
Abstract
Objective:
To determine trends in pyelolithotomy, evaluate risk factors for complications, and evaluate the difference in outcomes and charges between open and minimally invasive (MI) techniques.
Patients and Methods:
We used the Nationwide Inpatient Sample to identify patients with a diagnosis of having nephrolithiasis undergoing pyelolithotomy from 2008 to 2012. Total charges were inflation-adjusted to U.S. dollars in 2012. Patient demographics, hospital characteristics, and outcomes were reported and compared between open and MI groups after survey weighting.
Results:
We included a survey-weighted population of 17,294 patients, of whom 841 (4.9%) had MI pyelolithotomy. The proportion of MI cases increased by 2.57% annually (r 2 = 0.921, p = 0.01), although total pyelolithotomy cases remained stable. Simultaneous pyeloplasty occurred in 6.6% of all patients. Patients receiving open surgery experienced longer length of stay (3.9 days vs 2.7 days; p < 0.001), but accrued equivalent inflation-adjusted charges ($49,588 ± 2088 vs $51,716 ± 4893; p = 0.665). On multivariable analysis, higher Elixhauser comorbidity index and presence of any genitourinary anomaly were associated with experiencing a complication, while undergoing surgery at a top quartile hospital and elective admission status were protective against complications. MI technique and simultaneous ureteropelvic junction repair did not alter complication risk.
Conclusion:
While the annual number of pyelolithotomy cases was stable, there was an increasing trend toward MI technique. Both patient and hospital factors can significantly alter the risk for complications following pyelolithotomy.
Introduction
T
A recent study of upper tract stone cases revealed that from 1999 to 2009, pyelolithotomy cases declined, while nephrolithotomy cases increased. 1 However, this study did not describe the patient characteristics of those undergoing these procedures, such as aberrant anatomy and requirement of additional genitourinary tract procedures. The objective of this study was to determine current trends in pyelolithotomy and nephrolithotomy cases and elucidate patient and procedural characteristics to see if practitioners are truly following recommendations about appropriate patient selection. We also sought to identify patient and hospital risk factors for the development of in-hospital complications.
Patients and Methods
We queried the Healthcare Cost and Utilization Project (HCUP) Nationwide Inpatient Sample (NIS) 8 to identify male and female adult patients undergoing pyelolithotomy from 2008 to 2012. International Classification of Disease, Ninth Edition (ICD-9), coding for robotic procedures was not available before 2008. The NIS is a prospectively maintained national database of participating hospitals that contains discharge information on patients, including as many as 25 patient diagnoses as well as 15 patient procedures performed during admission. Patient and hospital factors are collected, as well as complications and charges up to discharge. 8 The HCUP provides weighting to all demographic variables, and a discharge weight is calculated for each hospital. Weighted patient estimates for each discharge are then applied for analysis. ICD-9 and clinical classification codes used are provided in Supplementary Table S1.
Patients were included if their age was ≥18 years, they had a diagnosis of renal calculus (ICD-9 code 592.0), and they had a procedure code for pyelolithotomy. Pyelolithotomy included both nephrotomy and pyelotomy ICD-9 procedure codes (55.01 and 55.11, respectively) as previously used in this database, 1 and MI pyelolithotomy was specified by the addition of codes for laparoscopic and robotic approaches. The year 2008 was chosen as the first year of study because this was the first year with codes to specify robotic technique. Patients needed both a diagnosis of renal calculus and a procedural code for pyelolithotomy for inclusion. ICD-9 and Clinical Classification Codes (available through the NIS 8 ) also identified patients who underwent pyeloplasty and had any genitourinary anomaly. Furthermore, specific diagnoses of ureteropelvic junction (UPJ) obstruction and horseshoe, ectopic, or fused kidneys were identified. Patient and hospital variables analyzed included race, age, Elixhauser comorbidity index, primary insurance payer, hospital location and teaching status, hospital region, simultaneous pyeloplasty performed, and whether the procedure was performed in an MI manner. Hospital volume quartiles were created based on the survey-weighted annual number of pyelolithotomies performed at each facility.
We then analyzed the following patient outcomes and compared them between open and MI groups: median length of stay (in days), median total charges (U.S. dollars adjusted for inflation to 2012 value 9 ), patient disposition, receipt of blood transfusion, and complications during the hospitalization through discharge. Patient disposition describes the location to which the patient was discharged. Next, we developed a multivariable logistic regression model to identify independent predictors for development of any complication. We finally evaluated trends in the annual number of all pyelolithotomies performed and compared them between open and MI groups.
All statistical analyses were performed using STATA 14.0 (Statacorp, College Station, TX). Continuous variables were performed using Student's t-test with the Wald correction, and categorical variables were compared using a chi-squared test with the Rao–Scott correction. Multivariable logistic regression was used to correlate factors predictive of any complication. Temporal trends were analyzed with linear regression modeling. All tests were two-sided with statistical significance defined as p-value <0.05.
Results
We included a survey-weighted cohort of 17,294 patients who underwent pyelolithotomy from 2008 to 2012, of whom 841 (4.9%) had their procedure performed by MI techniques (Table 1). Both groups had a similar gender distribution (54.8% female in the open group vs 54.5% in the MI group; p = 0.916). Mean age and race were statistically similar between both groups. Patients in the MI group had a higher proportion of individuals with an Elixhauser comorbidity index of 0 (49.8% vs 32.9%; p = 0.002), whereas the open group had a larger proportion with a score of 1 or more. The majority of operations occurred at urban hospitals with both groups having the largest proportions in urban teaching facilities, but there was an overall similar distribution between groups. There was a difference, however, in distribution of operations performed at each hospital per volume quartile between the groups. There was also a difference between groups in the distribution of cases by hospital region. A much larger proportion of patients in the MI group underwent simultaneous pyeloplasty (67.2% vs 3.5%; p < 0.001). The majority of admissions were elective, although there was a larger proportion of elective cases (92.3% vs 81.4%; p = 0.001) in the MI group. Patients in the MI group more commonly had a genitourinary anomaly (25.7% vs 6.6%; p < 0.001), including UPJ obstruction (12.2% vs 2.8%; p < 0.001) and a diagnosis of horseshoe, ectopic, or fused kidney (5.2% vs 2.2%; p = 0.036).
NIS guidelines do not permit reporting of cell numbers ≤10, so complications with these values were grouped as other.
A survey weighted 16,393 of the 16,452 patients in the open group who had known elective vs nonelective admission status, leaving 59 patients with unknown admission status; all 841 patients in the MI group had known admission status.
HMO = health maintenance organization; MI = minimally invasive; SE = standard error of the mean; UPJ = ureteropelvic junction.
Table 2 compares outcomes between open and MI groups. The open cohort had a significantly longer length of stay (3.9 days vs 2.7 days; p < 0.001), but there was no difference in mean total adjusted charges between groups ($49,588 in open vs $51,716 in MI groups; p = 0.665). There was also no difference in the distribution of patient disposition between groups, with a similar proportion (p = 0.069) of patients in open and MI groups being discharged home (86.1% vs 94.6%, respectively), to home health (8.4% vs 3.9%, respectively), and collectively to either a short-term hospital, a skilled nursing facility, against medical advice, or other (5.4% vs 1.5%, respectively). The NIS does not permit reporting of survey-weighted patient groups ≤10 patients, so several disposition categories within the disposition and complication sections were grouped together for reporting and analysis. Survey-weighted complications, 2066, were reported in the entire cohort. The open group had survey-weighted deaths, 29, whereas no deaths occurred in the MI group. Patients from both groups had similar statistical likelihood of receiving a blood transfusion (7.0% and 3.2%; p = 0.109), although there was a trend toward higher percentage of patients experiencing bleeding complications in the open group (8.6% vs 3.8%; p = 0.067). Similarly, there was a trend toward a lower percentage of patients experiencing any complication (12.2% vs 6.5%; p = 0.058) in the MI group.
NIS guidelines do not permit reporting of survey-weighted patient counts ≤10. Disposition groups with ≤10 members were all analyzed in one consortium. Complication groups ≤10 members were grouped as Other.
Other complication includes intraoperative, gastrointestinal, respiratory, urinary, cardiac, infection, vascular, wound, seroma, and additional unspecified complications. Any complication includes deaths as well as Bleeding and Other groups.
SNF = skilled nursing facility.
Table 3 provides a multivariable analysis for predictors of development of any complication after pyelolithotomy. When controlling for age, sex, and race, we found that higher Elixhauser comorbidity index (odds ratio [OR] 1.32; 95% confidence interval [CI] 1.21, 1.45; p < 0.001) and having any genitourinary anomaly (OR 1.71; 95% CI 1.05, 2.77; p = 0.031) increased patient odds of development of any complication. On the other hand, patients having surgery at a hospital in the top quartile of case volume (OR 0.59; 95% CI 0.39, 0.88; p = 0.11) and elective admission (OR 0.70; 95% CI 0.49, 0.99; p = 0.043) were protective against complications. Of note, simultaneous pyeloplasty and MI technique were not associated with a change in complication risk.
CI = confidence interval; HMO = health maintenance organization; REF = reference group.
Figure 1 depicts trends in the percentage of annual cases performed for both open and MI pyelolithotomy. The annual number of total pyelolithotomy cases did not significantly change over the study period (β = −485.5, r 2 = 0.568, p = 0.141). However, the percentage of MI cases significantly increased during this time (β = 2.57, r 2 = 0.921, p = 0.010).
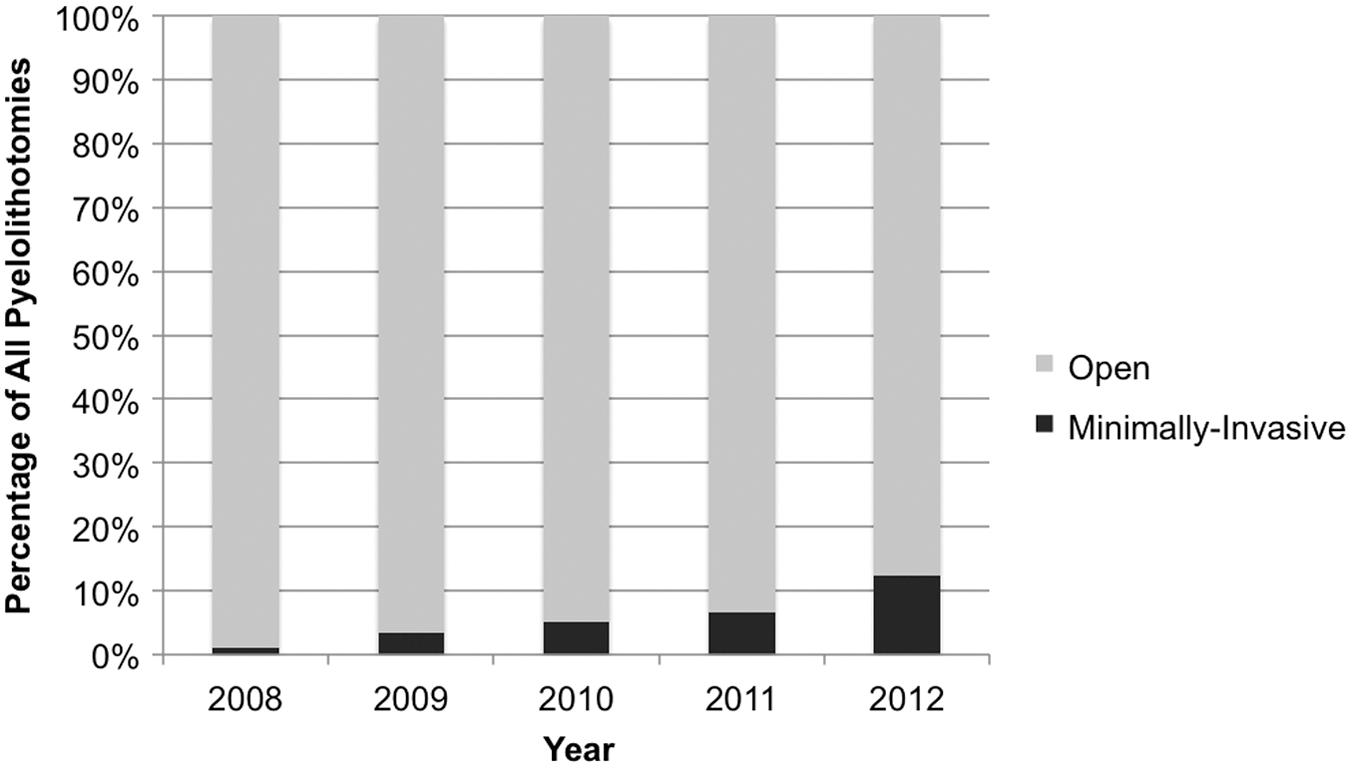
Percentage of open and minimally invasive pyelolithotomies performed annually.
Discussion
While the majority of upper urinary tract calculi are managed endoscopically or with SWL, 1 pyelolithotomy remains an option in patients with concomitant UPJ obstruction and in patients who are otherwise not candidates for less invasive techniques. 5,10,11 In the present study, we observed that the overall number of pyelolithotomy cases was stable over the 2008 to 2012 time period, although more recently a higher proportion of cases was performed in an MI manner. We also observed that MI pyelolithotomy is associated with a shorter hospital stay, although with equivalent accrued charges.
For many urologic procedures, the MI approach using laparoscopy with or without robotic assistance can allow patients such benefits as shorter length of stay, fewer complications, and reduced narcotic pain requirement, 12,13 but they are not always cost-effective. 14 –17 A study by Leow and colleagues 18 recently demonstrated that direct hospital costs associated with the use of the robotic platform during radical prostatectomy were significantly higher than with the open technique (U.S. $4528 more per case) across the board. However, high-volume surgeons and high-volume centers had equivalent costs between the open and robotic prostatectomies, suggesting that a more streamlined approach is feasible. Delto and colleagues 17 compared instruments used for robotic prostatectomy between surgeons at their single institution and identified which expensive instruments could be replaced by less expensive tools, cutting direct costs by 42% for one surgeon. The patients in this study undergoing MI pyelolithotomy accrued similar charges to those undergoing open surgery, which may be due to higher equipment costs associated with laparoscopic and robotic equipment given that the patients in the open group stayed for a mean of 1.2 days longer. With the infrequent use of this procedure compared with others such as robotic radical prostatectomy, surgeons on average may have more variability in technique and equipment used. In spite of potential variability in technique, the MI approach was not independently associated with a change in risk for complications in this study, and the risk of any complication was comparable with prior studies. 6,19,20 However, the data in this study trend toward fewer total and bleeding complications in the MI group. Furthermore, surgery at a high-volume center (fourth quartile) was independently associated with a lower complication risk in the present study, which would be expected.
In addition to financial concerns, the invasiveness of pyelolithotomy may reduce its desirability for practitioners and patients. Several studies have demonstrated longer operative time and length of stay with laparoscopic pyelolithotomy and nephrolithotomy compared with PCNL in patients with stones >20 to 30 mm. 2,20 –22 Interestingly, however, a meta-analysis of seven studies comparing laparoscopic pyelolithotomy to PCNL demonstrated an average 51-minute shorter operative time, 0.66-day shorter length of stay, smaller hemoglobin decline, and less postoperative fever in the pyelolithotomy group. 3 Taken together, the data suggest that nephrolithotomy and pyelolithotomy may be safe in appropriately selected patients. Nevertheless, patient selection criteria have yet to be based on level I evidence. 2 Current indications for pyelolithotomy and nephrolithotomy include aberrant genitourinary anatomy such as an ectopic kidney, stone located in an anterior caliceal diverticulum, and simultaneous pyeloplasty. 2,11 While a high proportion (67.2%) of patients in the MI group of this study underwent simultaneous pyeloplasty, only 3.5% of patients in the open group underwent this procedure. Similarly, less than 10% of patients in the open group had a documented genitourinary anomaly. Based on these data, it appears that a much larger percentage of patients undergoing MI pyelolithotomy have characteristics for which this procedure is recommended. This study assessed simultaneous pyeloplasty, but patients may be undergoing additional procedures outside of the genitourinary tract. Additionally, this database is unable to provide information concerning any previous procedures that may have been performed for the same stone. Future investigation regarding prior procedures and the need for repeat procedures could elicit additional information regarding the current state of practice as well as potential differences in outcomes.
We found that having any genitourinary anomaly (which included patients with ectopic kidney) was associated with a higher risk of complications, although simultaneous pyeloplasty was not associated with a higher rate of complications. Certain complex anatomic abnormalities may increase the technical difficulty of the procedure, although pyeloplasty is a surgery with which more urologists may be familiar. Another factor in patient selection not well described is patient comorbidity, 23 and in the present study, we demonstrated that higher Elixhauser comorbidity was independently associated with any complication. Patients with abnormal urinary tract anatomy and more comorbidities should be counseled appropriately before undergoing the procedure that they may be at higher risk of having a complication.
This study does have limitations, including the retrospective nature of data review. In addition, this study relies on accurate coding for procedures and diagnoses, especially in patients undergoing multiple procedures during a single operation. Prior procedures and patient follow-up are not recorded in this database. Prior procedures for stones may impact surgical planning and operative choice, which would be interesting to evaluate in addition to long-term outcomes. The type of stone is unable to be assessed in all patients in this database and could potentially impact patient outcomes, particularly in those with infectious stones. Genitourinary abnormalities may have been suspected based on preoperative imaging, but not noted by the diagnosis code. Additionally, unmeasured patient and procedural factors may have not been captured, which could explain complication rates.
Conclusions
In summary, over the time period of 2008 to 2012, rates of open and MI pyelolithotomy did not significantly change. While open surgery resulted in a longer length of stay, it did not impact the complication rate. Furthermore, patients undergoing simultaneous pyeloplasty did not have an increased risk of complications. Patients with higher Elixhauser comorbidity index and any genitourinary anomaly undergoing pyelolithotomy should be counseled that they are at higher risk of any complication. In contrast, patients at high-volume centers and those admitted electively to the hospital are at lower risk of any complication. Patients should also be counseled that undergoing simultaneous pyeloplasty does not appear to lead to an additional risk of complications.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.