
Abstract
Objectives:
Although previous studies have indicated that stone heterogeneity can affect extracorporeal shockwave lithotripsy (SWL) outcomes, there is no established measurement of stone heterogeneity on CT imagery. We investigated whether variation coefficient of stone density (VCSD) can predict shockwave success.
Materials and Methods:
We conducted a retrospective review of 245 patients with urinary calculi who had undergone SWL. We compared the predictive powers of treatment success between VCSD and other parameters associated with CT attenuation. In addition, we performed logistic regression analysis to identify the factors contributing to treatment success. Treatment success was determined within 3 months after first treatment using noncontrast CT.
Results:
The treatment success rate was 47.8% (117/245 cases). From receiver operating characteristic curves for treatment success, area under curve of VCSD (0.7181) was larger than that of mean stone density (MSD) (0.6384, p = 0.09) and standard deviation of stone density (0.5412, p < 0.01). Multivariate analysis revealed that MSD (p = 0.028) and VCSD (p < 0.001) independently predicted the outcome. Categorized by stone location, VCSD was the independent significant predictor for SWL outcomes in both kidney (p = 0.047) and ureteral calculi (p < 0.001).
Conclusions:
We found that VCSD can be a novel predictor of SWL success. The development of nomograms or scoring systems, including VCSD, can assist in the decision process for patients and minimize unnecessary delay in treatment of urolithiasis.
Introduction
E
Factors, such as stone size, stone location and number of stones, were reported to be predictors of SWL success. 5 In addition, there has been increasing evidence that noncontrast CT parameters, such as skin-to-stone distance (SSD) and mean stone density (MSD), can predict SWL success. 6 –16 The role of SSD as a predictor of SWL success remains controversial, 10,11,15 –18 whereas MSD has been widely recognized as a predictor of SWL outcome. According to the American Urological Association guideline, patients with MSD greater than 900 to 1000 HU have less effective results with SWL. 19 Previous reports indicate that stone heterogeneity can also affect SWL success. Zarse and colleagues have reported that the internal structure of calcium oxalate monohydrate calculi on CT imagery predicts lithotripsy fragility in vitro. 20 Moreover, Kim and colleagues have reported correlation of stone structure and morphology of cystine stone on CT imagery with fragility by SWL. 21 However, there is no established measurement of stone heterogeneity on CT imagery. Therefore, there is a need to identify a CT parameter that represents stone heterogeneity and to verify its predicting capability for SWL success.
We hypothesize that variation coefficient of stone density (VCSD) represents stone heterogeneity and can predict SWL outcome. In this study, we examined VCSD as well as previously reported parameters, including stone volume, SSD, MSD, and standard deviation of stone density (SDSD) as predictors of SWL success after a single session.
Materials and Methods
Patient selection
Between January 2008 and January 2016, 347 adult patients with radiopaque renal and ureteral calculi underwent extracorporeal SWL at the Wakayama Medical University Hospital. Of these, 245 patients with pretreatment noncontrast CT examination were enrolled in this study. Exclusion criteria were patients who were not followed up at our hospital, those who underwent SWL for the purpose of pretreatment for URS or PCNL, and those whose treatment outcomes could not be ascertained. This retrospective study was approved by the Institutional Review Board of Wakayama Medical University.
Treatment
All lithotripsy treatments were performed using Lithotripter S (Dornier MedTech, Germany). Patients were treated with up to a maximum of 3000 shocks for renal and upper ureteral stones and up to 4000 shocks for mid and distal ureteral stones with a gradual augmentation of power at 70 shocks per minute. Stones were targeted with fluoroscopy at regular intervals throughout treatment.
Predictors
Patient demographics (age and sex) and clinical data (stone location, stone volume, MSD, SDSD, VCSD, SSD, hydronephrosis, and urinary drainage) were collected retrospectively. Stone volume, MSD, SDSD, VCSD, SSD, and the presence of hydronephrosis were evaluated by a noncontrast CT. A single radiologist reviewed all CTs and determined these factors using a WebPACS system. Stone volume was calculated by a long diameter (a) and short diameter (b) on axial images and longitudinal diameter (c) on coronal images, and defined as (a × b × c)/2. Stone density was measured using bone windows on the magnified, axial noncontrast CT of the stone in the maximal diameter by making a digitizing free-hand trace of the stone edge without including adjacent soft tissue (Fig. 1). MSD and SDSD were defined as the mean value and the standard deviation value of CT attenuation in the traced region, respectively. VCSD was defined as the variation coefficient value of CT attenuation and calculated by ([SDSD]/[MSD]) × 100 (%). SSD was defined as the mean vertical distance from the center of the stone to the skin measured on a supine noncontrast CT image at 0°, 45°, and 90° as suggested by Pareek and colleagues. 6
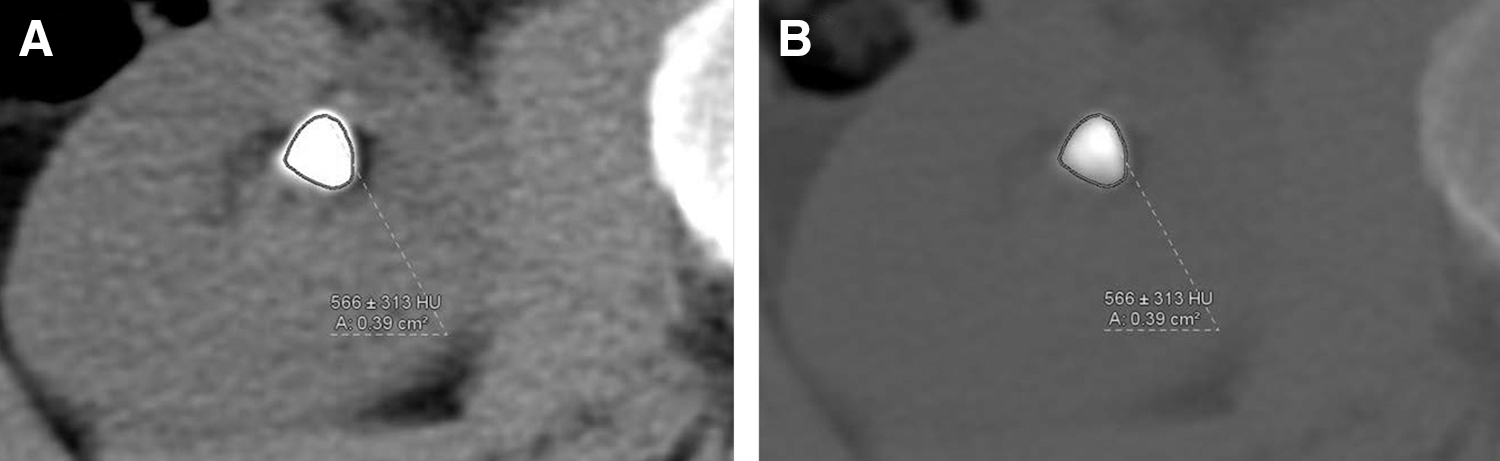
Measurement of MSD, SDSD, and VCSD on axial images of noncontrast CT.
Outcomes
Effective SWL was determined using noncontrast CT within 3 months after first SWL treatment and was defined as the absence of stones or clinically insignificant residual fragments less than 4 mm in maximum diameter. Patients who required retreatment or who required adjunctive treatment (URS, PCNL, ureteral stenting, or nephrostomy tube placement) were deemed unsuccessful cases.
Statistical analyses
A statistical comparison of patient demographics and stone parameters was performed using the chi-square tests and Mann–Whitney U tests. Univariate and multivariate analyses were performed to identify the factors contributing to clinically significant residual stones after the first SWL session in logistic regression analysis. Receiver operating characteristic (ROC) curves were plotted to compare the predictive powers for SWL success among MSD, SDSD, and VCSD. Correlation between MSD and SDSD was examined using the nonparametric Spearman rank method. For all statistical tests, p < 0.05 was considered significant. All statistical analyses were performed using JMP Pro 12 (SAS Institute).
Results
Patient demographics and stone parameters are summarized in Table 1. The median age of the total number of patients was 59 years and 162 patients (66.1%) were male. Median stone volume was 211.6 mm3. Median MSD, median SDSD, median VCSD were 545.0, 283.0 HU, and 54.0%, respectively. Of the 245 cases, 97 patients were treated for kidney stones and 148 patients were treated for ureteral stones. Stone volume in patients with kidney stones was significantly larger than that in patients with ureteral stones (p < 0.01).
Continuous variables are shown in “median (quartile)” form.
MSD = mean stone density; SSD = skin-to-stone distance; SDSD = standard deviation of stone density; VCSD = variation coefficient of stone density.
In total, 117 and 128 patients were classified as successful and unsuccessful groups, respectively. Comparison of patient characteristics and stone parameters between successful and unsuccessful cases is shown in Table 2. Patients in the successful group had a statistically significant younger age (p = 0.02), lower percentage of multiple stones (p = 0.02), and smaller stone volume (p < 0.01) than those in the unsuccessful group. In addition, in the successful group, MSD was significantly lower (p < 0.01) and VCSD was significantly higher (p < 0.01) than those in the unsuccessful group. On the contrary, there was no significant difference in SDSD between the two groups (p = 0.26). Median period between SWL and CT estimation was significantly longer in the successful group compared with the unsuccessful group (p = 0.04).
Continuous variables are shown in “median (quartile)” form.
SWL = extracorporeal shockwave lithotripsy.
Figure 2 shows the ROC curves of radiographic parameters associated with CT attenuation for prediction of SWL success. Area under curve (AUC) of MSD, SDSD, and VCSD, was 0.6384, 0.5412, and 0.7181, respectively. AUC of MSD (p < 0.01) and VCSD (p < 0.01) was significantly larger than that of SDSD. Moreover, AUC of VCSD was larger than that of MSD, although the difference was marginally significant (p = 0.09).

Receiver operating characteristics of radiographic parameters associated with CT attenuation for SWL success. SWL, extracorporeal shockwave lithotripsy.
Table 3 shows the results of univariate and multivariate logistic regression analyses of factors that predict residual stones after first SWL session for overall patients. In univariate analysis, increasing age (p = 0.023), multiple stones (p = 0.021), increasing stone volume (p < 0.001), increasing MSD (p < 0.001), and decreasing VCSD (p < 0.001) were associated with residual stones. On multivariate analysis, increasing MSD (p = 0.028) and decreasing VCSD (p < 0.001) were independent significant predictors of residual stones.
CI = confidence interval; OR = odds ratio.
Table 4 shows the results of univariate and multivariate analyses for kidney stones. In univariate analysis, lower caliceal stones (p < 0.001), increasing stone volume (p < 0.001), increasing MSD (p = 0.040), and decreasing VCSD (p = 0.003) were associated with residual stones. On multivariate analysis, lower caliceal stones (p < 0.001), increasing stone volume (p = 0.039), and decreasing VCSD (p = 0.047) were independent significant predictors of residual stones.
Table 5 shows the results of univariate and multivariate logistic regression analyses for ureteral stones. In univariate analysis, increasing age (p = 0.033), multiple stones (p = 0.020), increasing stone volume (p < 0.001), increasing MSD (p < 0.001), decreasing VCSD (p < 0.001), and urinary drainage (p = 0.039) were associated with residual stones. On multivariate analysis, decreasing VCSD was the only independent significant predictor of residual stones (p < 0.001).
Discussion
In the present study, we introduced the concept of stone heterogeneity based on CT attenuation and examined VCSD as a possible predictor of SWL outcome. To the best of our knowledge, this is the first report about the clinical significance of VCSD for SWL outcome. We revealed that VCSD was an independent predictor of SWL outcomes in both kidney and ureteral stones.
The representative predictor of SWL outcome associated with CT attenuation is MSD. As described above, MSD has been reported as a useful parameter to affect SWL success 7 –12,14 –17,22,23 and is widely used in the clinical field. However, MSD can represent only the average stone hardness, and the heterogeneity of stone composition is not reflected. While previous studies have suggested that stone heterogeneity is an important factor for SWL success, 20,21 there are few reports about a useful index that represents the stone heterogeneity based on CT parameters. Recently, SDSD has been reported to be an independent predictor of SWL success in patients with ureteral calculi and a useful parameter for stone fragility in a large retrospective study by Lee and colleagues. 24 While SDSD is considered to represent stone heterogeneity, it can be affected by MSD, an index of stone hardness, since standard deviation is generally influenced by mean value. In contrast, variation coefficient is the standard deviation divided by the mean value and is generally used to compare dispersion between multiple groups with different average values. We speculated that VCSD represented stone heterogeneity better than SDSD.
In the current study, it is suggested that VCSD can be a novel predictor of SWL success. In comparison with other factors associated with CT attenuation, VCSD has stronger predictive power on SWL success than MSD and SDSD (Fig. 1). Moreover, in multivariate analysis, higher VCSD is the independent significant predictor of SWL success (p < 0.001) in overall patients (Table 3). When categorized by the location of stones, VCSD was the independent significant predictor of SWL outcome in both kidney and ureteral calculi (Tables 4 and 5). High VCSD indicates large dispersion of stone density, that is, heterogeneous internal structure of the stone. Since previous studies suggested that stone heterogeneity contributed to the frangibility of stones by SWL, it was reasonable that VCSD in the successful cases was higher than that in unsuccessful cases. On the contrary, SDSD is not statistically significant in the present study. Also, MSD and SDSD have a strong positive correlation (Fig. 3, Spearman's rank correlation coefficient 0.8699, p < 0.0001) and this might be the reason why higher SDSD was not an independent factor for SWL outcome. From these results, we believe that VCSD is a more suitable factor that represents stone heterogeneity by eliminating the influence of stone hardness than SDSD. From the ROC curve analysis, the optimal cutoff value of VCSD for SWL success was 51.3% in overall patients. SWL success rates of patients with VCSD ≥51.3% and those with VCSD <51.3% were 64.5% and 26.2%, respectively. While further studies are necessary to apply VCSD in the treatment decision-making process, these results can provide useful information for physicians and patients.
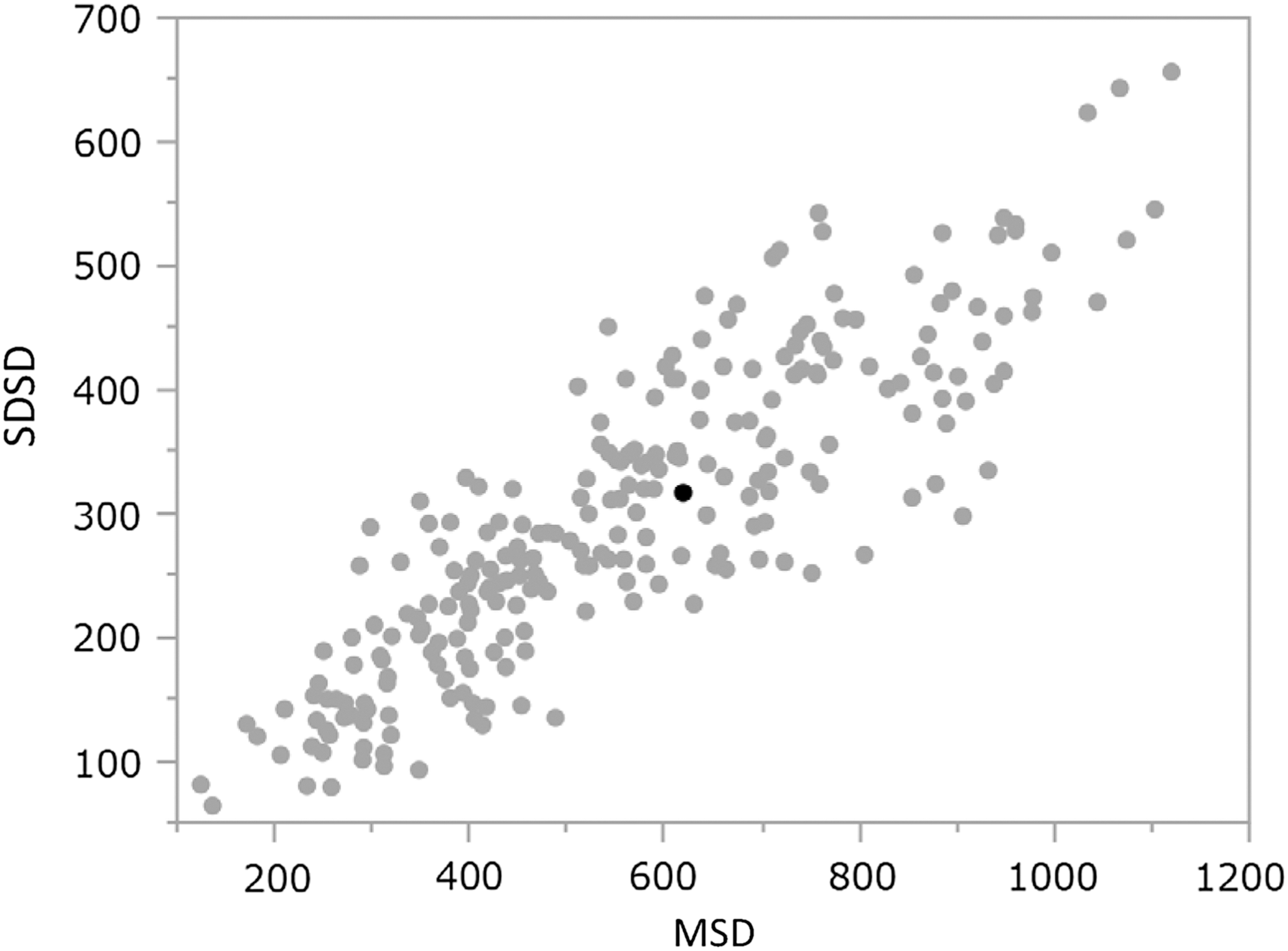
Scatterplot of the relationship between MSD and SDSD.
In patients with kidney stones, lower caliceal stones (p < 0.001) and stone volume (p = 0.039) were also significant predictors of SWL outcome. These results are in agreement with previous studies. 10 –12,25,26 In contrast, in patients with ureteral stones, stone volume was not a significant predictor. This may be because the size of ureteral stones was significantly smaller and distributed in a narrower range compared with kidney stones (Table 1), leading to the smaller influence on the outcome. In addition, the transverse diameter of stones might have a greater impact on SWL success in the treatment of ureteral calculi than stone volume as reported by Salman and colleagues. 27
While the efficacy of SSD as a predictor of SWL outcome remains controversial, 10,11,17,18 several studies have reported that SSD can predict SWL outcome. 7,12,13,22,28 However, SSD was not a significant predictor of SWL success in our study. We suppose that this might be because the number of morbidly obese patients is relatively small in Japan and SSD in our cohort was small with a narrow distribution compared with the previous studies.
MSD was an independent significant predictor of SWL outcome in overall patients, although it was not independently significant for kidney calculi or ureteral calculi categorized by stone location. This does not necessarily deny the efficacy of MSD as a predictor, rather may be attributed to the decrease in the number of patients included in each group when they were categorized as the kidney calculi group and ureteral calculi group. Hence, a future large-scale study is needed.
The present study has several limitations. First, this was a retrospective analysis undertaken at a single center, which may limit the generalization of the results. However, the number of patients included in our study is comparable to previous studies. Second, the timing of evaluating SWL outcome was inconsistent, although the SWL outcome was determined using noncontrast CT within 3 months after a first SWL treatment. A multicenter prospective analysis is required to overcome these limitations.
In conclusion, the results of this study indicated that VCSD was independently associated with SWL outcome in patients with upper urinary tract calculi. Therefore, VCSD can be a novel useful predictor for SWL success. The development of nomograms or scoring systems, including VCSD, may assist in the decision process for patients and minimize unnecessary delay in treatment of urolithiasis.
Footnotes
Acknowledgment
We thank Prof. Shimokawa for assistance in statistical analyses.
Author Disclosure Statement
No competing financial interests exist.