
Abstract
Introduction:
Although still experimental, focal treatment is being increasingly implemented in the management of prostate cancer (PCa). Aim of the current study was to compare functional and oncologic outcomes of high-intensity focal ultrasound (HIFU) hemiablation of the prostate to robot-assisted laparoscopic prostatectomy (RALP) in the management of unilateral PCa.
Materials:
Fifty-five men with unilateral, clinically localized PCa underwent HIFU hemiablation of the affected prostatic lobe between 2007 and 2015. All patients were found to have unilateral disease on the basis on full concordance between multiparametric magnetic resonance imaging (MRI) and MRI-guided biopsies. These patients were matched 1:1 with patients who underwent RALP for PCa in which pT2a-b disease (unilateral) was found on final pathologic analysis. Matching criteria were Gleason score, prostate specific antigen (PSA), and cT stage. Treatment failure was defined as the need for salvage external beam radiotherapy or systemic androgen deprivation therapy (ADT) due to disease progression. Kaplan–Meier curves and log-rank tests were constructed to assess differences in salvage treatment free survival across surgical techniques.
Results:
Matching was effective with no significant differences across the two groups, although men treated with HIFU were older (p < 0.001). Median follow-up was 36 months (interquartile range 16–56). HIFU was associated to better and faster recovery of continence, with most men (82%) showing no signs of urinary incontinence even right after surgery. Moreover, the risk of de novo erectile dysfunction was significantly lower after HIFU. No significant difference was found in the need for salvage external beam radiation therapy or ADT across the two surgical approaches: 7/55 men underwent salvage therapy in the HIFU vs 6/55 in the RALP group (p = 0.76). Nonetheless, seven more patients in the HIFU arm required a complementary treatment on the contralateral lobe during follow-up, after developing a contralateral PCa. No patient died of PCa on follow-up, while six men died of other causes (five HIFU vs one RALP, p = 0.11).
Conclusion:
In this matched pair analysis, HIFU hemiablation was comparable to RALP in controlling localized unilateral PCa, with no significant differences in the need for salvage therapies. HIFU was also associated to significantly better functional outcomes. Accurate patient selection remains vital, and larger prospective trials are needed to confirm our findings.
Introduction
P
In our department we began performing HIFU hemiablation of the prostate 9 years ago, 9 in patients with unilateral disease, proven by full correspondence between multiparametric MRI and MRI-guided targeted biopsies. 10 In the same period we were also performing RALP for patients with low and intermediate risk PCa, of which some also harbored unilateral disease as demonstrated by final pathologic analysis. Aim of the current study was to compare functional and oncologic outcomes of HIFU hemiablation of the prostate to RALP in the management of unilateral PCa.
Patients and Methods
After institutional review board approval, we retrospectively analyzed patients undergoing HIFU prostatic hemiablation for unilateral disease and patients who underwent RALP for pT2a-pT2b (unilateral) PCa between 2007 and 2015.
For HIFU hemiablation, patients were selected if the positive biopsy pattern was in complete concordance with the PCa lesions identified by MRI with precise loci matching on multiparametric approach. We included men with localized PCa (≤cT2), a prostate specific antigen (PSA) <15 ng/mL, a life expectancy of at least 5 years, and a prostate volume <40 cm3. We excluded patients who had extraprostatic extension on multiparametric MRI, suspected regional lymph nodes or distant metastases on cross-sectional imaging or bone scan, and/or previous HIFU or radiation therapy to the prostate. All patients underwent hemiablation using HIFU delivered by the Ablatherm integrated imaging system (EDAP-TMS, Vaulx-en-Velin, France), performed by a single surgeon (R.v.V.) with a high level of experience in whole-gland HIFU. HIFU hemiablation was defined as ablation of one lobe of the prostate and not just the index lesion because of device technical limitations. HIFU energy was delivered only to the hemi prostate gland, with no treatment of the ipsilateral neurovascular bundle within the technical feasibility of the approach.
Matching
Patients treated by HIFU prostatic hemiablation were matched 1:1 by propensity score analysis with patients undergoing RALP in the same years, in which unilateral PCa was detected on final pathologic report (pT2a-2b, unilateral disease). RALP was performed by three expert surgeons (R.v.V., A.P., and E.H.), all using the same surgical technique. A bilateral nerve sparing approach was performed in all cases. Urinary catheter was usually retrieved at day 5 postoperatively, after a retrograde cystography showed no leakage. The matching procedure was blinded to the outcome, guaranteeing the sorting of patients according to the matching parameters without bias in their outcomes. Matching criteria were, in order: Gleason score, preoperative PSA, and cT stage (cT1c vs cT2). To confirm an appropriate matching, the absence of significant clinical and pathologic differences between the two cohorts of patients treated was assessed using Wilcoxon Rank-sum or χ 2-test, as appropriate.
Functional follow-up
Urinary functional outcomes and erectile function were reported using patient-reported rates. Continence was considered in a categorical manner as 0 vs ≥1 pad. Patients were considered potent if erections, with or without iPDE5, were sufficient for intercourse.
Oncologic follow-up
Given the inherent difference across the two surgical approaches (organ-sparing vs radical extirpation), comparison of biochemical recurrence rates using PSA is inadequate. Moreover, there is currently no accepted definition for disease control following HIFU. 11,12 We therefore decided to test difference in treatment failures, identified as the need for local salvage therapy (radiotherapy of surgery), hormonal therapy, or metastases.
High-intensity focal ultrasound
Given the presence of an untreated half-prostate, an individual PSA nadir was identified in each patient. Biochemical recurrence according to Phoenix criteria (Nadir +2 ng/mL) 13 was used as a threshold to offer a new set of bilateral biopsies. Treatment failure was defined as positive biopsy of the treated area independent of the percentage of core involvement or if salvage radiation or hormonal therapy was needed during follow-up. Contralateral positive biopsy was not considered as a clinical failure, but as a metachronous development of a contralateral disease and was treated by a secondary contralateral hemiablation according to our protocol.
Robot-assisted laparoscopic prostatectomy
Biochemical recurrence was defined by a PSA level >0.2 ng/mL and subsequent rise. 14 The date of the first PSA ≥0.2 ng/mL was used to define biochemical recurrence. Salvage radiotherapy or hormone therapy was offered according to PSA doubling time, pathologic Gleason score, and final pathologic report.
Kaplan–Meier curves and log-rank tests were performed to analyze the influence of the surgical approach on salvage treatment free survival. Statistical significance was considered for p ≤ 0.05. Analyses were performed using STATA version 11.1 (StataCorp, TX).
Results
Fifty-five patients treated by HIFU hemiablation were identified and included in the study. These were matched 1:1 to 55 men who had undergone RALP with pT2a-2b stage in the same period. Matching was effective with no significant differences across the two groups (Table 1), although men treated with HIFU were older (p < 0.001).
Mann–Whitney test.
χ 2-test.
HIFU = high-intensity focal ultrasound; IQR = interquartile range; PSA = prostate specific antigen; RALP = robot-assisted laparoscopic prostatectomy.
Concerning early postoperative complications, these were detected in 8/55 (15%) in the HIFU group and 11/55 (20%) in the RALP group (p = 0.71). These events were mainly Clavien I complications, as prolonged acute urinary retention after HIFU and anastomotic leakage required extra catheter days in the RALP group. All Clavien II complications were urinary tract infections. One patient developed malignant hypertension requiring intensive care in the RALP group. Length of stay was 4 days (interquartile range [IQR] 3–5) in the HIFU group and 7 (IQR 7–8) in the RALP group (p < 0.001). Of note, our patients are allowed to leave the ward only after all catheters and drains are withdrawn.
Median follow-up was 36 months (IQR 16–56). Concerning functional outcomes (Table 2), HIFU was associated to better and faster recovery of continence, with most men (82%) showing no signs of urinary incontinence (0 pads) even just after surgery. This rate was significantly more elevated compared to patients undergoing RALP, in which 40% had 0 pads at 1 month control (p < 0.001). Moreover, the risk of de novo erectile dysfunction was significantly lower after focal HIFU. Indeed, a higher rate of patients in the RALP group presented de novo, persistent erectile dysfunction after surgery (44% vs 20%, p = 0.03). It must be highlighted that patients in the HIFU arm were also older, thus at increased risk of postoperative erectile dysfunction. 15
Wilcoxon Rank-sum.
χ 2.
Bold type indicates statistically significant values.
Specific biochemical outcomes of HIFU hemiablation have been previously published. 9 When analyzing oncologic outcomes, we did not observe a significant difference in terms of salvage therapy free survival across the two groups (Fig. 1). In fact, 7/55 patients in the HIFU arm vs 6/55 patients in the RALP arm required salvage external beam radiation therapy, androgen deprivation therapy, or both during follow-up (p = 0.76), with a nonsignificant difference in time to salvage therapy (Table 3). In the HIFU arm, 2/7 patients had ipsilateral recurrence and 5/7 had bilateral disease: in particular, two patients presented Gleason 6 (3 + 3) recurrence, two patients had Gleason 7 (3 + 4), two had Gleason 7 (4 + 3), and one had a Gleason 8 (4 + 4) recurrence. Nonetheless, 7 (13%) more patients in the HIFU arm required a complementary HIFU treatment on the contralateral lobe during follow-up, after developing a contralateral PCa. No patient died of PCa on follow-up, while 6 men died of other causes (5 HIFU vs 1 RALP, p = 0.11).
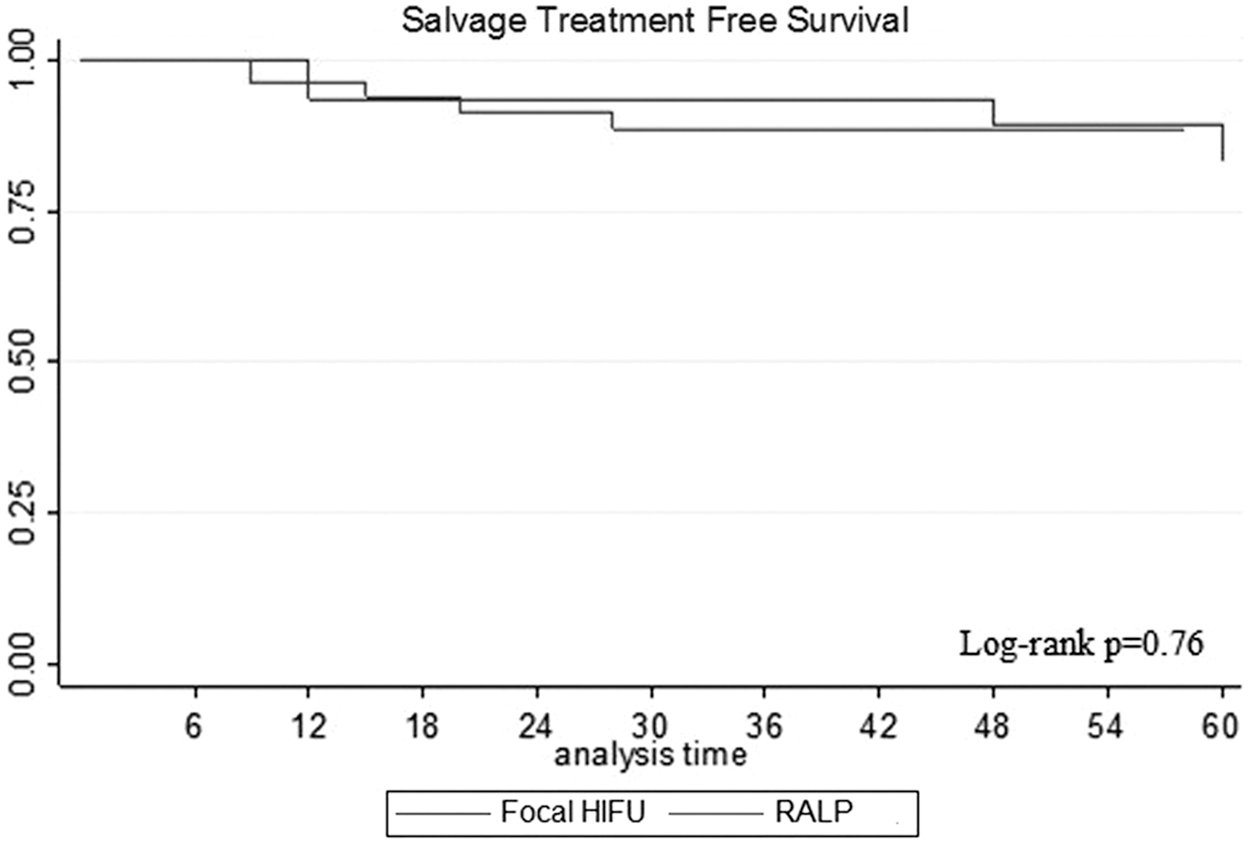
Exploring salvage treatment free survival across the two techniques for unilateral prostate cancer. HIFU = high-intensity focal ultrasound; RALP = robot-assisted laparoscopic prostatectomy.
χ 2-test.
ADT = androgen deprivation therapy; EBRT = external beam radiation therapy.
Discussion
Urology is a dynamic surgical specialty, with revolutionary changes which are constantly occurring. Focal therapy for PCa, which is still considered experimental, 16 is a promising approach for localized PCa, as new genetic and clinical data are suggesting that the outcome of the disease is mainly driven by the index lesion. 6 The focalized treatment of the index lesion could therefore obtain similar oncologic outcomes to whole gland therapy, although reducing morbidity, particularly concerning continence and sexual potency. 17
In this retrospective matched-pair analysis, we compared functional and oncologic results of two diametrically different approaches to unilateral PCa. On the one hand, we offered radical treatment using RALP: indeed these patients had worse functional outcomes, with a slower recuperation of continence and a worse recovery of sexual function. On the other hand, patient undergoing focal therapy achieved better functional results, and this is not surprising given the inherent tissue sparing approach of focal therapy. Of note, median age in the focal therapy arm was 73 years, and it is known that age is the most important risk factor for urinary incontinence following radical treatment of PCa. 18,19 As such, an 82% full continence rate at 1 month after surgery, in such an “old” group of men, is not only better than our RALP results but also is indeed appealing especially for older men in whom surgery may determine major aggravation of continence status. 18,19 A similar consideration can be made for our potency results: clearly, a tissue sparing approach determined a much lower negative impact of erectile function, especially in older men with a baseline worse erectile function. 18,20 Concerning postoperative complications, these are low across both techniques and are mainly represented by the need of prolonged urinary drainage or urinary tract infections, both classified as minor complications. 21
All the other comparing oncologic outcomes of a radical vs focal therapy can be tricky. Indeed, in a tissue sparing procedure as HIFU hemiablation, healthy prostatic glands (which physiologically produce PSA) are by definition left behind. As such, the definition of biochemical recurrence is still a matter of debate across experts in the field and no consensus exists. 5 Frequently, researchers have used the Phoenix criteria used after radiotherapy for PCa 13 : yet, these criteria are suboptimal in focal therapy. In our center, we use Phoenix criteria to prompt diagnostic work-up, including multiparametric MRI and prostate biopsies. In the RALP group, BCR was experienced by 6/55 patients (11%), as similar to other low and intermediate risk series. 16,22,23 Similarly, 7/55 patients in the HIFU arm required salvage treatment as a consequence of the failure of HIFU hemiablation to control PCa. Thus, it appears that the oncologic control of the index lesion determined by HIFU hemiablation was similar to that obtained by RALP, when considering treatment failure (i.e., the need for salvage radio or hormone therapy). These results are encouraging, although they must be handled with care. A great difference across the two arms of our study is that in the RALP group, unilateral disease is determined on whole-mount pathologic examination, while in the HIFU such “unilateral status” is defined by MRI and targeted biopsies. As such, while in the RALP group we are sure that all patients truly harbored only unilateral disease, in the HIFU groups there might have been patients with bilateral disease, erroneously found to have unilateral PCa, contributing to the number of men who failed treatment and required salvage therapy. Clearly, adequate patient selection and perfect preoperative diagnosis are vital when performing focal therapy. As such, it may be possible that part of the disease progressions observed in the HIFU arm (requiring salvage treatment) is due to inaccurate diagnosis, rather than treatment failure.
When leaving a prostatic lobe untreated, patients remain at risk of developing contralateral PCa. 5 This is an inherent aspect of focal therapy, which is normally discussed with the patient before surgery. In fact, it can be considered that active surveillance and focal therapy are two complementary strategies of the same therapeutic pathway. 24 Moreover, PCa can be already present in the contralateral untreated lobe as a consequence of a missed diagnosis on biopsy. In our center, where mp-MRI is incorporated to MRI-guided fusion targeted biopsies, 10 this is especially true in the case of OMS 2016 Grade I PCa (Gleason 6), which can be underdiagnosed on multiparametric MRI. 25 In the current study, 7/55 (13%) extra patients required secondary HIFU hemiablation of the contralateral lobe, due to the development of contralateral PCa, which is generally considered acceptable by experts of focal therapy. 5 These patients may be considered a failure of our approach and must be kept in mind when counseling men on PCa treatment. Although the consequences of contralateral recurrence are usually minor compared to salvage therapy, its exclusion from failures in the current study may have induced a bias with undue advantage for HIFU hemiablation over RALP and as such represents a limitation of the study.
Our study is not devoid of limitations. First, comparing focal therapy to radical surgery may seem like comparing apples and pears; our results must be interpreted with caution. Moreover, the follow-up is limited and insufficient to draw definite conclusions on oncologic control obtained by our focal therapy. Finally, the study is retrospective in nature, and the number of patients is limited.
Conclusions
In this retrospective matched-pair analysis, HIFU hemiablation of the prostate was comparable to RALP in controlling localized unilateral PCa, with no significant differences in the need for salvage therapies. However, patients undergoing focal treatment of PCa remain at risk of contralateral PCa, which required a contralateral hemiablation in 7/55 (13%) of our patients. HIFU hemiablation of the prostate was also associated to significantly better urinary continence and erectile potency recovery. Accurate patient selection remains vital, and larger prospective trials are needed to confirm our findings.
Footnotes
Author Disclosure Statement
No competing financial interests exist.