
Abstract
The prevalence of urinary stones in the United States has been described as 1 in 11 persons reporting a history of stones. Imaging plays a crucial role in diagnosis, management, and follow-up for these patients and imaging technology over the last 100 years has advanced as the disease prevalence has increased. CT remains the gold standard for imaging urolithiasis and changes in this technology, with the addition of multidetector CT and dual-energy CT, as well as the changes in utilization of CT, have decreased the radiation dose encountered by patients and allowed for improved stone detection. The use of digital tomography has been introduced for follow-up of recurrent stone formers offering the potential to lower radiation exposure over the course of a patient's lifelong treatment. However, there is still a demand for improved imaging techniques to detect smaller stones and stones in larger patients at lower radiation doses as well as the continued need for the judicious use of all imaging modalities for healthcare cost containment and patient safety.
Introduction
U
Intravenous Urogram
The historical evolution of imaging for urolithiasis began in 1923 with the description of the excretory urogram showing the excretion of sodium iodine. 2 Until the 1990s, the intravenous urogram (IVU) was the imaging modality of choice for the evaluation of patients with suspected urolithiasis, specifically ureteral calculi given its ability to delineate pelvicaliceal and ureteral anatomy, as well as upper urinary obstruction. Studies reported sensitivities and specificities of 70% and 95%, respectively. 3,4 Its limitations, however, are that it requires the administration of intravenous (IV) contrast, additional IVU radiographs are needed in the setting of obstructing stones, which extend the time of the study, an inability to visualize nonradiopaque calculi, as well as an inability to assess for other causes of the patient's pain that can mimic renal colic.
Computed Tomography
In 1995, Smith and colleagues found that a noncontrast-enhanced CT scan was more sensitive for the depiction of ureteral stones in patients with acute flank pain caused by ureteral obstruction, and since that time, the use of unenhanced helical CT scans has been the gold standard diagnostic imaging modality to identify urolithiasis. 5 CT has high sensitivity and specificity for detection of urinary tract stones of 95% to 100% and 96% to 98%, respectively. 5 –8
CT is the preferred imaging technique for patients who present to the emergency room (ER) with renal colic given its availability, rapid test performance, and absence of the need for oral or IV contrast administration, as well as its ability to assess the rest of the abdomen and pelvis for alternative causes of the patient's pain, such as appendicitis, diverticulitis, cholecystitis, or gynecological pathologies such as a hemorrhagic cyst or torsed ovary. 6 In the specific case of upper tract urolithiasis, CT has the advantage of assessing for secondary signs of renal and ureteral obstruction such as hydroureteronephrosis, periureteral edema, and unilateral renal enlargement.
In 1998, multidetector CT (MDCT) was introduced. MDCT is a form of CT technology, which uses a multidimensional array of detector elements replacing the linear array of detector elements used in typical conventional and helical CT scanners. The advantages of MDCT include faster scan times and the ability to acquire images at thinner slice intervals along with the ability to perform multiplanar reformations and three-dimensional reconstructions. 9 –11 The technology has developed rapidly with 4-, 8-, 16-, 32-, 40-, 64-, 256-, and 320-detector systems. 12,13 In the detection of urolithiasis, MDCT allows not only for the evaluation of the number of stones, size, location, and presence or absence of hydronephrosis but also for the volumetric analysis of stone burden and analysis of stone composition. 9,14
An MDCT protocol for the evaluation of stone disease covers the field of view from at least the upper pole of the kidneys to the base of the urinary bladder. A reconstruction slice thickness of 1 to 3 mm is ideal for detection and characterization of urinary calculi. Optimized MDCT protocols should allow for excellent detectability of stones while minimizing radiation dose to as low as reasonably achievable. MDCT scanners with more than four rows allow for two different collimations (millimeter and submillimeter), therefore it is recommended in clinical practice to choose a reconstruction thickness of no more than 5 mm with the reformatted coronal/sagittal images at 3 mm, improving stone detection and lowering radiation dose. 9,12,14 The utility of coronal reformatted images for stone detection and evaluation include differentiation of calcified vascular and renal parenchymal plaques, detection of urinary calculi that could go unrecognized on axial imaging, and better volumetric stone sizing estimates. 14 –16 Additionally, the use of MDCT can aid in surgical planning during percutaneous nephrolithotomy (PNL) procedures or extracorporeal shockwave lithotripsy (SWL) by evaluating the kidney position, orientation of the posterior calices, HU or CT density of the stones, and skin-to-stone distance, as well as the relationship of the kidney to other visceral organs. 9
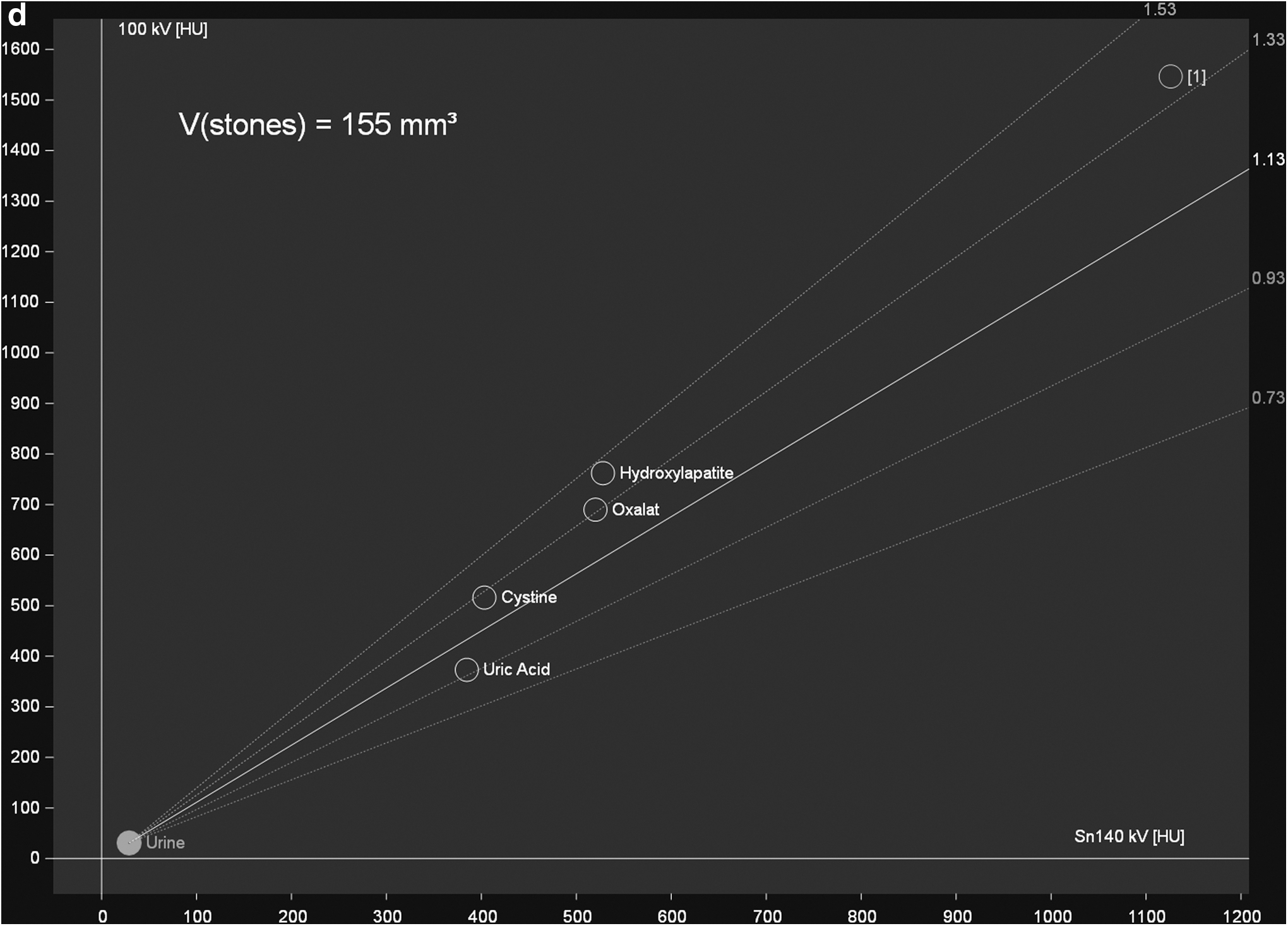
The utility of CT in diagnosis and treatment strategies lies in the characterization of stone size, location, composition, and potentially even stone fragility by examining whether there are areas of low attenuation within the body of the stone to suggest heterogeneity. Single-energy CT uses HU to help specify stone composition; however, there is wide variability in the density of stones of the same mineral component and stones of mixed composition. 17,18 One of the technologies introduced in the last decade includes dual-energy CT (DECT). There is compelling evidence that DECT can reliably determine the chemical composition of kidney stones both in vitro and in vivo. 19 –21 By using dedicated postprocessing techniques, the dual-energy ratio of a stone—defined as the mean attenuation value of the stone on the low-energy image divided by attenuation on the high-energy image—is calculated for each stone type. This approach allows for a general distinction of uric acid (made up of elements with low atomic numbers, such as hydrogen, carbon, nitrogen, and oxygen) from nonuric acid stones (which are made up of elements with higher atomic numbers, such as phosphorus, calcium, and sulfur). Modern DECT platform and reconstruction algorithms also enable more detailed stone composition analysis, including differentiation of cystine, struvite, calcium oxalate dihydrate or monohydrate, and apatite stones (Fig. 1).

Forty-six-year-old female presenting with acute left flank pain.
Another important clinical application of DECT is the reconstruction of virtual noncontrast (VNC) images, which may be used to remove the iodinated contrast material from the collecting system on images acquired during the excretory phase, allowing detection of both renal and ureteral stones. Preliminary evidence suggests that the VNC images can detect clinically relevant urinary stones (i.e., larger than 5 mm) with diagnostic accuracy equal to a true noncontrast image 22 (Fig. 1). This technique may substantially decrease the patient's overall radiation exposure by obviating the need of a separate noncontrast acquisition. 22 Another advantage of VNC images is the ability to assess precontrast attenuation of renal masses when dedicated unenhanced CT imaging has not been performed.
DECT can also be used postoperatively to distinguish between residual stone and tube placement in the cases of a stent or nephrostomy tube. The use of the color overlays allows better separation between stone and stent/tube. For example, the stone material could be colored blue, while the stent would be colored red. 23
Radiation dose considerations in CT
In addition to advances in the imaging technologies described above, there have been advances in the application of these technologies to reduce radiation exposure. Since the early 1980s, there has been a significant increase in the amount of medical radiation exposure and much of this can be attributed to the increased utilization of CT scans. Patients with urinary stone disease are at particularly high risk of continued radiation exposure from imaging during a single stone episode, but for recurrent stone formers, their risk is elevated over the course of their lifetime of treatment. 24,25 A study evaluating radiation dose associated with CT scans performed in 2008 at four different hospitals found that a noncontrast CT (NCCT) of the abdomen pelvis ranges from 3 to 43 mSv, with a median dose of 15 mSv. This study also estimated the lifetime attributable risk associated with the median radiation dose observed and found that younger female patients are at the highest risk and potentially higher than previously reported. 26
To address the issue of radiation exposure associated with NCCT, there have been several studies assessing the effectiveness of low-dose NCCT protocols for the evaluation of urolithiasis. Low-dose protocol NCCT of the abdomen and pelvis is generally considered to have an effective radiation dose <3 mSv. Several studies have found similar sensitivities (96%–97%) and specificities (95%–97%) for standard and low-dose NCCT scans for the detection of urolithiasis. 27 –30 However, what has been noted is that the sensitivity and specificity decline in patients with body mass indices (BMIs) >30 kg/m2 and for stones <3 mm. 27,31,32 Both the American Urological Association (AUA) and the European Association of Urology (EAU) recommend a low-dose protocol NCCT scan during the initial presentation of renal colic, excluding pediatric and pregnant patients, and both assert that in patients with BMI greater than 30 kg/m2, a standard-dose NCCT scan should be performed to maximize stone detectability and limit the number of false-negative examinations. 25,33
Additionally, there have been investigations into ultralow-dose NCCT protocols that further reduce radiation exposure. The effective dose of ultralow-dose CT (ULDCT) has been less well defined, but the literature reports typical effective doses between 0.5 and 0.9 mSv, essentially equivalent to a plain abdominal radiograph. 34,35 One study found that the sensitivity and specificity of these ultralow-dose NCCTs for detection of urinary calculi are on par with LDCT at 97% and 95%, respectively. 34 However, another study using MDCT from three different vendors, all >64 row scanners, performed at submilli-Sievert level was not sufficient for diagnostic confidence for renal stones. 36
One of the disadvantages of low-dose CT (LDCT) imaging for stone detection has been a reduction in the image quality due to an increased level of image noise at these low doses. Noise can make it hard to distinguish between small structures without contrasting surrounding tissue, such as fat, specifically between the distal ureter and surrounding or adjacent structures. Until the last decade, filtered back projection (FBP) algorithms have been the standard for image reconstruction based on speed and ease of implementation; however, the desire to have better resolution, lower radiation dose, and faster scan times has led to the more widespread availability of iterative reconstruction algorithms. In addition, advances in computing speeds have made iterative reconstruction algorithms more feasible in clinical use. 37,38 These iterative reconstruction algorithms help to reduce the noise associated with FBP algorithms, allowing for improvements in the image quality of a low-dose protocol CT and therefore improved diagnostic performance at a lower radiation dose to the patient. 37 –39
Current AUA guidelines assert that CT is the first-line imaging modality to establish a diagnosis of nephrolithiasis and the EAU suggests that CT scan should be performed following initial ultrasound (US) assessment to confirm the diagnosis. 25,33 Both governing bodies emphasize that a low-dose, or reduced-dose, protocol should be employed in patients with BMI <30 kg/m2. However, even despite these recommendations for reduced-dose CT imaging, a report by the American College of Radiology found that only 2% of the nearly 50,000 CT scans performed for renal colic at 93 institutions were conducted at a reduced dose or effective dose of 3 mSv. 40 More work is needed to create standardized LDCT and ULDCT protocols that can be used at a greater number of sites nationally.
Fluoroscopy
As one of the few modalities that provide live imaging of the patient, intraoperative fluoroscopy is the principal imaging modality for guiding urologic procedures, including ureteroscopy (URS), SWL, and PNL. The effective radiation dose that patients receive during fluoroscopy for URS and PNL has been measured between 1.0 and 8.6 mSv, respectively. 41 –44 One study looked at fluoroscopy times during URS and found that after implementing simple strategies, such as having preoperative imaging available during the case, having a laser-guided C-arm, and using a designated fluoroscopy technologist, as well as the use of visual and tactile cues rather than relying on a fluoroscopic image, reduced fluoroscopy time by 82%. 45 In addition, there are data that show that decreasing the pulse rate of the fluoroscopy unit from the standard 30 frames per second to 4 frames per second during URS and PNL reduces fluoroscopy times. 41 Unpublished data on a novel image enhancement device to reduce fluoroscopic radiation exposure during URS showed a reduction in patient exposure by 63% and a fourfold reduction in the amount of radiation the surgeon was exposed to. 46
Digital Tomosynthesis
CT is certainly the most sensitive and specific imaging modality to evaluate the presence of urinary calculi; however, other imaging modalities are still routinely employed during the management of a single stone episode as well as the continued management of a recurrent stone former. Plain abdominal radiographs, commonly called KUBs (refer to kidney, ureter, and bladder radiographs), are still used in clinical practice. The AUA clinical effectiveness protocol draws on data that suggest the use of KUB as an adjunct to CT in cases where the stone is not visible on the CT scout image given that if the stone is not seen on a scout image, it may be seen on a KUB roughly 30% of the time. 25,47 In addition, KUB is widely used to follow a patient with a radiopaque stone during a trial of passage and to monitor stone burden in recurrent stone formers.
Digital tomosynthesis (DT), a derivative of the standard KUB and a novel technique, is a series of low-dose projection images taken during a single sweep of the X-ray tube over a limited range (<60° arc). Digital software then reconstructs the images to provide high-resolution coronal slices at different depths. The advantages of this technology lie in its ability to minimize the effects of obscuring structures such as bowel gas on stone detection in addition to allowing differentiation of ureteral calculi from spinal processes. 48,49 The effective dose of DT has been measured in a phantom model to be 0.87 mSv, in the range of a standard KUB. 50 This is in contrast to a series of KUBs and tomograms where a single scout KUB image is obtained with three tomographic sweeps amounting to a reported effective dose to be almost 4 mSv, greater than a low-dose protocol NCCT. 51
Using unenhanced MDCT of the abdomen and pelvis as a control, DT was found to be superior to KUB in the detection of renal stones with improved detection of stones between 2 and 5 mm. 52 Additionally, an IVU with DT was found to have an improved diagnostic quality over a traditional IVU increasing from 46% to 95% with a significant reduction in radiation dose. 49 This has significant implications for imaging follow-up in recurrent stone formers given that DT was found to be as effective as NCCT in following recurrent stone formers as well as evaluation of postoperative stone-free status. 53
Cost Containment
While technological advances for imaging in urolithiasis have allowed for excellent detection of stones at lower radiation doses, there are recommendations to use imaging technologies judiciously both for reduced radiation exposure and cost containment.
US is still a valuable imaging modality and used commonly in the diagnosis and follow-up of patient's with known or suspected ureteral stones. US allows for detection of secondary signs of stone disease such as obstruction if the calculi are not well visualized. The EAU guidelines on urolithiasis recommend US as the initial diagnostic test for patients with renal colic, followed by NCCT, given that with US there is no exposure to radiation, it is readily available, and there are data to show that US has a pooled sensitivity and specificity for detection of ureteral calculi at 45% and 94%, respectively. 54
Smith-Bindman and colleagues suggested in a study published in the New England Journal of Medicine in 2014 that US should be used as the initial diagnostic test for patients presenting to the emergency room with suspected nephrolithiasis. They did not find a significant difference between the US group and the CT groups for 30-day incidence of high-risk diagnoses with complications, serious adverse events, pain scores, and return emergency room visits or hospitalizations, and there was significantly lower radiation dose in the US group even after factoring in the patients that ultimately underwent a secondary CT scan. 55
Interestingly, however, a study looking at healthcare costs for patient's presenting to the ER who underwent point-of-care US, radiology US, or CT scan concluded based on cost analysis that there was no difference in the overall healthcare cost between the groups, suggesting that the imaging choice did not contribute to a substantial portion of the total healthcare cost. Conversely, when the group did sensitivity analyses to determine if the frequency of subsequent CT scans performed in the US assigned groups was the reason that there was no statistical difference in the total cost analysis, they found a statistically significant reduction in the ED visit cost for the US group compared with the CT group. 56
US is a valuable tool in the follow-up of patients who have passed a ureteral calculus and or undergone surgical intervention with or without extraction of the offending stone. The AUA clinical effectiveness protocol asserts that all patients undergoing surgical intervention for ureteral calculi must undergo follow-up US. Evidence based on a model suggests that the lifetime cost of silent obstruction is $10,200 and that the cost saved by selectively imaging patients following URS was only $130 dollars per patient compared with routine postoperative imaging. 25,57,58
US also remains the first-line diagnostic imaging modality for pediatric and pregnant patients. Even with low-dose and ultralow-dose protocol NCCT scans, there is still ionizing radiation the fetus is exposed to. Therefore, despite the advances in CT described above, the use of US still has valuable diagnostic advantage on certain populations. The use of magnetic resonance imaging (MRI) in pregnant patients can help delineate secondary signs of nonphysiologic renal and ureteral obstruction caused by ureteral calculi even though MRI has significant limitations in its ability to directly visualize the calculi; one study shows that discrete calculi were only visualized 50% of the time with MRI compared with CT. 59 There are other limitations to the use of MRI in diagnosis of urolithiasis, particularly its availability and cost.
Conclusion
Imaging plays an important role in the diagnosis and management of urolithiasis and has evolved over the last 100 years since the initial uses of the KUB. It is prudent among medical professionals, particularly the urologist, to understand the imaging modalities available to them for efficient, effective, and safe treatment of their patients. NCCT remains the gold standard imaging modality and initiatives to increase the utilization of low dose and low-dose protocols will continue to allow for safe and responsible imaging of patients with renal stones. There remains a continued need for technological advances to improve detection of smaller stones as well as stones in larger patients at lower radiation doses. Furthermore, with rising costs of healthcare and the move toward value-based incentives for physicians, prudent use of imaging and technology for the best patient and overall societal outcome as a whole are necessary considerations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.