
Abstract
Introduction:
Accurate determination of ureteral length (UL) and appropriate stent length remains a challenge. The objective of this study was to describe an intraoperative technique to measure UL and determine appropriate stent length, and to compare this technique with other methods of determining appropriate stent length.
Methods:
Patients undergoing ureteroscopy requiring postoperative stenting and who had a preoperative CT were prospectively identified. Gender, age, height, body mass index, L1 to L5 lumbar height on CT, and surgeon's estimate of UL were recorded. UL was measured using four methods: direct measurement with a ureteral catheter, ureteropelvic junction (UPJ) to ureterovesical junction distance on axial and coronal CT, and using a novel intraoperative radiographic technique. Radiographic measurement was performed using a radiographic nipple marker affixed to the skin over the ureteral orifice (UO) and an angiographic catheter with radiopaque markings at 1 cm intervals. UL was the distance from the UPJ to the marker at the UO measured using the catheter markers. Correlation between direct measurement and the recorded variables and methods of ureteral measurement were calculated. Stent length was chosen based on radiographic measurement. Stents were deemed of appropriate length if they showed a proximal coil in the renal pelvis and a distal coil in the bladder without crossing midline.
Results:
Twenty-five ureters from 23 patients were included. Radiographically measured UL was strongly correlated with direct measurement. (r = 0.873, p < 0.01). Coronal and axial CT ULs were significantly associated with direct measurement (p < 0.05). Height, lumbar height, and surgeon's estimate of UL were not. Stents were deemed of appropriate length in 23/25 cases (92%).
Conclusions:
This new method for radiographic UL measurement is strongly correlated with directly measured UL. A length of stent chosen based on radiographic UL resulted in an appropriate stent length.
Introduction
U
The primary objective of this study was to describe our experience with an intraoperative technique to measure ureteral length (UL) and determine appropriate stent length, and to compare this technique with other methods of estimating UL. The secondary objective was to evaluate the appropriateness of fit of stents placed based on this measurement.
Materials and Methods
Approval from the Research Ethics Board of St. Michael's Hospital was obtained to perform a prospective study on patients undergoing ureteroscopy at our institution between March 19, 2015, and September 3, 2015. Patients expected to require postoperative stenting and who had a preoperative CT were prospectively identified and included in the study. Exclusion criteria included pediatric patients (age <18 years old), patients with congenital kidney anomalies (horseshoe kidney, ectopic kidney, etc.) or anomalous urinary tracts (ileal conduit, ileal ureter, ureteral reimplant, and severe pelvic organ prolapse), and lack of a preoperative CT. Study patients were representative of typical patients treated with ureteroscopy at our institution. None were prestented.
Patient gender, age, height, body mass index, and lumbar height on CT scout and coronal CT were recorded. The operating surgeon's estimate of likely UL, and subsequently appropriate stent length, was recorded before instrumentation. Lumbar vertebral height (L1–L5) was measured on CT scout radiograph and on coronal reconstructions. The operating surgeon's preoperative estimate of appropriate stent length was recorded before any measurements of UL.
UL was measured using four methods: direct measurement with a graduated ureteral catheter, ureteropelvic junction (UPJ) to ureterovesical junction (UVJ) distance on axial and coronal CT, and using a novel intraoperative radiographic technique.
Direct measurement of ULcath was performed using a graduated 5F ureteral catheter with markings at 1 cm intervals to perform a retrograde pyelogram. The tip of the catheter was fluoroscopically positioned at the UPJ, and the length of the ureter was measured by endoscopically viewing the catheter marker emanating from the ureteral orifice (UO), with the bladder near empty.
CT measurements of UL were performed preoperatively using both the axial (ULax) and coronal (ULcor) reconstructions. ULax was calculated by determining the number of cuts between the UPJ and UVJ, and multiplying this by the slice thickness. The UPJ was defined as the slice where the caliber of the renal pelvis narrowed to match the proximal ureter, and the UVJ was defined as the slice where the distal ureter could be seen entering the bladder wall. ULcor was determined by measuring the straight linear distance between the UPJ and UVJ on the coronal reconstruction.
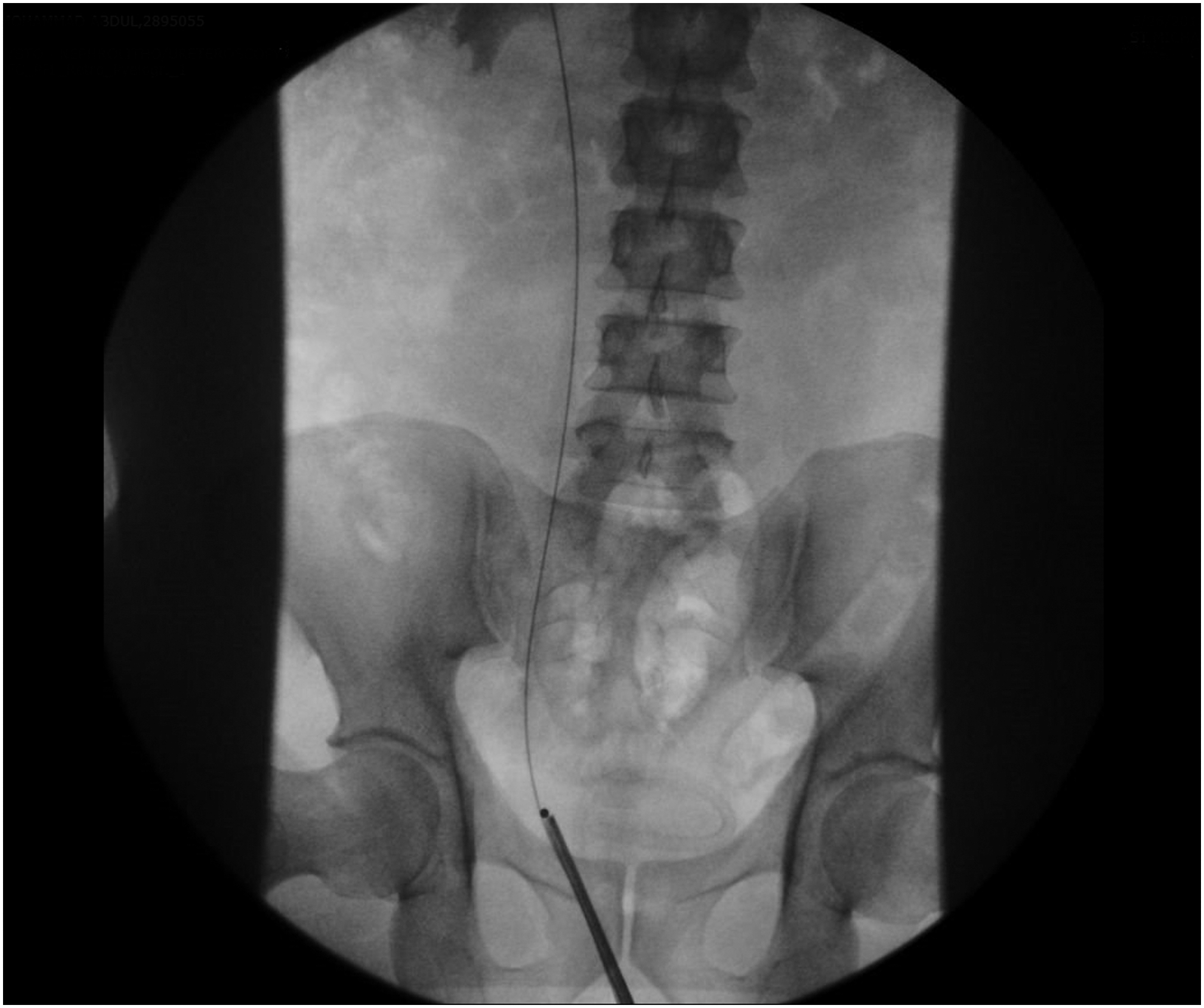
To perform the radiographic measurement, the tip of the cystoscope or ureteroscope was positioned at the UO and viewed under fluoroscopy. A radiographic nipple marker (which is a metal bead on an adhesive strip) was affixed to the skin over the UO to mark its location fluoroscopically. A 5F open-ended angiographic catheter (Cook Medical) with radiopaque markings at 1 cm intervals out to 24 cm was advanced over a 0.038 sensor guidewire (Boston Scientific), used to perform a retrograde pyelogram, and the tip positioned at the UPJ. UL was the distance from the UPJ to the marker at the UO using the radiopaque catheter markers (ULrad), with the bladder near empty. For ureters measuring longer than the 24 cm covered by the catheter markings, a visual estimate was performed, using the gradations between 22 and 24 cm as a scale for reference (Figs. 1 –3).
Nipple marker affixed to skin above UO. UO, ureteral orifice.

Ureteral length measured using angiographic catheter markers.
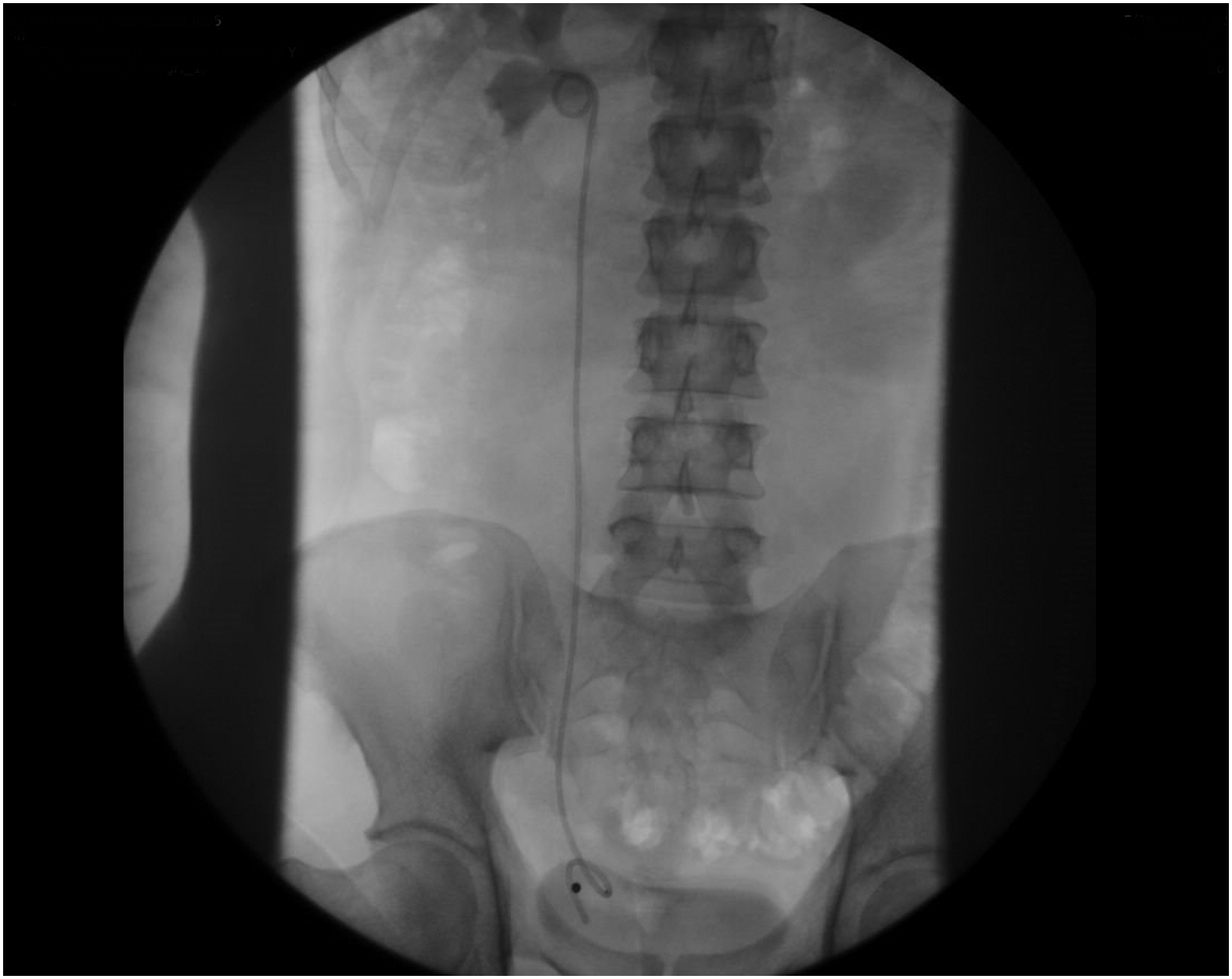
Stent length chosen based on radiographically measured ureteral length.
Placement of a 22-, 24-, or 26-cm 6F Double-J stent (Cook Medical) was performed, with stent length chosen based on UL obtained through radiographic measurement (ULrad). Where ULrad was determined to be between available stent lengths, a longer stent of the nearest length was used (e.g., if ULrad was 23 cm, a 24 cm stent was placed). Stents were deemed of appropriate length if they showed a proximal coil in the renal pelvis and a distal coil in the bladder without crossing the midline on intraoperative fluoroscopy, and an image was captured as a record of stent position.
Correlation between direct ureteral measurement and the recorded variables and methods of UL measurement were calculated. All analyses were performed with use of SAS software version 9.2 (SAS Institute Inc.). A p value <0.05 was considered significant.
Results
Twenty-five ureters from 23 patients (16 men and 7 women) were included in the study. Twenty-four patients were originally consented, but one female patient was excluded from the study because of severe bladder neck prolapse. All patients underwent ureteroscopy for stone disease or hydronephrosis.
Patient height and lumbar vertebral heights on CT and CT scout were poorly correlated with directly measured ULcath. The surgeon's preoperative estimate of UL was also poorly correlated with ULcath (r = 0.176, p = 0.399).
Moderate correlation was found between CT measurements of UL on both the coronal (ULcor; r = 0.646, p < 0.001) and axial (ULax; r = 0.455, p = 0.019) reconstructions. Radiographic measurement of UL was effective in all cases, and was strongly correlated with ULcath (ULrad; r = 0.833, p < 0.001) (Table 1).
N.B. r ≥ 0.8 denotes a strong correlation, r > 0.5 <0.8 denotes a moderate correlation, and r ≤ 0.5 denotes a weak correlation.
ULcath = ureteral length measured directly by catheter; ULax = ureteral length measured on axial CT; ULcor = ureteral length measured on coronal CT.
Stents were placed in all patients undergoing ureteral measurement. Twenty-three stents placed based on ULrad were deemed to be of appropriate length (23/25, 92%). Two stents were evaluated as being suboptimally positioned. In one case, this was because of the proximal stent coil had been placed in an upper pole calix. As the distal coil was complete and within the bladder, it was not repositioned. In the second case, there was a very small renal pelvis that precluded proximal coil formation, and as such the distal coil partially crossed the bladder midline. No stents were found to be too short, and no stents were accidentally advanced excessively far up the ureter such as to require repositioning.
Discussion
Ureteral stents are commonly used for the relief of ureteral obstruction, or after urologic procedures to maintain drainage and prevention of secondary obstruction caused by edema, but are associated with significant morbidity. The Ureteral Stent Symptom Questionnaire (USSQ) developed and subsequently validated by Joshi and colleagues has allowed for a clearer understanding of the frequency and magnitude of stent-related symptoms and their impact on patient's QoL. 13 Further studies of stent-related morbidity utilizing the USSQ and similar tools have made it clear that these symptoms are common, with rates of significant LUTSs and pain of up to 80%. 1 –5
Although it remains a challenge to predict which patients will experience symptoms related to stent placement, and to what degree, certain factors related to the stents themselves that may contribute have been identified. These include excess stent within the bladder (particularly with the distal coil crossing the bladder midline), 2,4,5,7,14,15 upper caliceal positioning of the proximal coil, 7 duration of stenting, 7 and stent composition and design. 16 Of these, stent length and positioning are most directly controlled and may be optimized by the surgeon.
Choosing an appropriate length of stent requires the surgeon to know the precise length of ureter in question. Although measurement with a graduated ureteral catheter under cystoscopic direct vision is considered the gold standard for determining true UL, this is rarely done in practice as it is time consuming and often requires repeat instrumentation. In addition, this may not be possible at the start of a procedure because of the presence of an obstructing stone. Multiple predictors of UL have been proposed.
Despite its common use in choosing stent length, multiple studies have consistently found that patient height is poorly correlated with UL. 17 –20 This finding is again confirmed by this study, in which a poor correlation was found between patient height and ULcath (r = 0.352). Lumbar vertebral height on KUB or CT has been proposed as a more accurate alternative to patient height for the estimation of UL, but was not found to significantly correlate with directly measured UL in a study from our institution. 21 This finding was further confirmed in this study for both lumbar vertebral height on scout film (r = −0.011) and measured on coronal CT (r = −0.082).
In clinical practice, it is common for stent length to be chosen based on the surgeon's estimate of a patient's UL, which in this study was found to be poorly correlated with ULcath (r = 0.176). This is likely because of the influence of patient height on the surgeon's estimate, and is not surprising as height was also found to be poorly correlated with ULcath. A single staff surgeon (R.J.D'A.H.) participated in this study and performed all estimations. To our knowledge, this is the first study to evaluate the common practice of choosing a stent length based on the surgeon's estimate.
CT axial cuts have been shown to have moderate correlation with directly measured UL. 22 By applying a correction factor of 20% to axial CT measurements, Shrewsberry et al. were able to increase their correlation with directly measured length (r = 0.979). 18 A prospective study at our institution also found moderate correlation between ULcath and both axial and coronal CT measurements (r = 0.630 and 0.640, respectively). 21 This study also found a weak-to-moderate correlation between CT measurements and ULcath (ULax r = 0.455; ULcor r = 0.646).
This study describes our prospective experience with a novel intraoperative technique for the radiographic measurement of UL. The development of this technique arose from the desire to find an efficient way to accurately measure UL and help in the selection of an appropriate stent length, but which would not add significant time to the case. Direct measurement may not be possible at the start of a case because of an obstructing stone or lesion that precludes passage of the ureteral catheter up to the UPJ, and when performed at the end of a case requires reinstrumentation with the cystoscope. This method allows for accurate intraoperative measurement of UL without reintroduction of the cystoscope. The technique described in this study was found to be highly correlated with direct ureteral measurement (r = 0.833, p < 0.001). The angiographic catheter utilized was of the same caliber as our standard ureteral catheters (5F), and was used in an identical manner. We are currently working with industry to have three radiopaque markers added to our standard 5F ureteral catheters and to include a sterile nipple marker in the catheter packaging.
Marking the radiographic location of the UO has the advantage of aiding in proper stent positioning. Studies of the fluoroscopy location of the UO relative to bony landmarks, including one from our institution, have shown differences between men and women. In men, the UO tends to be located superior to the upper border of the pubic ramus (PR) when the bladder is empty (83%–100%), and nearly always when it is full (95%–100%). 9 –12,23 In women, the location of the UO shows more variability, being located superior to the upper border of the PR when the bladder is empty in only 27% to 66% of cases. Also, its position is more influenced by bladder filling, being most commonly located behind the pubis when the bladder is full (75%). 9 –12,23 However, the exact fluoroscopic position of the UO of any individual patient is unknown at the time of stent placement without a marker.
Rates of complications related to stent positioning have been reported to be as high as 9%, with the majority of cases being proximal migration of the stent. 9 –12 Marking the UO before stent placement allows the surgeon greater confidence when placing a stent fluoroscopically at the end of a case. It should be noted that, because the bead is affixed to the patient's skin, care must be taken not to distort the skin (such as with excessive penile traction) during stent placement, as this may move the bead relative to the UO. It is also advisable to place the stent with a degree of bladder fullness comparable with that when the UO was marked. At the end of a case, before stent placement, a retrograde pyelogram is usually performed to assess the correct placement of the proximal coil. In this study, this was done using the open-ended angiographic catheter. Minimal additional radiation is required to observe the lower end of the catheter as it relates to the markers at the UO.
This study did not measure stent symptoms through the use of a questionnaire, such as the USSQ, as this has been done in a number of published studies. These studies consistently show a relationship between stent length and LUTSs. The characteristics of an inappropriate stent as defined in this study reflect factors identified in previous studies as contributing to worsening symptoms. 2,4,5,15 This study was designed to demonstrate that it is possible to place the correct length of stent in virtually every patient. Further studies including follow-up imaging to rule out postoperative stent migration or displacement, as well as evaluation of stent-related symptoms using the USSQ, would be valuable.
Conclusions
This new method for radiographic UL measurement is strongly correlated with directly measured UL. A length of stent chosen based on radiographically measured UL resulted in an appropriate stent length and good stent position in 92% of cases.
Footnotes
Acknowledgments
This material has been presented at the Canadian Urological Association Annual Meeting 2016. Cook Medical provided angiographic catheters.
Author Disclosure Statement
K.B., D.G., R.J.S., and M.F. have no competing financial interests. K.T.P. is aBoston Scientific Corporation consultant/advisor/meeting participant/lecturer; Paladin Labs consultant/advisor; Ferring Canada consultant/advisor; Amgen consultant/advisor; Janssen consultant/advisor; and Cook Medical, Inc. support for fellowship program. R.J.D'A.H. is a Cook Medical, Inc. support for fellowship program and Cook Medical royalty agreement.