
Abstract
Objective:
The Triple D scoring system is defined as novel and simple nomogram using the main parameters (skin-to-stone distance, stone density, and volume) to indicate most appropriate patients for extracorporeal shockwave lithotripsy (SWL). We aimed to evaluate the accuracy of the Triple D scoring system in predicting SWL success rates.
Patients and Methods:
In two tertiary academic centers, charts were retrospectively analyzed of patients who had, between January 2014 and May 2016, been treated by SWL for radiopaque kidney stones. A total of 200 patients were enrolled into the study. Parameters were calculated for each of the three specified variables. Since one point was assigned for any parameter that was less than the cutoff value, Triple D scores ranged from 0 (worst) to 3 (best).
Results:
Stone-free status was achieved in 115 patients (57.5%), and 85 patients had one or more residual fragments (42.5%). Differences in stone characteristics, including stone location, density, and volume, were statistically significant in patients whether SWL achieved stone-free status or not (p < 0.001, p < 0.001, and p < 0.001, respectively). Triple D scores were significantly higher in patients treated with SWL compared with patients in whom SWL failed (p < 0.001). Triple D scores of 0, 1, 2, and 3 correlated with stone-free rates of 41.7%, 33.7%, 69.4%, and 97%, respectively. The multivariate analyses revealed that Triple D score and stone location were identified as independent factors affecting SWL success (p < 0.001 and p = 0.008, respectively). The mean number of SWL sessions was significantly higher in patients with SWL failure (p = 0.003).
Conclusion:
Our study externally validates that the Triple D scoring system is associated with SWL success in the treatment of renal and ureteral stones. Further studies are warranted to assess clinical usefulness and the accuracy of this nomogram in different patient groups.
Introduction
S
SWL has proved helpful in the treatment of kidney stones, but its success rate is variable. The decision of whether or not to use the process could be assisted by information gained from nomograms. Although still under investigation, clinical nomograms have been used to guide physicians and patients in selecting the most safe and effective treatment for kidney stones. Some authors have demonstrated that when information from nomograms was used to select patients to undergo SWL, success rates were higher. In practice, some are complex and confusing to use, 5,6 but recently Tran and colleagues reported a novel and simple nomogram they call the Triple D scoring system. Using computed tomography imaging, the Triple D describes three parameters: stone density, stone volume (SV), and SSD. The authors concluded that this scoring system may increase the success rates of SWL by indicating appropriate patients for the treatment. 7 Until now, however, Triple D scores have not been externally validated. This study aims to evaluate the accuracy of the Triple D scoring system in predicting SWL success rates.
Patients and Methods
In two tertiary academic centers, charts were retrospectively analyzed of patients who had, between January 2014 and May 2016, been treated by SWL for radiopaque kidney stones. Excluded from the study were 32 patients who had not been assessed with CT before SWL and 48 patients who had not completed treatment. Other exclusion criteria were patients under 18 years of age and those with renal abnormalities. At the end of evaluation, 200 patients were enrolled in the study. They were classified into two groups: those whose treatment was successful with SWL and those for whom it was not.
In this study, all patients were evaluated with CT before SWL. To reduce measurement bias, relevant parameters were examined by two urologists (F.O., A.T.) who were also blinded as to SWL results. Patients were evaluated with a kidney, ureter, and bladder radiograph (KUB) and urinary system ultrasonography (USG) 1 week after each SWL session. A maximum of three SWL sessions were given. The evaluation of stone-free status was done on each patient with both KUB and USG 12 weeks after the last SWL session. Patients were considered to be stone free if complete stone clearance was achieved.
Patient preoperative characteristics were recorded, including age, gender, body mass index (BMI), stone location, and the laterality of each stone. Also noted were CT evaluations of SV, SSD, and stone density (Hounsfield Unit-HU). SSD values were measured as described by Pareek and colleagues, and SV was determined by using the formula SV = π/6 × (Anteroposterior × Transverse × Craniocaudal diameters of the stone in mm) and symbolized as mm3. 8 Triple D scores were calculated based on the formula introduced by Tran and colleagues. 7 A stone's values were calculated for each of the three specified parameters (SSD, SV, and stone density). Since one point was assigned for any parameter that was less than the cutoff value (150 μL for SV, 600 HU for stone density, and 12 cm for SSD), Triple D scores ranged from 0 (worst) to 3 (best). 7
SWL technique
Under sedoanalgesia, the standard SWL session was performed as an outpatient procedure by two experienced staff with a Dornier Compact Sigma (Dornier MedTech GmbH, Wessling, Germany) and an ELMED Multimed Classic lithotripter (ELMED, Ankara, Turkey). The procedure was started with a frequency of 60 shocks/min and an energy level of 1, which was then increased to level 4. Frequency was increased to a maximum of 90 depending on patient tolerance. In each session, 2000 to 2500 shocks were delivered.
Statistical analysis
Data analysis was performed using the SPSS statistical package (version 22.0; SPSS, Inc., Chicago, IL). Continuous variables are reported as mean and standard deviation; categorical variables are reposted as percentages. Student's t-test was used for the comparison of continuous variables and the chi-square test for comparison of categorical variables in the two groups. Two-tailed p values <0.05 were considered statistically significant. Binary logistic regression analysis was used to identify independent predictors of stone-free status following SWL treatment. The area under the curve, calculated by the receiver operating characteristic curve, was used to assess the predictive ability of the Triple D scoring system.
Results
A total of 200 patients were enrolled into the study. Stone-free status was achieved in 115 patients (57.5%), and 85 patients had one or more residual fragments (42.5%). Success rate according to lithotripter type was not statistically significant between groups (p = 0.4). The age, gender, mean BMI, and stone laterality were similar between the groups (p = 0.7, p = 0.1, p = 0.9, and p = 0.2, respectively). Differences in stone characteristics, including stone location, stone density, and SV, were statistically significant in patients whether SWL achieved stone-free status or not (p < 0.001, p < 0.001, and p < 0.001, respectively). SSD values were significantly greater in patients with SWL failure (102 mm vs 93 mm, p = 0.008). Triple D scores were significantly higher in patients treated with SWL compared with patients in whom SWL failed (p < 0.001). Preoperative characteristics of patients and stone parameters are summarized in Table 1.
BMI = body mass index.
Triple D scores of 0, 1, 2, and 3 correlated with stone-free rates of 41.7%, 33.7%, 69.4%, and 97%, respectively. The multivariate analyses revealed that Triple D score and stone location were identified as independent factors affecting SWL success (p < 0.001 and p = 0.008, respectively). The mean number of SWL sessions was significantly higher in patients with SWL failure (p = 0.003). Outcomes of multivariate analyses are listed in Table 2 (Figure 1).
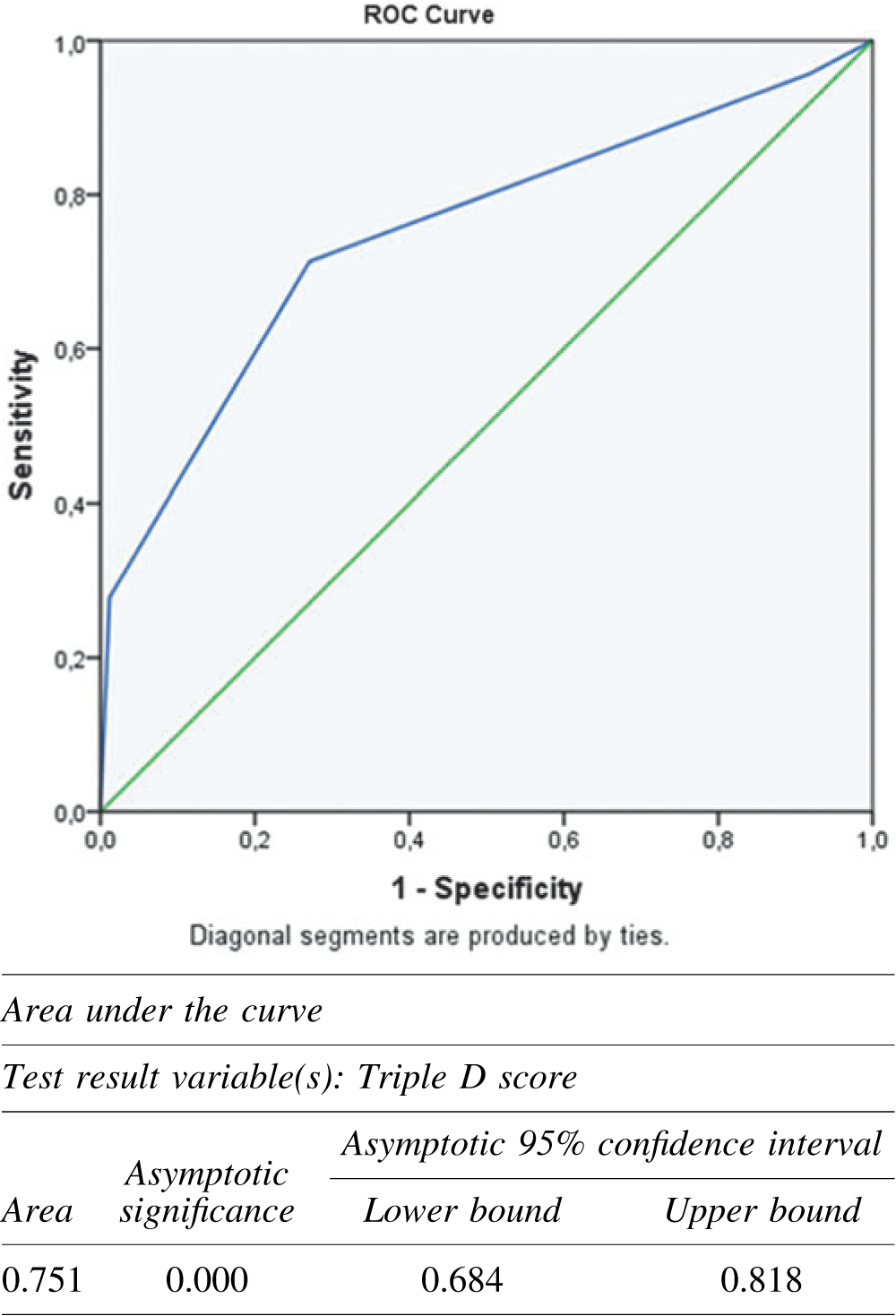
Diagonal segments are produced by ties.
Discussion
Despite the important role of SWL in the management of kidney stones, interest in SWL has decreased in recent years, largely because of advances in technology. Minimally invasive surgeries (including flexible ureteroscopy and percutaneous nephrolithotomy), along with improved success rates and decreased complication rates, have distinctly usurped SWL. 9 Second, studies investigating SWL report highly variable success rates—from 32% to 95%. 10,11 This variety indicates that many factors affect the outcome and decision-making and that patient selection is not simple. With the aim of predicting postprocedural outcomes and to help in choosing appropriate candidates to undergo the procedure, nomograms were developed.
Previous reports have stated that using nomograms in the selection of patients for SWL provides some benefits. First, the utility of nomograms prevents delays in definitive treatment. In addition, choice of appropriate treatment modality may minimize treatment-induced kidney damage and reduce the economic burden on the healthcare system. Even though these nomograms included important parameters and assure valuable reports on SWL success, the use of nomograms is not widely accepted in clinical practice, 12 possibly because of their impractical nature, being complex and confusing to use. Triple D remedies these problems because its scores utilize three parameters that exist routinely in CT imaging and facilitate use of this nomogram.
Negative correlation between stone burden and achieving success after SWL is well known, yet there is still no consensus about the most accurate method to calculate stone burden. It is generally evaluated by measuring a stone's maximum length or surface area, but this can be problematic because renal and ureteral stones have irregular three-dimensional forms with complex geometric properties. Bandi and colleagues found no significant correlation between maximal stone length and SWL success, but they did find significantly lower SV in patients who had achieved stone-free status following SWL (273 and 464 μL, p = 0.002). 13 Similarly, El-Nahas claimed SV as a predictive factor for disintegration of stones following SWL. 14
Previous reports emphasized that BMI is an important parameter in predicting SWL success, although some authors have concluded that the SSD value is a more predictive parameter than BMI due to different body types and body fat distribution among people and races. Pareek and colleagues revealed that SSD (using a cutoff value of 10 mm) was a much more powerful predictor than BMI and theorized that the traveling of shockwaves for longer distances is associated with attenuation of those shockwaves. 8 Similarly, Wiesenthal and colleagues reported that the cutoff value for SSD was 11 mm. 15
Many studies have clarified that stone density has a predictive value for SWL outcomes. In Wiesenthal's study and another by Wang, stones with >900 HU were more likely to fail after SWL. 15,16 Nakasato and colleagues have reported that success rates following SWL were significantly higher for stones <815 HU than for stones >815 HU (p < 0.02). 17 In another study, Ouzaid and colleagues reported that stone density of 970 HU was the most sensitive point in the determination of stone density. They achieved 96% stone-free rates for stones <970 HU and 38% stone-free rates for stones ≥970 HU (p < 0.001). 18
Before the Triple D, other nomograms had been produced to predict SWL outcomes, using factors related to SWL success in adult populations. Most, however, did not use scoring systems. Kanao's nomogram demonstrated that stone location, number, and size were predictive factors for estimating SWL success. 19 In addition to stone size, Wiesenthal and colleagues showed the importance of patient age and SSD for SWL success. Onal and colleagues created a nomogram for SWL treatment in children, which scored five parameters: age (range 0–2), stone burden (range 0–4), history of stone treatment (range 0–1), gender, and stone location (range 0–3). They emphasized that all these parameters had a predictive value for SWL success and that a higher score was associated with significantly lower stone-free rates (42.8% success in patients with scores >6, and 98.7% success in those with scores <2). 6
The Triple D scoring system developed by Tran and colleagues was the first nomogram to score possible predictive parameters for SWL outcomes in adult populations. Achieving stone-free rates of 21.4%, 41.3%, 78.7%, and 96.1% for Triple D scores of 0, 1, 2, and 3, respectively, they concluded that the Triple D correlates with SWL success. 7 In Gokce's study investigating the validation of Triple D scores in elderly patients with renal and ureteral stones, a score of 3 was associated with 95.5% and 95% success, respectively. Conversely, the success rates of patients with a Triple D score of 0 were 20% and 25% in the renal and ureteral stone groups. 20 In our study, Triple D scores were significantly lower in patients in whom SWL had failed (1.2 vs 1.9, p < 0.001). Multivariate analyses revealed that a Triple D score was an independent factor to predict SWL success.
The Triple D score includes SV, SSD, and stone density, three variables that are accepted as predictive factors for SWL outcomes; however, the accuracy of nomograms for SWL may be improved by the addition of other prognostic factors such as the presence of renal abnormalities, stone number, presence of obstruction, impaction of ureteral stones, and especially stone location. For example, in Kanao's study, the highest stone-free rate was achieved in the treatment of mid-ureteral stones, and the lowest stone-free rate was observed after the treatment of lower pole stones. 19 In like manner, Abdel-Khalek and colleagues reported that the presence of a lower pole stone associated with SWL failure. 21 In the present study, stone location was an independent risk factor for SWL success in multivariate logistic regression analysis. That stone location (especially lower caliceal anatomy) is not included as an important factor affecting SWL outcome is a limitation of the Triple D.
Although our present study is the first to externally validate the Triple D scoring system in a general population, it has some limitations. First of all, this is a retrospective study. Second, the study group was heterogeneous in nature, focusing on renal and ureteral stones. In addition, the number of patients with ureteral stone was relatively small.
Conclusion
This study externally validates that the Triple D scoring system is associated with SWL success in the treatment of renal and ureteral stones. Further studies are warranted to assess clinical usefulness and the accuracy of this nomogram in different patient groups; yet, for patients with upper urinary tract stones, a Triple D score may be an effective tool in selecting the most appropriate candidates for SWL.
Footnotes
Author Disclosure Statement
No competing financial interests exist.