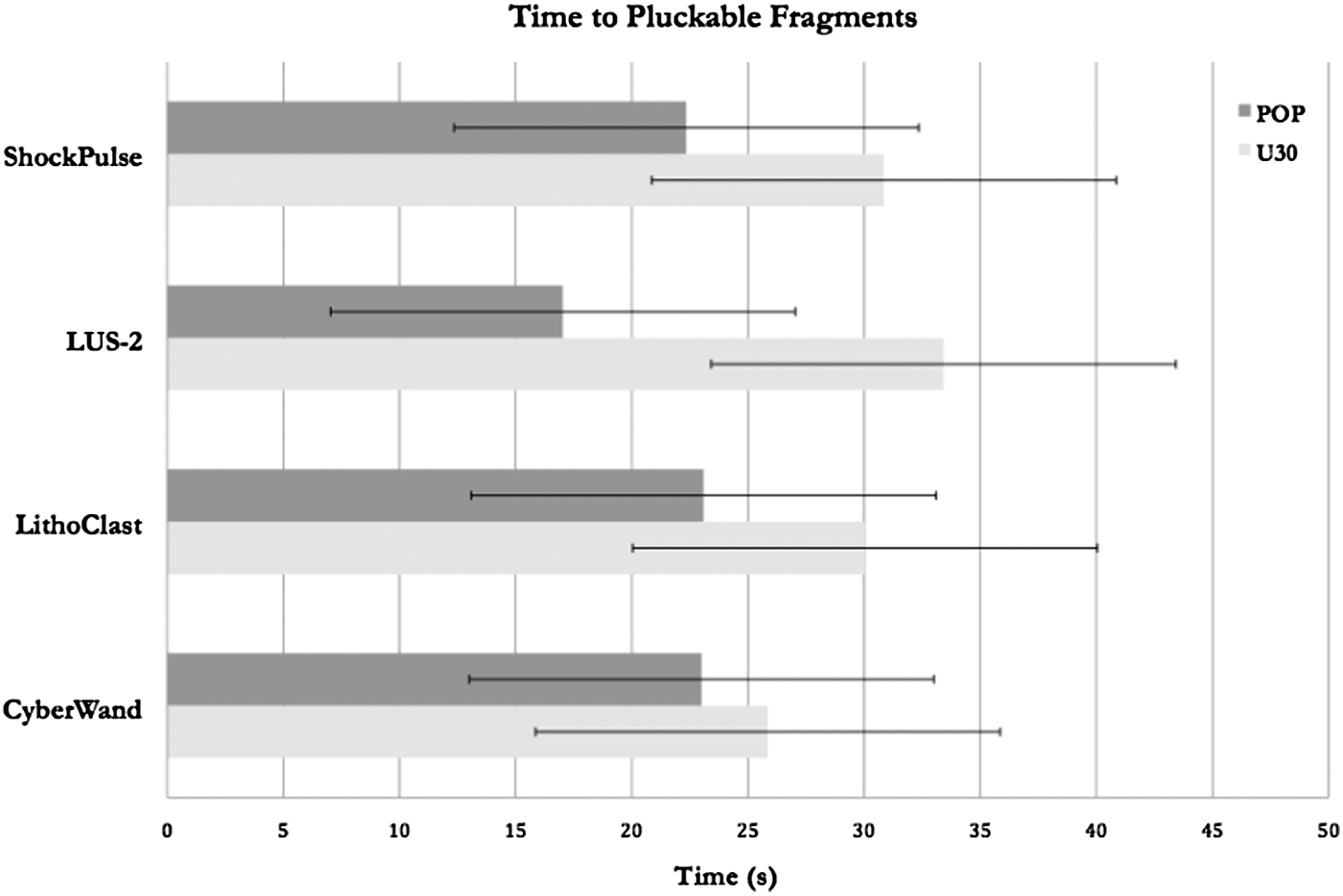
Time to retrievable fragments.
Free mass removal
Using U30 stones, the ShockPulse achieved the greatest free mass removal rate at 45.1 seconds/g. For POP stones, the ShockPulse system also had the greatest free mass removal rate at 32.9 seconds/g. For both hard and soft stones, the ShockPulse, LUS-2, and LithoClast systems performed significantly better than the CyberWand (p < 0.0001). When further compared with just the LUS-2 and LithoClast systems, the ShockPulse was still significantly faster (p = 0.046; Fig. 6).
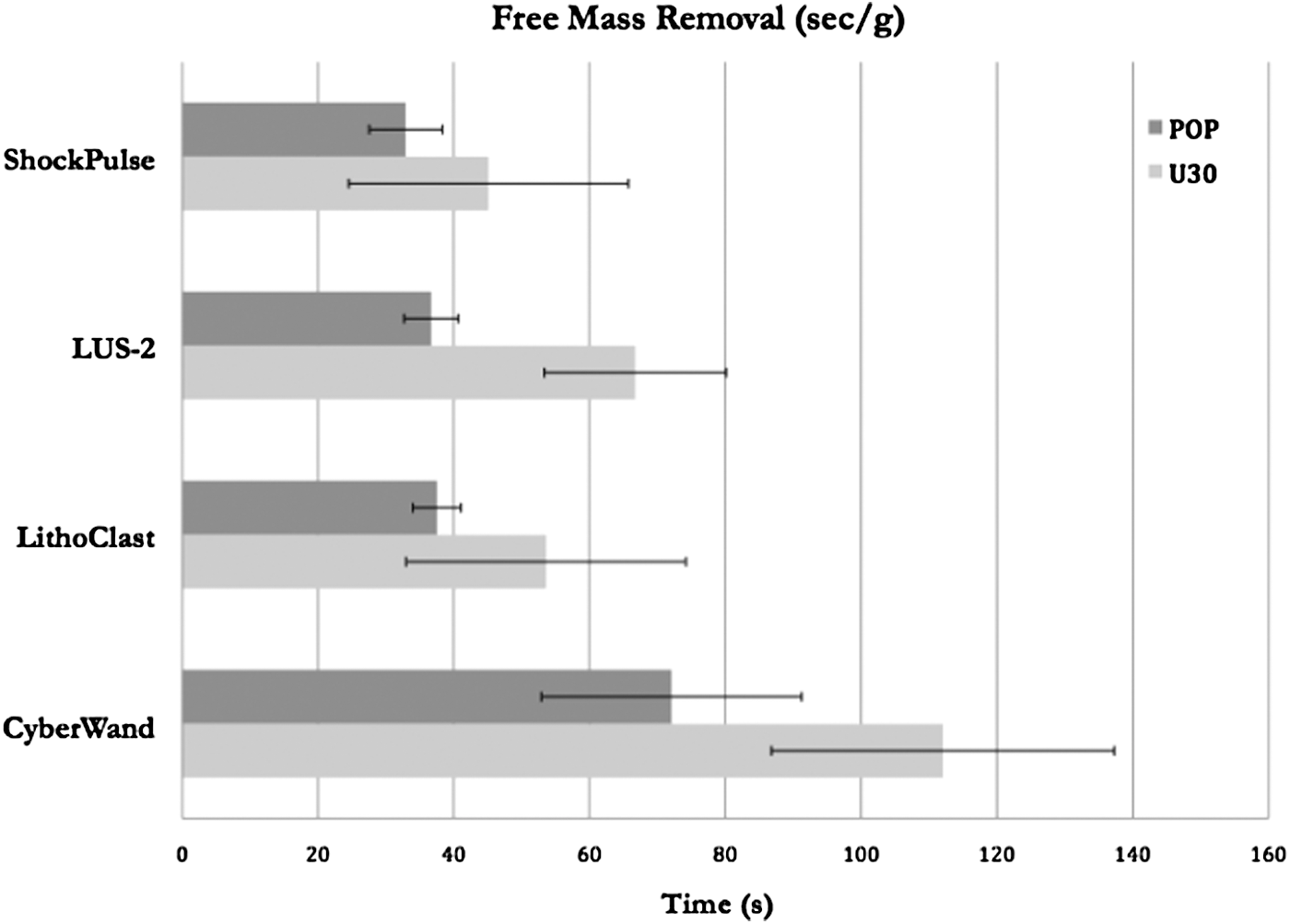
Free mass removal.
Fixed force testing
When fixed force testing was applied to a single solid U30 stone, the ShockPulse and CyberWand systems were significantly faster at all forces than the LithoClast and LUS-2 (p < 0.0001). Interestingly, the LUS-2 was unable to fully penetrate at 1.0 or 2.0 pounds of fixed force, but could do so at 1.5 lb, suggesting that this is the optimal pressure needed to fragment large calculi (Fig. 7).
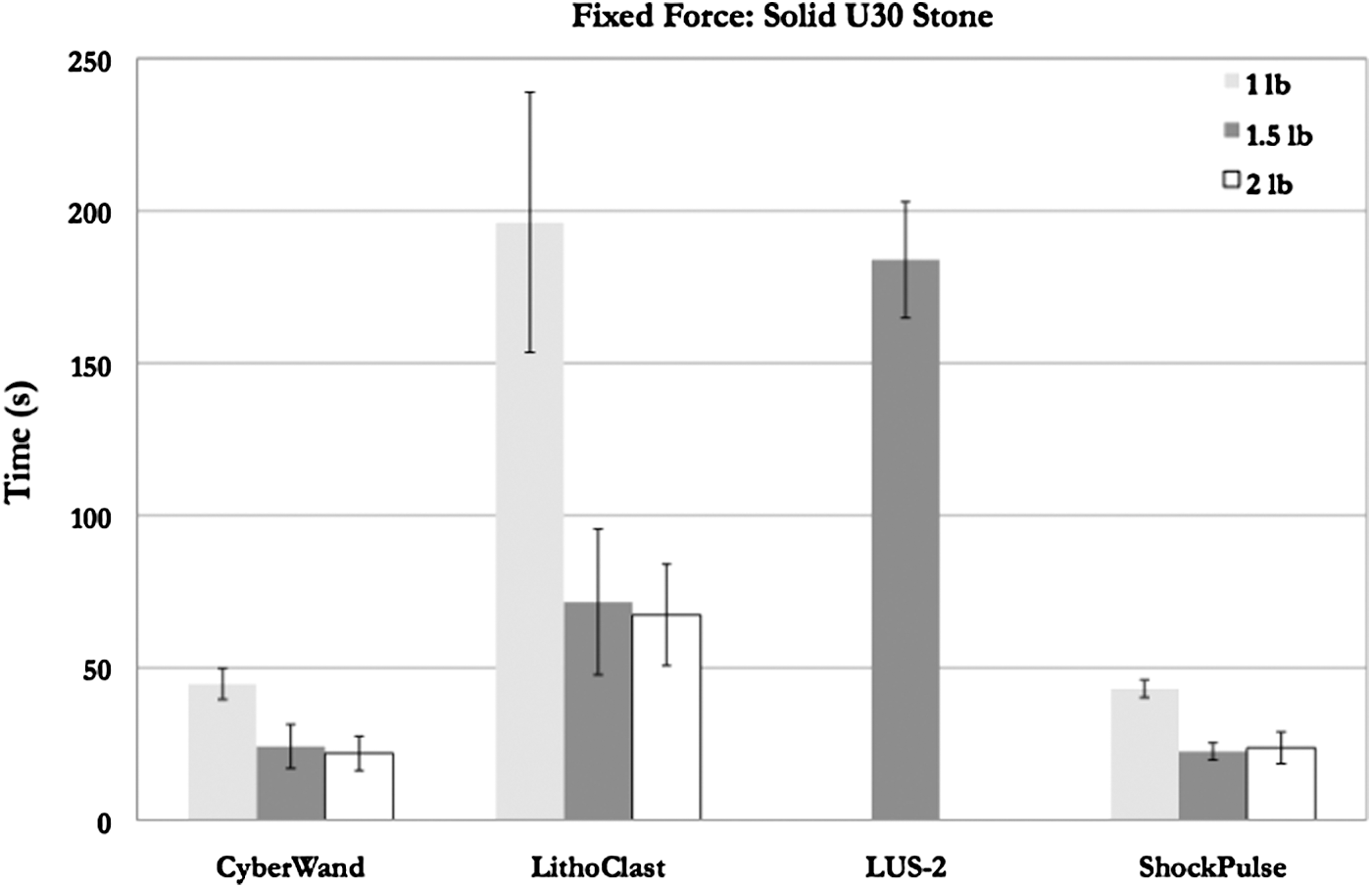
Fixed force testing applied to a single solid U30 stone. U30 = Ultracal-30.
When fixed forces were applied to the six smaller U30 stone fragments, the ShockPulse was significantly faster than all other systems at 1.0 (p < 0.001) and 1.5 pounds (p < 0.002). At two pounds, no significant differences were observed between any of the systems (p = 0.09; Fig. 8).
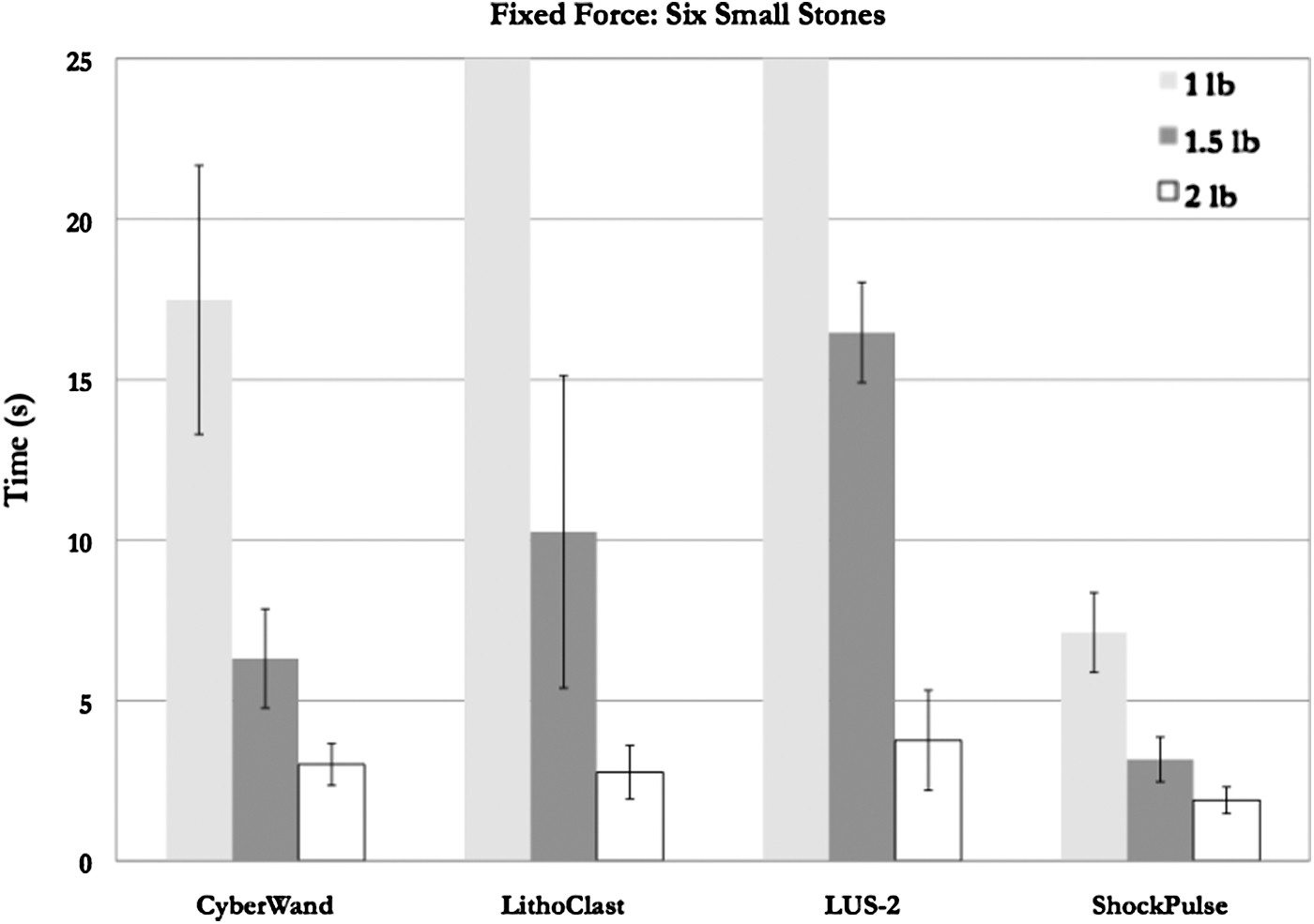
Fixed force testing applied to six smaller U30 stone fragments.
Clinical experience
In the six patients involved in the clinical testing of the ShockPulse, three underwent a left-sided PCNL and three had a right-sided procedure. Mean body mass index was 25.0 ± 3.2 kg/m2—typical of most patients we treat. Stone surface area was 415 ± 177 mm2 and a stone-free rate of 83.3% (5/6) was achieved, which was determined with a computed tomography scan performed on postoperative day 1. For the only patient in whom stone-free status was not achieved, a single residual uric acid fragment was identified in the calix adjacent to the original nephrostomy site. No complications were encountered during this trial.
Serum electrolytes and a complete blood count were drawn on all patients on postoperative day 1. The mean postoperative changes in creatinine and hemoglobin were +2.7 ± 7 umol/L and 17.3 ± 7.4 g/L, respectively. There was no need for additional perioperative intervention, blood product transfusions, or nonurological consultation.
No difficulties were encountered during the clinical testing of the ShockPulse system. The hand-activated suction helped refine the ergonomics of the operative floor space, and intraoperatively, only gentle pressure was needed to fragment stones, similar to what was observed in vitro. The ShockPulse was also effective at evacuating stone fragments, debris, and blood clots from the collecting system. Additionally, operating room staff observed significant noise reduction compared with the CyberWand.
Discussion
For over 30 years, ultrasonic and pneumatic intracorporeal lithotripters have been favored for percutaneous nephrolithotripsy. Ultrasonic lithotripters, although relatively inefficient at fragmenting hard stones, provide the advantage of concurrent suction, often eliminating the need for manual endoscopic extraction. Conversely, pneumatic lithotripters, which are not typically equipped with suction control, have proven superior at fragmenting stones of all consistencies. 7 However, subsequent retrieval of fragments can prove to be both tedious and time-consuming.
Ultrasonic lithotripters employ a piezoelectric transducer, which generates high-frequency oscillations that create energy, which is transmitted to the stone, causing fragmentation without damaging surrounding tissues. 8 Pneumatic technology, on the other hand, utilizes compressed gas to actuate a probe at a defined frequency. 9 This creates a jackhammer effect, causing stone fragmentation. Unlike ultrasonic lithotripters, pneumatic probes are not equipped with concurrent suction and have been criticized in this regard. 7
More recently, ultrasonic and pneumatic technologies have been blended into single devices. By selectively incorporating the most desired features of each modality, these combination systems have helped to maximize procedural efficiency. 1 In vitro and clinical experiments have found these devices to be equally as effective and, in some cases, even more effective than any one modality alone. 1,10,11 Simultaneous vacuum suction, as is commonplace with most ultrasonic probes, is available in dual-technology devices. The advent of combination lithotripters has garnered an ongoing interest in the field of lithotripsy technology and product development, and as such, these devices are continuously being refined. Since their introduction over a decade ago, these devices have been tested and compared with unimodal systems, demonstrating equivocal or even superior results.
In this study, we tested the newly developed ShockPulse combination lithotripter, which we found to perform equally well and, in some cases, even better than the LUS-2, LithoClast, and CyberWand systems in vitro. Of note, the ShockPulse was significantly faster than all systems at fragmenting stone phantoms at 1.0 and 1.5 pounds of fixed force. When tested in six patients at our institution, the operating surgeon noted that the device was both easy to use and ergonomically adept.
Olbert and colleagues 12 were one of the first to describe the efficacy of combined ultrasonic and pneumatic lithotripsy probes when they published their experience with the LithoClast Master in 2003. This device was tested against ultrasonic and pneumatic systems and was found to provide superior stone fragmentation rates. Similarly designed in vitro studies at that time consolidated these findings. 11,13 In addition to in vitro efficiency, clinical application proved safe for clinical use. 14,15
Shortly thereafter, Boston Scientific introduced the LithoClast Ultra. In vitro testing by Pietrow at al. 16 compared this combination lithotripter with the LUS-2. Just as prior studies had demonstrated, significantly faster stone clearance rates were observed with the combination device (39.5 mm2/minutes vs 16.8 mm2/minutes). In our study, however, no difference was observed between the LUS-2 and the EMS LithoClast for free mass removal. As for the ShockPulse, although greater total free mass removal was observed (Fig. 5), this difference was not significant.
Several years later in 2007, ACMI introduced the CyberWand. Kim and colleagues 17 compared the CyberWand with the LithoClast Ultra, which was widely accepted as one of the most efficient systems at the time. In this study, standardized gypsum stones were sandwiched between the lithotripter probe and a 63.4 g fixed weight, which provided constant force between the probe and the stone. In this study, the CyberWand achieved significantly faster penetration rates than the LithoClast. A similar study by Goldman and colleagues 18 compared the CyberWand and LithoClast at various fixed forces. Forces of 400, 1000, and 2000 g were applied. In all scenarios, the CyberWand outperformed the LithoClast. Fixed force testing in our study yielded comparable results. When forces of 1.0, 1.5, and 2.0 pounds were applied to a large stone phantom, we similarly found the CyberWand to be significantly faster at stone fragmentation than the LithoClast. Interestingly, despite superior rates of stone fragmentation, the CyberWand was significantly slower at free mass removal. This may be attributed to the concentric design of the probe, which affords a relatively small 2.77-mm lumen. Although this design optimizes stone fragmentation, it may impede aspiration.
In our study, we aimed to perform unbiased in vitro testing of the new ShockPulse system by ensuring that all participating surgeons were competently familiar with the functionality and nuances of the LUS-2, CyberWand, EMS LithoClast, and ShockPulse systems before testing to minimize confounding. Additionally, the use of the hands-free apparatus eliminated the potential for operator bias. To date, the performance of the ShockPulse system has not yet been compared with other systems.
Based on the results of our in vitro experiments, we can conclude that the ShockPulse system is equally as effective as the three lithotripters against which it was tested, and in some regards, perhaps even more effective. In our six-patient clinical experience, no intraoperative complications were encountered. This device was easy to use and the hand-activated suction control was an effective addition.
Given the nature of this study, it was not possible to blind surgeons to the devices used. Consequently, it is possible for operator bias to have been introduced. Since the fixed force component of the study was conducted in a hands-free manner, this eliminated any possibility of operator bias during this component of the study. However, by eliminating operator influence, this may have limited the clinical applicability of the study when we consider that intraoperatively, the degree of applied pressure is dynamic. The hands-free apparatus also eliminated any possibility of probe rotation, which is a frequently utilized technique during intracorporeal lithotripsy. Consequently, this may limit clinical applicability to some degree.
Conclusions
Our in vitro results found the new ShockPulse intracorporeal lithotripter to be equally as effective and, in certain aspects, even more effective than three commonly used devices. The ultrasonic/pneumatic design of this device, along with an enlarged probe lumen and hand-activated suction, serves to optimize efficiency, which may account for our positive results. In our clinical component, the ShockPulse was found to be ergonomically adept while providing excellent stone clearance. However, the efficiency displayed in our in vitro experiments will next have to be tested against other modalities in a clinical setting.
Footnotes
Author Disclosure Statement
No competing financial interests exist.