
Abstract
Introduction:
Hilar clamping is often performed to facilitate robotic partial nephrectomy (RPN). Minimal clamping techniques may reduce renal ischemia, including early unclamping, selective clamping, and off-clamp RPN. We assess the utilization of clamping techniques in a large international consortium of surgeons performing RPN for complex tumors.
Methods:
We retrospectively evaluated 721 patients with complex tumors, who underwent RPN at 11 centers worldwide between 2008 and 2014. Complex tumors were defined as renal masses with a nephrometry score >6. Total clamping was defined as complete clamping of the main renal artery. Minimal clamping techniques included early unclamping, selective clamping, and off-clamp RPN. Clamping techniques were additionally assessed in patients with estimated glomerular filtration rate (eGFR) <60 and in patients with a solitary kidney. Two-tailed t-tests (p < 0.05) were used to statistically analyze differences in mean warm ischemia time (WIT).
Results:
Most patients underwent complete clamping (75.1%). Minimal clamping (24.9%) included early unclamping (10.8%), selective clamping (8.7%), and off-clamp (5.4%). Mean WIT of total clamping, selective clamping, and early unclamping was 22.2, 21.2, and 17.3 minutes, respectively. Of patients with an eGFR <60 (n = 90), 26.6% underwent minimal clamping, including 15.5% early unclamping, 4.4% selective clamping, and 6.7% off-clamp. Of patients with solitary kidneys (n = 12), 10 (83%) were performed with total clamping with mean WIT of 14.9 minutes.
Conclusions:
In this large international series of RPN for complex tumors, most patients underwent total clamping of the main renal artery. Minimal clamping techniques, including early unclamping, selective clamping, and off-clamp techniques, were used in a minority of cases. There was no significant increase in use of minimal clamping, even in patients with chronic kidney disease or solitary kidneys. However, mean WIT was low (<23 minutes) in all patient groups.
Introduction
C
Modifications to renal hilar clamping technique in RPN have been suggested to minimize ischemic injury to functional renal cells. These include the following: early unclamping, 4 selective clamping, 5 and off-clamp techniques. 6,7 Complete hilar clamping involves clamping of the main renal artery and vein to minimize blood loss and optimize visualization, but results in increased ischemia time. In early unclamping, the renal hilum is clamped only for tumor excision and initial central running suture. 4 Selective clamping utilizes renal segmental arteries such that tumor-specific ischemia is pursued. 5 The off-clamp technique avoids clamping of renal and instead pursues anatomic arterial microdissection in an attempt to preserve renal function. 6,7 Although these minimal clamping techniques are well described in this literature, it is currently unknown if surgeons are actively utilizing modified techniques.
Methods
This study identified 1596 patients from the Vattikuti Collective Quality Initiative database who underwent RPN at multiple medical institutions worldwide between 2008 and 2014. A schematic diagram detailing the inclusion and exclusion criteria (Fig. 1) illustrates our design process. We defined complex tumors as renal masses with a PADUA or R.E.N.A.L nephrometry score >6. Clamping technique, mean WIT, preoperative glomerular filtration rate (GFR), and solitary kidney status were recorded for all patients. Patients who did not have clamping technique, PADUA/R.E.N.A.L score, mean WIT, GFR, or solitary kidney status recorded were excluded. Patients who underwent RPN with tourniquet (n = 1) or Satinsky clamp (n = 1) were also excluded. Bulldog clamps were used to achieve ischemia in all cases included. Total clamping was defined as complete clamping of the main renal artery. Minimal clamping techniques included early unclamping (removal of main renal artery clamp immediately following the inner layer renorrhaphy), selective clamping (clamping of selective arteries supplying the tumor), and off-clamp RPN (no clamping). The choice of clamping techniques was made at the discretion of the surgeon. After exclusion criteria, 721 patients with complex tumors were available for the analysis. Estimated glomerular filtration rate (eGFR) was calculated preoperatively and at time to last follow-up using the Modification of Diet in Renal Disease equation and the change in eGFR was compared between groups. Two-tailed t-tests and chi-squared tests (p < 0.05) performed using Microsoft Excel 2013 were used to statistically analyze the results.
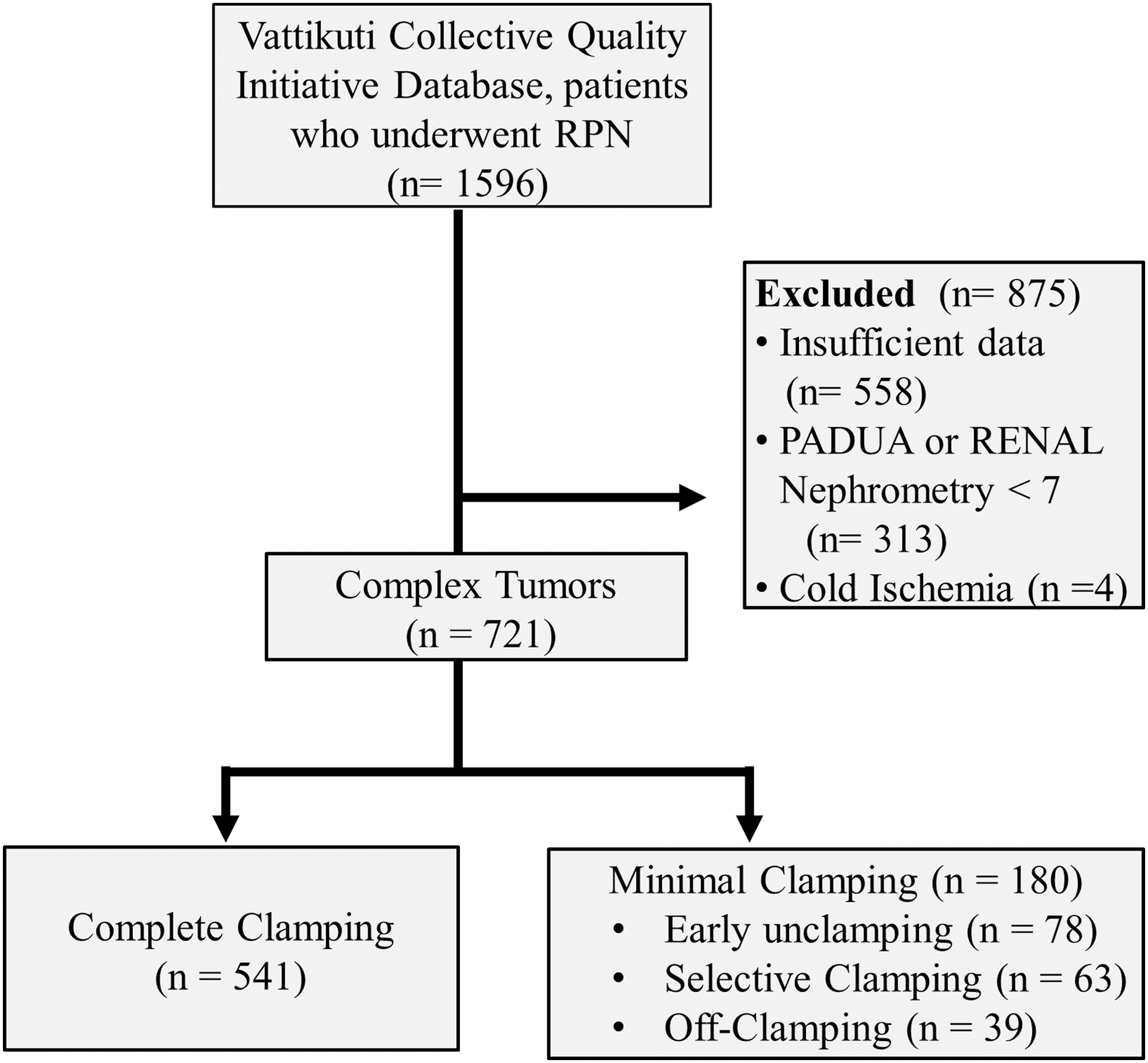
Schematic of design process of patients included and clamping techniques.
Results
The majority (75.1%) of patients with complex renal tumors had RPN performed with complete clamping of the renal artery (Table 1). Only 24.9% of complex cases were performed with minimal clamping techniques, which included early unclamping (10.8%), selective clamping (8.7%), and off-clamp (5.4%) (Fig. 2). Mean WIT of complete clamping, early unclamping, and selective clamping was 22.2, 17.3, and 21.2 minutes, respectively. In addition, patients were grouped by preoperative renal function: those with preoperative eGFR <60 mL/min/1.73 m2 and those with preoperative eGFR >60 mL/min/1.73 m2. The majority (73.3%) of patients with preoperative eGFR <60 underwent RPN with complete clamping (Fig. 3). Of patients with an eGFR <60 (n = 90), only 24.7% underwent RPN with minimal clamping, including early unclamping (15.5%), selective clamping (4.4%), and off-clamp techniques (6.7%). No statistically significant difference was found between any clamping technique and preoperative eGFR (p = 0.20). Patients were also grouped based on solitary kidney status. Of patients with solitary kidneys (n = 12), 10 (83%) were performed with complete hilar clamping with mean WIT of 14.9 minutes.
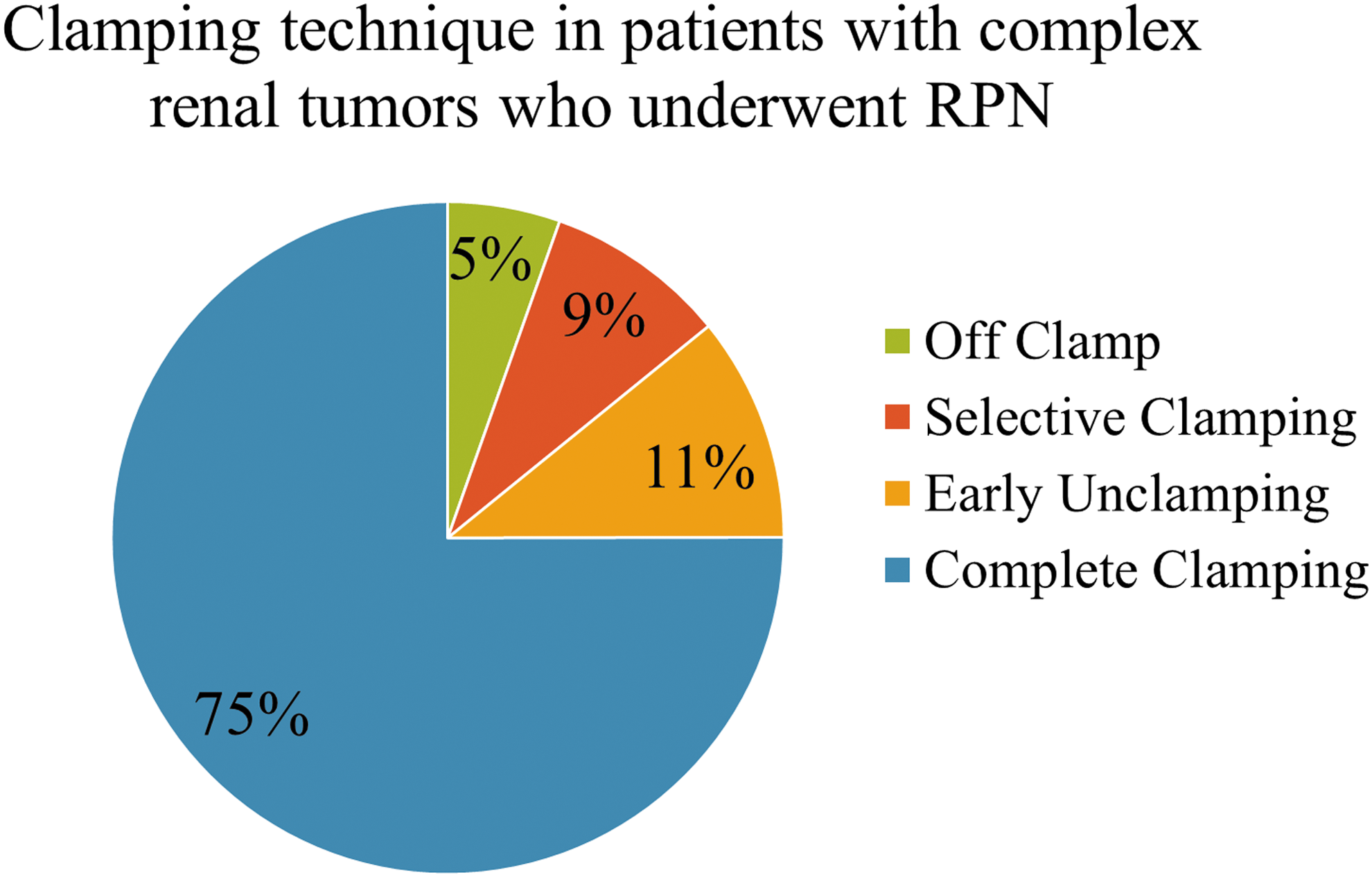
Distribution of clamping technique in patients with complex renal tumors who underwent RPN (n = 721). Majority of cases were performed with complete clamping of the main renal artery (n = 541). Only 24.9% of complex cases were performed with minimal clamping techniques. RPN, robotic partial nephrectomy.

Distribution of clamping technique frequency by preoperative GFR (mL/min/1.73/m2). No statistically significant difference was found between any clamping technique and GFR (p = 0.20). GFR, glomerular filtration rate.
GFR = glomerular filtration rate.
A total of 393 of the 721 (55%) patients had both preoperative and postoperative eGFR data available (total clamping n = 301; early unclamping n = 35; selective clamping n = 32; off-clamp n = 25). No statistically significant difference in change in eGFR (mean follow-up 16.3 months) was found between total clamping (p = 0.33), early unclamping (p = 0.98), selective clamping (p = 0.88), and off-clamp techniques (p = 0.06).
Discussion
Partial nephrectomy is a nephron-sparing technique that provides equivalent oncologic outcomes when compared to a radical nephrectomy. 8 Partial nephrectomy is facilitated by clamping of the renal hilar vessels to minimize blood loss and improve visualization of the operating field. RPN is a minimally invasive technique that can facilitate partial nephrectomy, particularly in complex tumors. 9 However, the temporary ischemia by vessel clamping may cause damage to functional nephrons. There is controversy on the factors contributing to postoperative renal function, but many studies suggest the length of WIT, increased blood loss, and preoperative renal function as major determinants of postoperative renal function. 1,2 This has led to efforts to minimize WIT during partial nephrectomy. 3 Modifications to clamping techniques have been suggested to minimize ischemic injury, including early unclamping, 4 selective clamping, 5 and off-clamp techniques. 6,7 Recommendations to reduce ischemia have been focused on patients with comorbidities or preexisting decreased renal function. 10 As described by Nguyen and Gill, early unclamping can be performed such that the main renal hilar clamp is removed after the initial central running suture, 4 allowing revacularization of the renal parenchyma during the remainder of the renorrhaphy. In their study, WIT was reduced by more than 50%. In addition, McClintock and colleagues described a technique where near-infrared fluorescence imaging can be used to facilitate clamping of selective segmental arteries. 5 Segmental arteries allow for selective ischemia of specific kidney segments, thus reducing global renal ischemia. 10 Gill and colleagues described an off-clamp “zero ischemia” technique for RPN, taking advantage of high-order segmental renal arteries that supply the renal mass. In their approach, ischemia time was zero, all patients had negative tumor margins, and pre/postoperative eGFR were comparable. 6,7 However, for patients with normal renal function and a mean WIT <25 minutes, no long-term benefit in preservation of renal function was found in off-clamp vs hilar clamping techniques. 11
Although these clamping techniques are well described in the literature, it is unknown to what extent surgeons are utilizing them in current clinical practice, especially in patients who might most benefit, such as those with decreased preoperative GFR and solitary kidney status. In our retrospective study of international consortium of surgeons, we found that most surgeons performed RPN using complete clamping of the main renal artery vs minimal clamping techniques such as early unclamping, selective clamping, and off-clamp techniques. However, regardless of clamping technique performed, mean WIT was low, and <25 minutes. Thus, damage to remaining functional renal parenchyma is presumed to be minimal. This could partially explain why there was no statistically significant difference in postoperative renal function seen between different clamping techniques.
In addition, utilization of minimal clamping techniques did not change despite a patient's preexisting renal morbidity, with the frequency of each clamping technique comparable between eGFR >60 and eGFR <60 cohorts. Furthermore, patients with preoperative solitary kidney status had RPN performed by complete hilar clamping in majority of cases, with low ischemia times.
Minimal clamping techniques may involve more surgical complexity; although all surgeons in our study were skilled, different degrees of experience may perhaps be a confounding factor in our results. In addition, our study did not assess clamping of the renal vein as these data were not available. Our findings are also limited by the lack of available eGFR data in 45% of patients, potential selection bias, and the retrospective nature of the study.
Conclusions
In this large international series of RPN for complex tumors, minimal clamping techniques, including early unclamping, selective clamping, and off-clamp techniques, were used in a minority of cases. There was no significant increase in the use of minimal clamping techniques over complete hilar clamping, even in patients with chronic kidney disease or solitary kidneys. However, mean WIT was low (<23 minutes) in all patient groups.
Footnotes
Author Disclosure Statement
No competing financial interests exist.