
Abstract
Purpose:
We sought to test the content validity of a new training model for flexible ureteroscopy: the Key-Box.
Material and Methods:
Sixteen medical students were randomized to undergo a 10-day training consisting of performing 10 different exercises aimed at learning specific movements with the flexible ureteroscope, and how to catch and release stones with a nitinol basket using the Key-Box (n = 8 students in the training group, n = 8 students in the nontraining control group). Subsequently, an expert endourologist (O.T.) blindly assessed skills acquired by the whole cohort of students through two exercises on ureteroscope manipulation and one exercise on stone capture selected among those used for the training. A performance scale (1–5) assessing different steps of the procedure was used to evaluate each student. Time to complete the exercises was measured. Mann–Whitney Rank Sum test was used for comparisons between the two groups.
Results:
Mean scores obtained by trained students were significantly higher compared with those obtained by nontrained students (all p < 0.001). All trained students were able to complete the two exercises on ureteroscope manipulation within 3 minutes, whereas two students (25%) were not able to finish the exercise on stone capture. Conversely, four (50%) and six (75%) nontrained students were not able to finish one out of the two exercises on ureteroscope manipulation and the exercise on stone capture, respectively. The mean time to complete the three exercises was 76.3, 69.9, and 107 and 172.5, 137.9, and 168 seconds in the trained and nontrained groups, respectively (all p < 0.001).
Conclusions:
The K-Box® seems to be a valid easy-to-use training model for initiating novel endoscopists to flexible ureteroscopy.
Introduction
T
The need for offering a high-level healthcare service, whatever the level of expertise of the surgeon as well as for reducing operating room costs and time, waiting lists, and medico-legal issues due to medical error, 2,3 has led to the development of surgical training models as convenient tools with high educational impact for acquiring technical skills before undertaking endoscopic procedures on patients. 4
A great variety of training simulators has been described for ureteroscopy, ranging from computer-assisted virtual reality to the home-made bench model, each of them with different peculiarities, prices, and proven efficacy. 5
For instance, the past-generation virtual-reality high-fidelity ureteroscopy simulator seems to improve surgical performance and may help shorten the learning curve early in training of novice endoscopists, although high prices may limit the distribution and widespread introduction of such a device into a training curriculum of an academic center. 6,7 Moreover, there is no clear evidence regarding the most cost-effective training strategy. 8,9
In this context, we sought to evaluate the content validity 10 of a new low-fidelity bench model, the Key-Box (K-Box®), by conducting a randomized trial on medical students with no previous experience on flexible ureteroscopy.
Specifically, we assessed technical skills acquisition after a didactic teaching with instructional video and an intensive 10-day specific training with the K-Box or didactic teaching alone to judge the appropriateness of this simulator as an effective training modality.
Materials and Methods
The Key-Box
The Key-Box (K-Box; Porgès-Coloplast, France) is a new-generation portable bench-training training model for flexible ureteroscopy composed of four different independent boxes 11 (Fig. 1). Each box has three entries and three exits on each side, allowing the access of the ureteroscope to three different spaces (Fig. 2A). Each box is provided with flaps, which remain closed, forcing the user to watch what he or she is doing on the screen without direct visual inspection. However, these flaps can be opened if assistance is required, allowing the user to roughly simulate real-life radiological control (Fig. 2B). Each space of the K-Box does not reproduce the exact anatomy of the renal collecting system but creates an environment that forces the user handling the flexible ureteroscope to make the specific movements required when performing a flexible ureteroscopy in humans (Fig. 3).
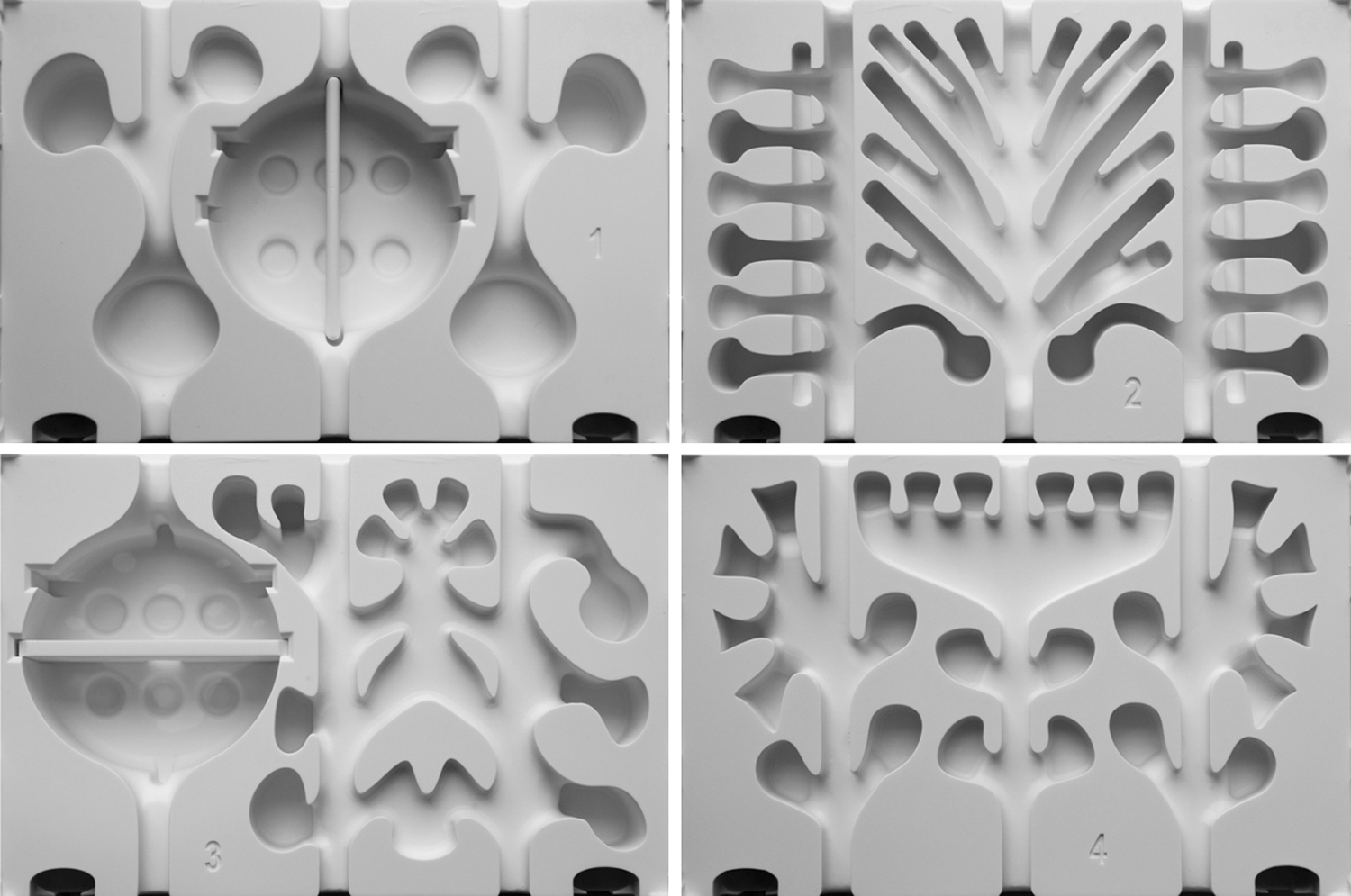
The four different independent boxes composing the K-Box.
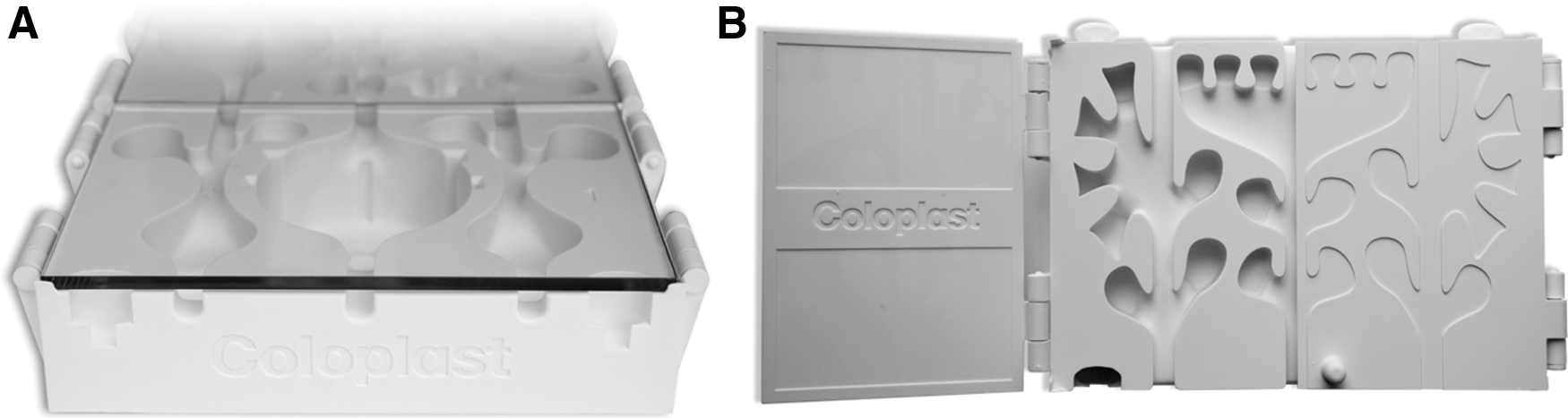
Axial view of the K-Box, showing the three different entries that allow the access to three different spaces
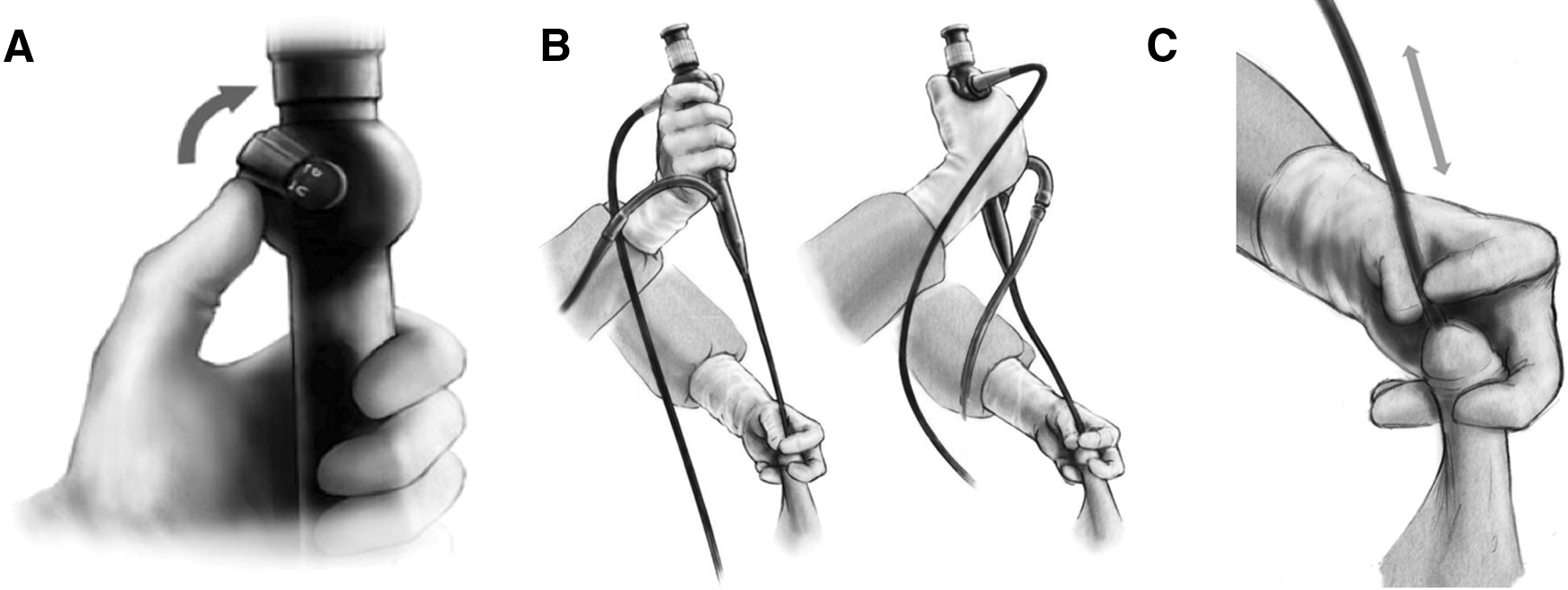
Main movements required to explore the environment with a flexible ureteroscope: upward or downward deflection of the tip of the ureteroscope to explore the vertical axis
Training curriculum
Sixteen medical students (n = 9 women and n = 7 men, aged 22–23 years) were identified on a volunteer basis to receive didactic teaching with a theoretical lesson and a 10-minute video on practical demonstration on the manipulation of a flexible ureteroscope (Flex-XC; Karl Storz) and a nitinol basket (1.9F ZeroTip; Boston Scientific) for stone retrieval by using the K-Box trainer.
At baseline, all students completed the specific questionnaire aimed at assessing the basic knowledge of endourological procedures and endoscopic instruments (Fig. 4).

Baseline questionnaire administered before students' randomization.
Subsequently, they were randomly divided into two groups: The first group (group A, n = 8 students) underwent a 10-day training consisting of personally repeating different exercises aimed at learning specific movements with the flexible ureteroscope (n = 5 days, 10 minutes per exercise per day) and how to catch and release stones with a nitinol basket (n = 5 days, 10 minutes per exercise per day) by using the K-Box trainer. An experienced endourologist followed students during each training session, instructing them on how to acquire specific skills required to perform various exercises. The second group (group B, n = 8 students) served as a nontrained control group and received only didactic teaching.
Students' assessment
After a wash-out period of 2 weeks (at the end of the training), a further video demonstration was offered to all the students to review the manipulation of the flexible ureteroscope and the nitinol baskets inside the K-Box. Finally, an expert endourologist (O.T.) blindly assessed the whole cohort of students through a final examination consisting of performing two exercises on ureteroscope manipulation and one exercise on stone capture using the K-Box selected by the examiner among those used for the training. A performance scale was created by relying on the global rating scale described by Matsumoto and colleagues aimed at assessing the hands-on training with the high-fidelity genitourinary bench model (Uro-Scopic Trainer) 12 and used to evaluate each student in terms of respect for surrounding environment, hand movements, handling of endoscope, finesse in the procedure, knowledge of the procedure, use of assistants, and basket handling (Table 1).
A specific score ranging from 1 to 5 was assigned to every student for each specific domain. Time to complete the exercise was also measured. The success rate was defined as the ability of completing these exercises within 3 minutes. Descriptive statistics were used to detail the results of the two groups. Wilcoxon–Mann–Whitney Rank Sum test was used for comparisons between the two groups, with a significance level set at p < 0.05.
Results
The results of the questionnaire aimed at providing a basic evaluation of the whole cohort showed that six and five students in the trained and nontrained groups, respectively, had already heard about endourology but none of the students had ever assisted an endourological procedure nor had any practical skills in this field.
After specific training, all students (n = 8) were able to complete (within 3 minutes) the two exercises on ureteroscope manipulation, whereas two students (25%) were not able to finish the exercise aimed at capturing the stone with a nitinol basket. Conversely, four (50%) and six (75%) nontrained students were not able to complete (within 3 minutes) one out of the two exercises on ureteroscope manipulation and the exercise on stone capture, respectively.
At final examination, mean scores (±standard error of the mean) were significantly higher in the trained group compared with the nontrained group in terms of respect for surrounding environment, hand movements, handling of endoscope, finesse in the procedure, knowledge of the procedure, use of assistants, and basket handling (Table 2, all p < 0.001). Indeed, trained students learnt properly how to handle the ureteroscope to explore the K-Box cavities with no unnecessary hands movements (Supplementary Video S1; Supplementary Data are available online at
SEM = standard error of the mean.
The mean time (±standard error of the mean) to complete each exercise was 76.3 (±11.6), 69.9 (±9.9), and 107 (±22.5) seconds in the trained group compared with 172.5 (±6.3), 137.9 (±9.4), and 168 (±17.8) seconds in the nontrained group (all p < 0.001).
Discussion
Halstedian concepts of surgical apprenticeship introduced in the early 1950s, based on the principle of “see one, do one, teach one” and adopted for a long time in the past decades for the urologic endoscopic training of surgical residents, has been largely overcome by the development and introduction of simulators and training models that allow young residents and inexperienced surgeons to become confident with surgical instruments and to acquire technical skills before performing endoscopic procedures on live patients in the operating theatre. 13,14
In this context, the K-Box has been developed as a bench model made of four different boxes that can be assembled in different configurations to let the trainees familiarize with flexible ureteroscope handling as long as basic movements and steps are required during endoscopic procedures of the upper urinary tract.
The main aim of the specific 10-day training used in the current study was to enable students to explore the surrounding space in all the three axes. To get this target, didactic teaching and an instructional video offered to the whole cohort of students before their randomization depicted the movement of upward or downward deflection of the tip of the ureteroscope (to see any object that is placed in a vertical axis compared to the position of the ureterscope, Fig. 3A), pronation and supination of the wrist handling the ureteroscope (to see any object that is placed on a horizontal axis compared with the position of the ureteroscope, Fig. 3B), and pushing and pulling the shaft of ureteroscope while keeping straight the tip of the ureteroscope (to see the space forward or backward, Fig. 3C).
The results of the current study showed that students underwent a 10-day specific training and obtained higher scores at final evaluation in all the domains assessing the maneuverability of the ureteroscope compared with nontrained students (all p < 0.001, Table 2). Moreover, grasping and releasing the stone with the nitinol basket was significantly better in the trained group compared with their nontrained counterparts.
The benefit of approaching real-life endoscopic cases with a certain degree of expertise rather than being novice endoscopists has been demonstrated by several authors, demonstrating the role of the learning curve in affecting the success rate, the risk of complication, and endoscope breakage when the instruments were used improperly or by inexperienced users. 15 –17 Moreover, better knowledge of instrument handling and a fluent procedure may not only increase the likelihood of completing the surgery successfully, thus limiting medico-legal concerns, but also can reduce the operative time, with positive implications on waiting lists and cost containment.
In this context, the results of the current study demonstrated that a specific training increases the success rates (100% and 75% of students in the trained group vs 50% and 25% in the control group completed within 3 minutes the two exercises on ureteroscope manipulation and the exercise aimed at using the nitinol basket, respectively) and reduces the time to complete the procedure successfully [76.3 (±11.6), 69.9 (±9.9) and 107 (±22.5) seconds in the trained group compared with 172.5 (±6.3), 137.9 (±9.4), and 168 (±17.8) seconds in the nontrained group, all p < 0.001)] (Supplementary Videos S1 and S2).
Although the K-Box has to be considered as a low-fidelity portable bench training model, since it has not been developed to reproduce accurately the anatomy of the upper urinary tract, but rather to create an environment with different tracks and cavities where the trainees can learn how to manipulate endoscopic instruments and to explore the surrounding space, our findings demonstrate that it achieves the goal for which it was designed, that is, to teach what it is expected to teach.
Generally, it may be argued that surgical training with a high-fidelity or in vivo animal models is the preferred option of the trainees and may be better in terms of face and content validity and have a higher educational value than relying on low-fidelity bench models. 18,19 However, this intuitive belief is not supported by any study comparing the two different training modalities.
Conversely, a randomized trial has demonstrated that hands-on training with a low-fidelity model (consisting of penrose drain, inverted cup, molded latex in portable plastic case, and two embedded straws ∼8 mm in diameter as substitutes for urethra, bladder dome, bladder base, and bilateral ureters, respectively) leads to achieve equal performance as compared with a high-fidelity one (Uro-Scopic Trainer, by Limbs and Things, Bristol, United Kingdom), with no difference in terms of global rating scale, checklist, pass rating, and time needed to complete the task (i.e., to remove a left or right mid ureteral stone), 7 although the cost was definitely in favor of the low-fidelity model (Canadian $20 vs Canadian $3,700 to produce the low- and to purchase the high-fidelity model, respectively). 12
Various high-fidelity models (Uro-Scopic Trainer, Scope Trainer, Adult Ureteroscopy Trainer, UroMentor) have been developed and evaluated in terms of face, content, construct, educational impact, and predictive validity, 8,12,20 –25 thus being at present available to be incorporated into the educational program of academic centers. However, the hypothetical advantage of training on more realistic models or on living animals with the possibility for the trainees to face with respiratory movements, bleeding, and haptic feelings must be balanced either with ethical issues and availability of adequate labs for the in vivo animal models and with the higher costs of purchase and maintenance of certain simulators as compared with the low-fidelity bench models. 14
The K-Box has been designed to let the trainees acquire technical skills while handling endoscopic instruments. Although step-by-step placement of guidewire and access sheath is possible, the K-Box does not guarantee simulation feelings comparable to those offered by the more advanced bench model or virtual-reality trainers. However, this disadvantage has to be weighed against the cost of other more expensive trainers and K-Box seems to be a good alternative to them.
Although our preliminary findings showed the effectiveness of the K-Box for acquiring basic endourological skills, further studies are necessary to evaluate construct, concurrent, and predictive validity of this innovative training model according to specific criteria established in literature 10,26 to demonstrate with an adequate level of evidence its reliability and appropriateness when incorporated into training curricula of novice endoscopists.
Conclusions
Students trained on the K-Box for 10-days achieved higher performance in terms of respect for surrounding environment, hand movements, handling of endoscope, finesse in the procedure, knowledge of the procedure, use of assistants, and basket handling compared with students who received didactic teaching only. The success rate and the time to complete the exercises were in favor of trained students. Further studies are necessary to confirm the reliability and validity of the K-Box as a valid teaching modality for technical skills acquisition of novel endoscopists.
Footnotes
Acknowledgments
The authors want to thank Paola Garavelli and Jeremie Berg for their unconditioned support. Moreover, they acknowledge the Scientific Program of 33rd World Congress of Endourology and SWL held in London, October 2015, where the abstract of the current article first appeared.
Author Disclosure Statement
O.T. is consultant for Olympus, Coloplast, Boston Scientific, Rocamed. Regarding the other authors, no competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.