
Abstract
Introduction:
We sought to determine the rate of and factors associated with patient nonadherence to prescribed follow-up after uncomplicated ureteroscopy.
Materials and Methods:
The records of 247 consecutive patients who underwent ureteroscopy at a tertiary referral center from November 2010 to February 2016 were reviewed. Bivariate and multivariate analyses were performed to determine the impact of demographic, procedural, socioeconomic, and environmental factors on the rate of compliance with secondary prevention counseling.
Results:
Forty-five patients (18.5%) were lost to scheduled follow-up for secondary prevention counseling after ureteroscopy. Lost to counseling rates were broad based and not associated with traditional predictors of poor follow-up such as age, gender, marital status, and distance traveled. On multivariate analysis, compared with those using commercial insurance, patients with Medicare (odds ratio [OR] for follow-up 0.48, 95% confidence interval [CI] 0.21, 1.1 p = 0.095) and Medicaid (OR for follow-up 0.25, 95% CI 0.1, 0.6, p < 0.001) were less likely to be adherent to prescribed follow-up.
Conclusions:
Nearly one in five patients will be lost to follow-up for secondary prevention counseling after ureteroscopy. Lack of follow-up may prevent the diagnosis of postoperative complications and limit the ability to counsel patients on stone prevention. Efforts to improve follow-up following ureteroscopy should focus on including more postoperative counseling in the preoperative period and a more individualized approach to specific patient populations, particularly those with a lower socioeconomic status.
Introduction
I
In clinical practice, 20%–34% of patients who undergo ureteroscopy are lost to follow-up 4 –6 and therefore not offered the opportunity for routine postoperative imaging or preventative interventions. Current literature regarding follow-up is difficult to interpret as many prospective studies report excellent follow-up within their prospective study protocol and most retrospective studies examining outcomes exclude patients without available follow-up data. Prior studies in psychiatric and medicine patients have identified multiple patient, practice, and physician factors, which lead to poor follow-up. 7,8 Stone formers, however, represent a unique patient population with both a medical and surgical disease, and reasons for being lost to secondary prevention counseling (LTC), which represents noncompliance with follow-up, have not been evaluated in this population. To evaluate the rate of and potential reasons for being LTC as well as determine how to improve the management of patients with nephrolithiasis, we reviewed our experience over 6 years at a single academic center to determine potential patient and surgical factors related to being LTC following ureteroscopy.
Materials and Methods
After obtaining IRB approval, we identified all patients undergoing uncomplicated ureteroscopy for nephrolithiasis from November 2010 through February 2016 by a single fellowship-trained endourologist (C.R.T.). Patient counseling and follow-up were standardized for these patients. All patients received verbal preoperative counseling regarding the importance of follow-up to monitor for procedure-related outcomes such as silent hydronephrosis and residual stone burden and to discuss secondary prevention of stone recurrence. All patients with a stent with an extraction string and patients who undergo cystoscopic stent removal are scheduled for follow-up 6 weeks after stent removal with an ultrasound, kidney, ureter, and bladder radiograph and for prevention counseling, including review of 24-hour urine collection, stone composition analysis, and serum blood chemistries. All patients receive an appointment for follow-up before discharge after surgery as well as a letter at least 10 days before follow-up. All patients who do not follow-up are contacted by phone from the scheduling department to reschedule their missed appointment (Fig. 1). Of note, patients who were referred from a community urologist and preferred to follow-up with the community urologist were not included in the study (n = 6).
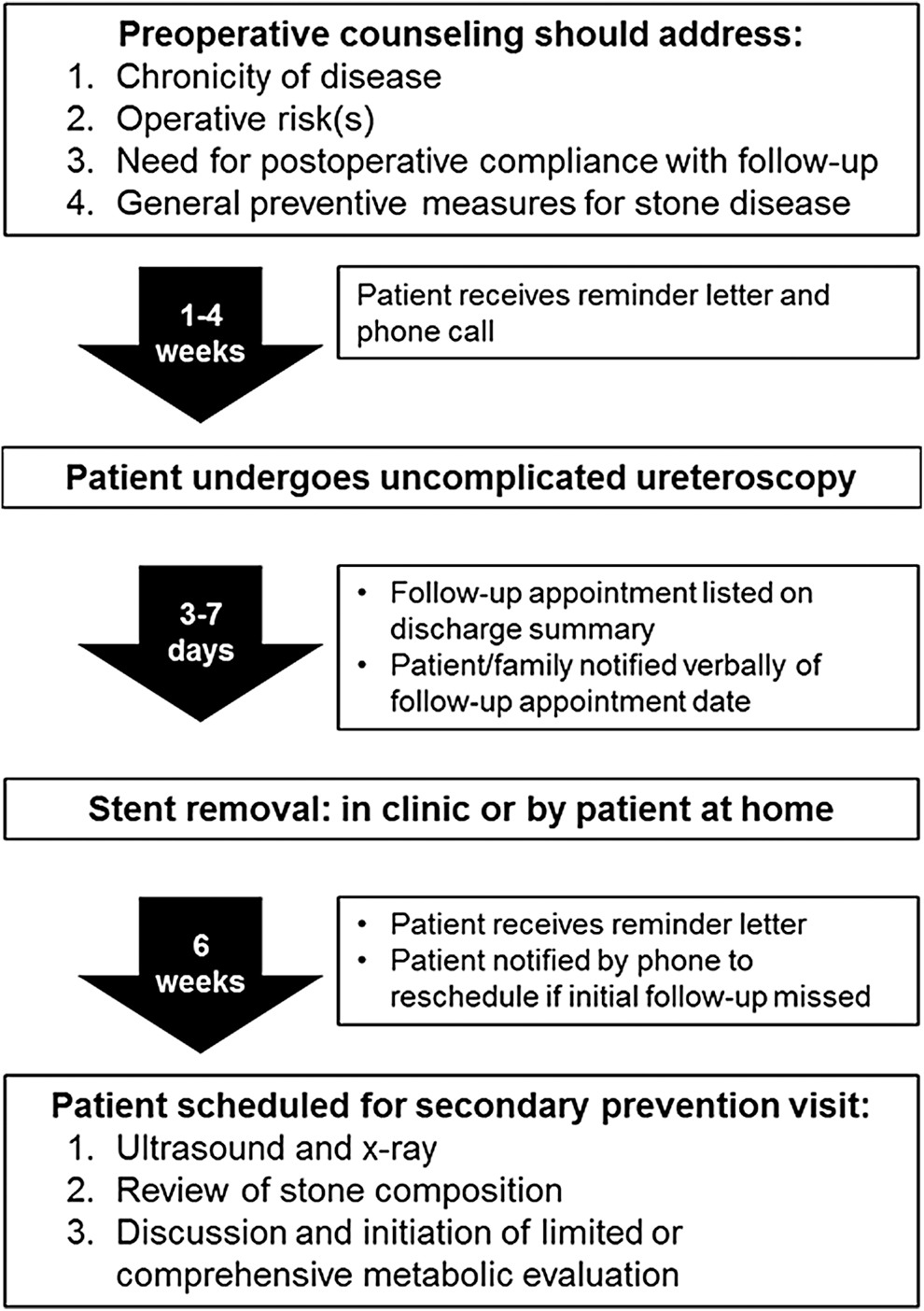
Standardized patient throughput from preoperative counseling through secondary prevention appointment.
Patients were included if they were at least 30 days from their first scheduled follow-up appointment. Uncomplicated ureteroscopy was defined as unilateral ureteroscopy in patients without solitary kidneys, anatomic abnormalities, or ureteral injuries. For patients who required cystoscopic stent removal, being LTC was determined by missing their first appointment after cystoscopic removal. For those without a stent or who performed home extraction of the stent through an extraction string, LTC was defined as missing the first scheduled appointment after ureteroscopy.
To identify potential reasons for being LTC, we reviewed demographic information, patient factors, and perioperative factors. Demographic information included patient age at the time of procedure, gender, marital status, and insurance type. Distance traveled for treatment was calculated using the distance from patient's home zip code to the hospital. Patient stone-related factors included recurrent stone formation vs first stone episode, cumulative stone burden, and stone composition. Perioperative factors included intraoperative complications, ureteral access sheath use, and stent placement with or without an extraction string. Postoperative factors included all complications, as well as procedure-related events (PREs), including any patient phone call, unintended clinic visit, or emergency room visit, related to their procedure or indwelling stent within 30 days. 9
Statistical analysis was performed using SAS (version 9.4). Univariate logistic regression was repeatedly performed to assess the impact of several variables on follow-up status. Estimates obtained quantify the log odds of a patient following up for a 1 U increase in a continuous variable or compared with the reference in a categorical variable. The 95% confidence intervals (CIs) and p-values were also calculated to determine the significance of the variable's impact on follow-up status. Odds ratios (ORs) were determined by reverse log transformation of the estimate.
Multivariate analysis was performed using the candidate collection of predictors; we modeled all possible subsets to determine the best variables to use in a multivariate model. We identified the most suitable predictor set using the Akaike information criterion (AIC). Model development was limited to a maximum of 3–4 variables based on the number of patients who did not follow-up. However, the final model with the predictors age, gender, and insurance had AIC within 2 U of the minimum, making it our model of interest.
Results
Of 247 patients (114 men and 133 women) who underwent uncomplicated ureteroscopy, 45 (18.5%) were LTC. The LTC rate was similar across nearly every category (Table 1). LTC patients tended to be younger (mean age 49.0 vs 53.2 years, p = 0.098) and had less stone burden when compared with those patients who were not LTC; however, these differences were not significant. In addition, neither gender, comorbidity as measured by the American Society of Anesthesiologists (ASA) score, marital status, PREs, stenting with an extraction string, or recurrent stone episode predicted follow-up. Similarly, complications, ureteral injury, and/or PREs were not associated with being LTC. Stone composition did not affect LTC rates, although of note all patients with cystine stone composition did follow-up as advised.
The odds ratio represents that odds of being noncompliant with prescribed follow-up (LTC).
LTC = lost to secondary prevention counseling; PRE = procedure-related event.
The only significant factor associated with poor follow-up was insurance type. Compared with patients with private insurance, patients with Medicare (OR for follow-up 0.48, 95% CI 0.21, 1.1 p = 0.095) and Medicaid (OR for follow-up 0.25, 95% CI 0.1, 0.6, p < 0.001) were less likely to follow-up (Fig. 2). This remained the case after performing multivariate analysis, suggesting that having Medicaid is independently associated with LTC (Table 2).
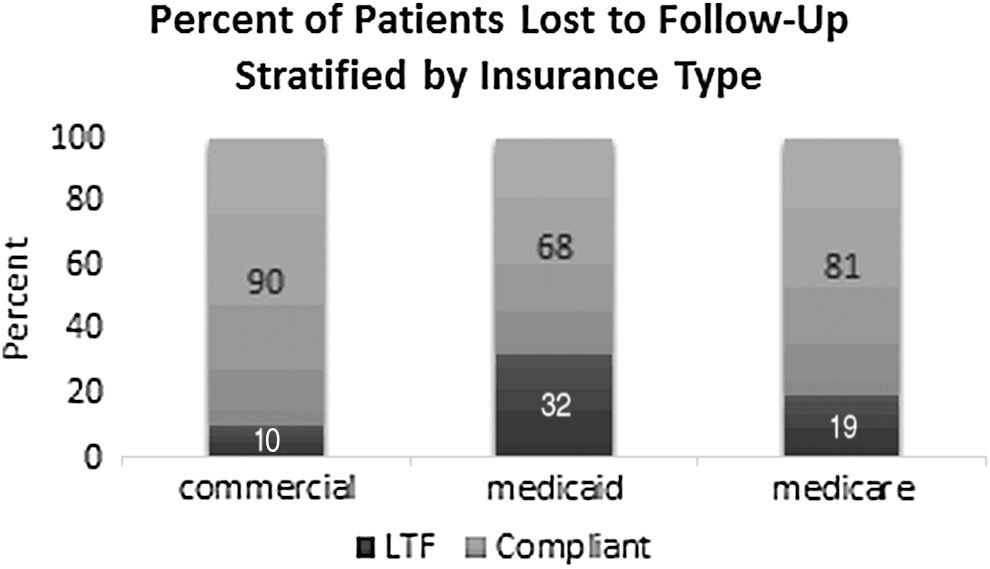
Insurance is associated with patient compliance. Compared with patients with private insurance, patients with Medicaid were significantly less likely to be compliant with follow-up. LTF = lost to follow-up.
An odds ratio <1 indicates that the patients did not comply with follow-up. Multiple multivariate models were created with the final model reflecting the impact of traditionally associated factors of age and gender on compliance. The only significant factor associated with poor compliance with follow-up remained having Medicaid as the primary payer source.
In addition to patient factors, environmental factors did not predict patient follow-up. There was no difference in follow-up patterns based on the season in which the ureteroscopy was performed or the month, although there was a trend toward poor follow-up for ureteroscopy performed in November (OR 0.240, 95% CI 0.053, 1.10, p = 0.067) (Fig. 3). Patients who lived closer also trended toward better follow-up (mean 64.3 vs 76.0 miles, p = 0.14).
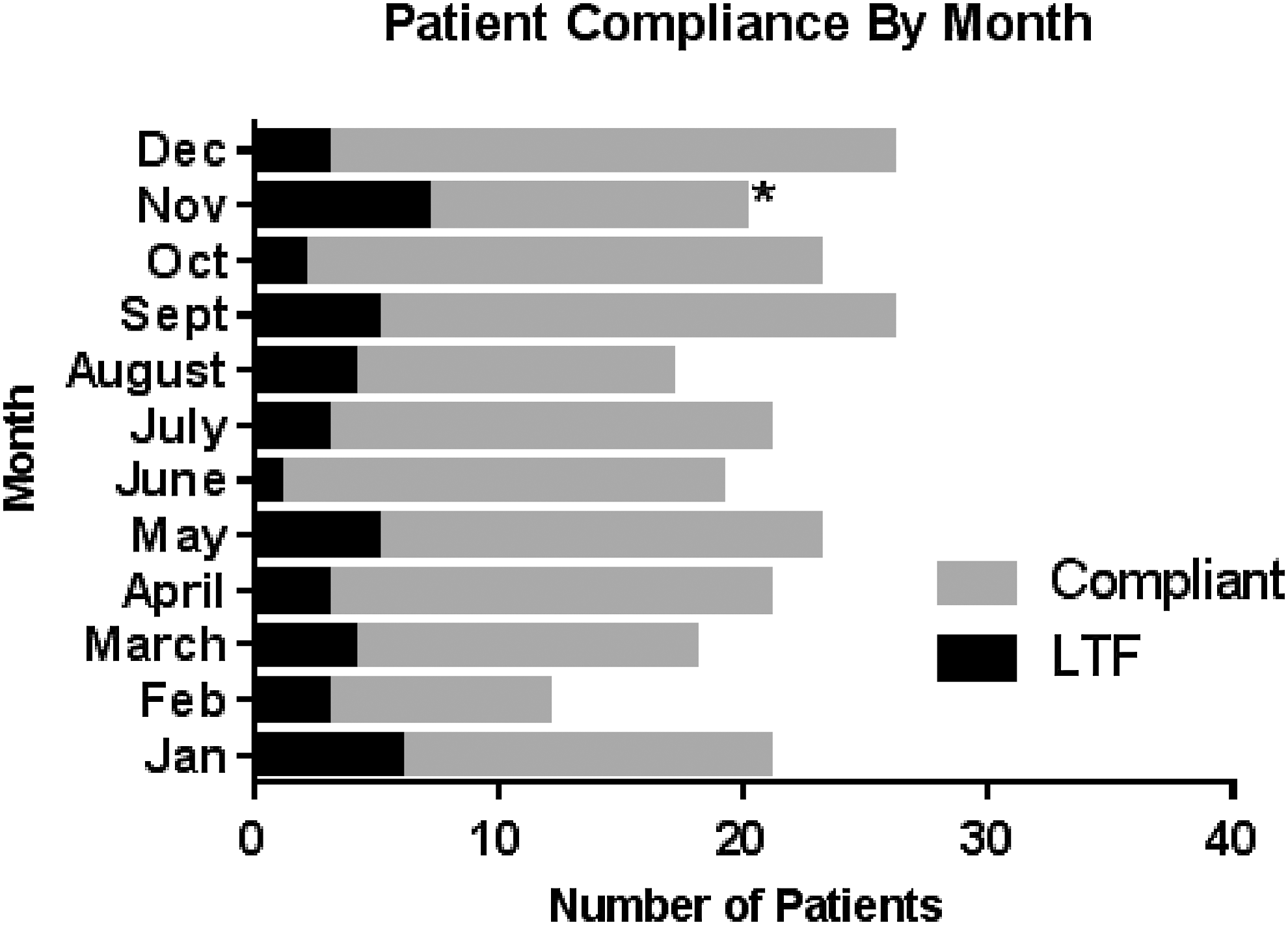
Patient compliance by month of procedure. There was a trend toward poor compliance with follow-up for procedures performed in November.
Discussion
In our cohort of 247 patients, 18.5% were lost to follow-up following routine ureteroscopy, which is similar to previously reported LTC rates. 4 LTC rates were broad based and not predicted by demographic factors, stone-related factors, or operative outcomes. Although all patients received similar preoperative and postoperative counseling, only insurance type was predictive of follow-up, with patients who had Medicaid insurance following up at about 25% the rate of patients with private insurance. Given that counseling following stone treatment, through dietary changes 10 and or medical management, 11,12 may help alleviate future stone recurrence, knowledge of factors that lead to being LTC may help develop a comprehensive plan for improving outcomes in nephrolithiasis. This is especially important as there was no difference in LTC rates between first time and recurrent stone formers.
A study by Moses et al. in patients undergoing either ureteroscopy or percutaneous nephrolithotomy demonstrated that 23% of patients were LTC. Similar to our current study, government-assisted insurance was the only significantly associated factor. 13 However, while the prior study took into account age, gender, distance, season, and education (patient factors), they did not take into account procedure and disease-related factors such as stone burden, first time vs recurrent stone formation, procedure-related events, or preoperative stenting, which we feel are strengths of our study. Prior studies from orthopedics, cardiology, and pulmonology have found that poor compliance is significantly influenced by younger age, being unmarried, longer distance traveled, and being male. 14 –17 In patients with nephrolithiasis, these traditional predictors of being LTC do not appear to apply, although there was a trend toward poor compliance among younger patients (p = 0.08) who traveled a greater distance (p = 0.15) to have their operation. Given that distance has been shown to be a factor in other diseases and that our cohort generally did travel a larger distance than would be expected, our results might not represent those seen in a more urban setting. Interestingly, patients who underwent their procedure in November tended to have worse follow-up than any other month, which has not been evaluated in prior studies. As our prescribed follow-up is typically 4–6 weeks after the procedure, increased LTC rates during this time may be secondary to the corresponding holiday season or weather-related transportation factors.
With regard to operative outcomes, patients who experienced a postoperative-related event (PRE) were slightly more likely to follow-up. However, even in patients with adverse events or ureteral injury, follow-up was not different than those without such event. This finding is of particular concern as 2%–4% of patients may have silent hydronephrosis, ureteral stricture, and obstruction after routine ureteroscopy that would only be identified on follow-up imaging. 18,19 Therefore, appropriate follow-up in this cohort may help to prevent sequela associated with ureteral obstruction, including decreased renal function, hypertension, and potential renal loss. 20 Importantly, the method of stent removal (cystoscopy vs home extraction via string) did not predict inadequate follow-up, such that the decision to leave an extraction string should not be based on concern for decreased follow-up in patients who otherwise would be candidates.
Patients with Medicaid were significantly more likely to be lost to follow-up. Although we did not have socioeconomic data, adults who receive Medicaid in Iowa have an income <138% of the federal poverty level, which is the equivalent of an annual income for a family of 4 of 33,465 for 2016, which is $ 20,000 less than the state median household income. Lower economic means along with education level and occupation compose socioeconomic status (SES), 21 suggesting that SES is an important predictor of LTC rates following ureteroscopy. Large population-based studies have demonstrated that 25% of patients with an income <200% of the federal poverty level delay or do not seek medical care. 22 Similar health disparity has been demonstrated among those with lower SES in Europe as well, suggesting that in systems with centralized social healthcare, disparities might be seen in similar populations to those patients with Medicaid in the United States of America. 23 Importantly, follow-up in this population may be even more important than the general population as impoverished patients have previously been shown to have a high rate of modifiable urine parameters for secondary prevention of nephrolithiasis. 24
The increased LTC rate among patients with a lower SES is likely driven by previously described barriers, including financial instability, resource scarcity, employment pressure, travel expense, and relationship instability. Poor patient compliance with follow-up might also represent poor adherence to prescribed management strategies in this population. 25 Any effort to improve patient follow-up should have a specific focus on this patient cohort and may require nontraditional mechanisms such as telemedicine or coordination with a local provider, not only for follow-up but also to ensure adherence to treatment as has been demonstrated in other chronic conditions. 26
Based on these findings, several interventions should be considered when counseling patients about stone disease and subsequent follow-up. Because a subset of patients will invariably not follow-up after ureteroscopy, the first area to intervene would be on the initial presentation by clearly explaining that stone disease is a chronic disease that can be managed with both dietary and medical means. Preoperative counseling should include working with patients to understand their goals of care and to determine barriers for therapy and follow-up as implementing a more personalized approach might lead to better adherence and therefore improved secondary prevention of nephrolithiasis. Additionally, risk factors for stone prevention, including dietary evaluation and a limited metabolic workup with serum electrolytes, calcium, uric acid, phosphorus, and urinalysis, should be performed at presentation with the knowledge that a small group of at-risk patients would otherwise be missed if evaluation is initiated upon follow-up. 3
Attention to improving follow-up has been given to chronic fatal illnesses such as congestive heart failure, cancer, and HIV and efforts have been implemented to improve LTC rates. 27,28 While nephrolithiasis is not generally viewed with the same severity as these diseases, it is nonetheless a chronic disease affecting over 10% of the US population and costing the healthcare system over 2.1 billion dollars per year. 29 As counseling and appropriate dietary and medical intervention have shown to decrease stone recurrence rates in actively managed patients, improved follow-up may decrease subsequent patient morbidity and associated costs to the healthcare system. 30,31
Our results represent a select cohort of consecutive patients seen by a single specialist at a tertiary, academic referral center, which may limit generalizability to the overall population and to populations outside the United States of America. The cohort size was somewhat limited as we opted to evaluate only cases of uncomplicated ureteroscopy, which are often less common at our referral center. While limiting patients was crucial for limiting heterogeneity within the study cohort, a larger cohort may allow for evaluation of more subtle differences between groups. Nonetheless, given that our rate of compliance is similar to other published rates, the extent of this limitation might be lessened. Additionally, the use of a single surgeon's experience controls for variability in preoperative counseling and postoperative management and instructions. Prospective follow-up of ureteroscopy patients may help determine what types of interventions would be most useful for improving follow-up. Future work should also address healthcare provider factors to address practice limitations and mechanisms for improving patient notification and scheduling coordination, which may also affect patient follow-up. 32
Conclusions
One in every five patients undergoing ureteroscopy fails to return for follow-up. Lost to follow-up rates are broad based and are not predicted by any demographic, stone-related, or operative factors other than having Medicaid or state-sponsored insurance. Lack of follow-up may prevent the diagnosis of postoperative complications and limit ability to counsel patients on stone prevention. Further evaluation and interventions are needed to address patient follow-up in this population.
Footnotes
Author Disclosure Statement
No competing financial interest exists.