
Abstract
Objective:
The aim of this study was to evaluate the safety, feasibility, and effectiveness of bipolar transurethral plasmakinetic enucleation of the prostate (PKEP).
Patients and methods:
Between January 2010 and October 2013, 245 patients with lower urinary tract symptoms due to benign prostatic hyperplasia underwent transurethral enucleation of prostate using bipolar plasma vaporization energy. Patients were evaluated preoperatively by full detailed history, routine preoperative investigation digital rectal examination, serum prostate-specific antigen, abdominal and transrectal ultrasonography, and maximum flow rates (Qmax).
Results:
Patients' ages ranged from 50 to 81 (65.5 ± 6) years with transrectal ultrasound-measured prostate volume of 97.1 ± 36.7 mL resulting in an operating time of 76.9 ± 27.9 minutes, and postoperative irrigation and catheterization times were 3.5 ± 3.2 and 12.7 ± 6.1 hours, respectively. No significant complication occurred intra- or postoperatively. Qmax increased from 7.1 ± 3.2 mL/second preoperative to 18.4 ± 4.2 mL/second (p < 0.001). The International Prostate Symptom Score decreased from 25 ± 6 to 7.9 ± 2.4 (p < 0.01).
Conclusion:
This study confirmed that PKEP is a safe, easy to learn, and durable technique suitable for any prostate sizes.
Introduction
B
Conventional monopolar transurethral resection of prostate (M-TURP) was considered as the gold standard of surgical management for BPH causing lower urinary tract symptoms (LUTS). 3
The complications rate associated with M-TURP is ranged between 7% and 43%, which are mainly bleeding, transurethral-resection syndrome, urinary incontinence, retrograde ejaculation, infection, and erectile dysfunction. Moreover, the mortality rate associated with M-TURP is 0.2%. 4
Technical modification of transurethral resection of prostate (TURP) with incorporation of bipolar technology (bipolar transurethral resection of prostate [B-TURP]) has two advantages: first, patients can better tolerate sodium chloride solution and thus eliminate the risk of transurethral resection (TUR) syndrome. Second, the high-frequency current used minimizes tissue denaturation. The resectoscope and electrode act as the neutral electrode that completes the circuit without need to the patient's plate. 5,6
The depth of tissue penetration in plasma vaporization is about 0.2 mm, which is smaller than with M-TURP. This leads to controlled vaporization of superficial tissue layers virtually without heat, thus even named “cold vaporization.” 7
Prostatic adenoma can be enucleated anatomically regardless its size with few morbidities. This can be done by using the tip and loop of the resectoscope for dissection of adenoma instead of surgeon's finger in open prostatectomy (OP). 8,9
Despite its innovative nature, the plasma vaporization electrode does not involve great expense for hospitals. The bipolar transurethral resection in saline cutting loops can simply be replaced by the new vaporization electrode.
Not only the cost for the upgrade is much lower than with standard laser vaporization procedures but the cost for the single-use electrode is also lower.
In addition to the low equipment costs and short hospital stay, the short learning curve of the procedure adds to its excellent benefit effectiveness. In contrast to other modern minimally invasive procedures, the technique is similar to the commonly practiced standard TURP method. Extensively long learning courses and training periods are thereby reduced. 4,7
Patients and Methods
Two hundred forty-five patients with LUTS due to BPH were included in this study.
The patients underwent the following preoperative evaluation: detailed medical history and digital rectal examination. In addition, urine analysis with culture and sensitivity (when indicated), renal function tests, hemoglobin concentration, coagulation profile, serum electrolytes, blood sugar and liver function tests, and serum prostate-specific antigen were assessed. Furthermore, abdominal and transrectal ultrasonography (US) was performed to assess upper tract and to measure residual urine and prostate size and maximum flow rates (Qmax; voided urine >150 mL).
Inclusion criteria were as follows: the study included patients with Qmax of ≤10 mL/second or obstructive pressure-flow study due to BPH, severe LUTS/BPH requiring surgical treatment, and International Prostate Symptom Score (IPSS) >7 due to BPH.
The exclusion criteria were as follows: patients with prostate and/or bladder cancer, bladder diverticulae, urethral stricture, active urinary tract infection (UTI), unless treated and culture became sterile, and men with neurogenic voiding dysfunction. In addition, patients who did not complete at least 3 years of follow-up.
All patients underwent transurethral enucleation of prostate using bipolar plasmakinetic energy.
The technique required a bipolar generator of high-frequency power for sufficient plasma activation; the power output is set at 180 and 100 W for cutting and coagulation modes, respectively.
The SurgMaster™ UES40 (Olympus, Tokyo, Japan) generator and a 26F continuous flow resectoscope with a separate irrigation channel were used.
Physiologic saline at 37°C was used as an irrigant to ensure excellent visibility and for elimination of vaporization bubbles.
Bipolar plasma enucleation of the prostate was performed under direct visualization using a continuous flow resectoscope, vaporization mushroom electrode, and cutting loop (Olympus Winter & Ibe GmbH, Hamburg, Germany).
As a first stage, bladder neck and/or middle lobe were dealt with by making two lateral incisions at 5 and 7 o'clock positions starting from just below the ureteral orifices to verumontanum using the mushroom electrode (Fig. 1). Then, the two incisions were connected and deepened to the level of capsular fibers. The retrograde mechanical pushing technique, utilizing the peak and the loop of resectoscope, was used to separate the median lobe off the prostatic bed (Fig. 2). The median lobe was left suspended by a small stalk for the purpose of easy, rapid, and safe resection by the cutting lobe (Fig. 3).

5 o'clock incision.

Enucleation of median lobe.

Resection of enucleated lobe.
In the second stage, a transverse mark incision was made just proximal to the external sphincter and then a longitudinal incision was made, starting at the anterior bladder neck (12 o'clock position) and ending at the transverse mark incision (apex of the prostate). The incision was deepened to the level of capsular fibers to separate the two lateral lobes from each other. This enabled us to manage each lobe individually in a retrograde manner starting at the apex and sweeping it back into the bladder by the resectoscope tip until the level of bladder neck was reached. While it was still attached by a small pedicle to the bladder, the lobe was safely and rapidly cut into pieces using the cutting electrode. The tissue was removed by bladder evacuator and the resulting tissue chips were sent for histopathologic examination. At the end of the procedure, urethrocystoscopy was performed and any residual adenomatous tissue in the prostatic bed was ablated by plasma vaporization (Fig. 4).
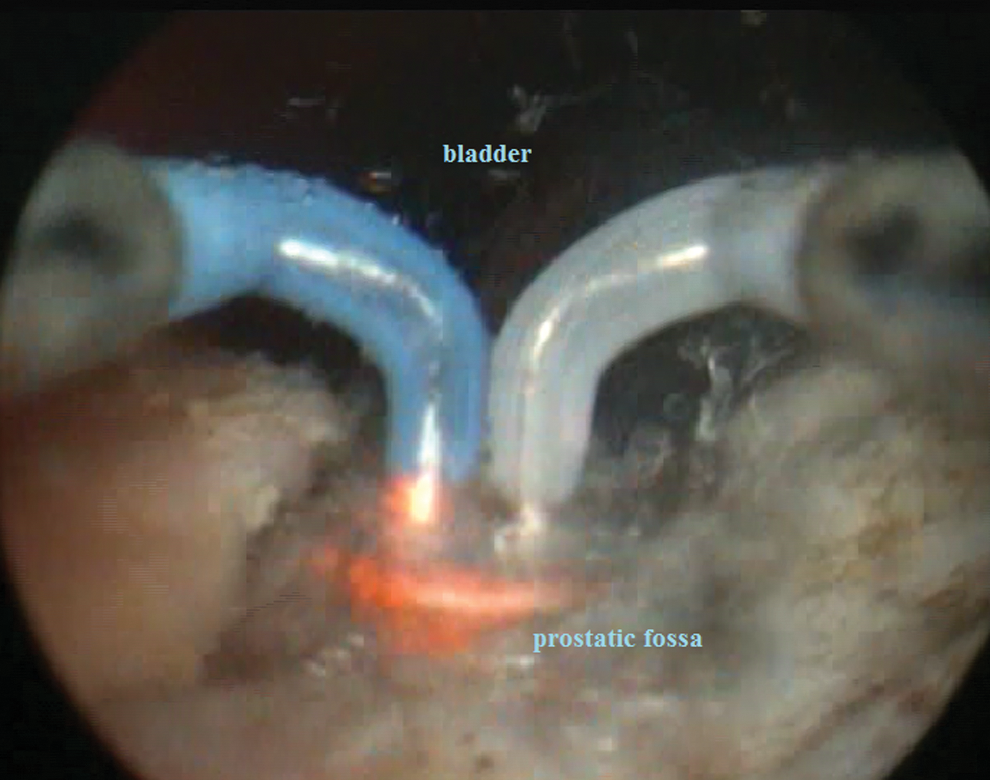
Finishing off the procedure.
Postoperative evaluation
All patients received continuous bladder irrigation postoperatively, and the irrigation volume and bladder washouts were recorded.
Duration of catheterization, any complications associated with catheter removal, and the length of hospital stay were recorded.
Adverse events, such as pyrexia, hypotension, blood transfusion, or clot retention episodes, were observed. Special attention was made to any signs of TUR syndrome.
In addition, blood hemoglobin, sodium, and potassium were measured postoperatively.
Follow-up
The patients were followed up postoperatively at 1, 6, 12, 24, and 36 months. The follow-up included IPSS, quality-of-life assessment, uroflowmetry, and pelvic US (for estimation of postvoiding residual urine [PVRU] and prostate size).
Results
The study was conducted on 245 patients with BPH who underwent plasmakinetic enucleation of the prostate (PKEP), their age ranged from 50 to 81 years (mean 65.5 ± 6 years).
The mean IPSS preoperatively was 24.4 ± 6.1 (M ± SD) and ranges from 12 to 35.
The mean baseline prostate volume, evaluated by transrectal US, was 97.1 ± 36.7 mL (range 40–230), resulting in operating time of 25 to 150 minutes with an average of 76.9 ± 27.9 minutes (Table 1). During the procedure, 6.9 ± 8.9 L (range 5–72 L) of irrigation saline was used.
IPSS = International Prostate Symptom Score; PVRU = postvoiding residual urine; Qmax = maximum flow rate.
Only one electrode was utilized for every patient without technical failures.
All treated patients did not have any significant perioperative morbidity associated with the plasma enucleation. Only two patients required blood transfusions (1 U for each) (Table 4). The mean preoperative hemoglobin (Hb) value was 12 g/dL (range 10.5–14.3 g/dL) and the mean postoperative Hb value was 11.7 g/dL (range 9.8–13.8 g/dL), with no significant statistical difference.
There was no significant fluid absorption during the procedure, and thus, there were no disturbances in serum electrolyte form of TUR syndrome. The mean preoperative serum sodium (Na+) value was 140.4 ± 5.2 mEq/L (range 133–145 mEq/L) and the mean postoperative Na+ value was 137.5 ± 4.9 mEq/L (range 130–145 mEq/L).
The mean overall catheterization time was 12.7 ± 6.1 hours (range 8–24 hours). The mean irrigation time was 3.5 ± 3.2 hours (range 0.5–6 hours) (Table 2).
Six patients presented with obstructive LUTS 1 week postoperative, who required catheterization for 1 week and then another trial of catheter removal that was effective; the patients were able to void normally (Table 4).
The mean hospital stay time was 21.3 ± 6.5 hours (range 16–28 hours), most patients were discharged after catheter removal and effective voiding.
In postoperative follow-up, uroflowmetry showed dramatic improvement in the voiding pattern as Qmax improved from 6.7 as a mean (range 0–12) preoperatively to a mean of 18.5 (range 11–35). In addition, there was marked reduction of IPSS from 21.5 as a mean (12–35) preoperatively to a mean value 8.3 (3–12) postoperatively (Table 3).
Because of vaporization of some prostatic tissues during the procedure, so the estimation of removed prostatic tissue can be roughly assessed by the difference in the mean prostatic volume measured preoperative (mean ∼97 g) (range 40–230 g) and the postoperative (mean ∼34.5 g) (range 15–90).
In this study, early and late adverse events are reported in Table 4. Six patients (2.4%) had urinary tract infection. Their urine cultures were positive, and their irritative symptoms improved after proper antibiotics, according to culture and sensitivity. Only five patients had acute urinary retention after initial attempts of catheter removal and required recatheterization. Indeed, these patients were discharged with an indwelling catheter, which was then removed on second attempt 1 week later and discharged after effective voiding trial. In three patients, clot retention occurred, which required recatheterization, manual bladder irrigation for clot evacuation, and then continuous bladder irrigation for a while.
Postoperative secondary hematuria was encountered in three patients only. Eight patients suffered from self-limited transient incontinence and were urodynamically evaluated, which proved no intrinsic sphincter deficiency. All of the eight patients improved within 3 months. Urethral stricture was diagnosed in two patients who required no more than dilation on an outpatient basis without visual internal urethrotomy. Bladder neck resection was performed for only one case because of persistence of obstructive symptoms due to bladder outlet stenosis.
Discussion
In most developing countries, OP is commonly practiced as the gold standard for management of large prostate, which is an effective and durable option ensuring anatomical removal of nearly all obstructing prostatic tissue. 10
Minimally invasive options are greatly considered at present, especially with increased patient awareness about these options guided by the Internet and multiple mass media. 11,12
With the great development of appliances and introduction of new technologies, precise enucleation of prostate can be done with ease and excellent outcome. 13 Many different types of laser energies can be used for endoscopic management of prostate by using their three modes; resection, vaporization, and/or enucleation. 13 Enucleation by laser using combined resection and hemostasis allows removal of the adenoma with any size reaching the surgical capsule. 14 However, wide use of lasers is limited by many obstacles especially in developing countries such as costs, steep curve of learning (about 50 cases), limited endoscopic appliances, and lack of expertise. Unlike holmium laser enucleation of the prostate (HoLEP), PKEP uses the same equipment as bipolar TURP, with no extra equipment required. 15
It was found that an endourologist experienced with TURP can become skilled with PKEP within 10 cases only. 16
In bipolar surgery, the risks of burns and cardiac pacemaker problems are abolished. Besides, more efficient tissue removal with simultaneous excellent hemostasis is the main advantage of this technique in comparison with the monopolar procedure. Effective and precise coagulation decreases the hemostasis time and provides clear field of vision during the procedure. 17 Thus, it is indicated in patients at high risk and those who are on anticoagulant agents. 18
On contrary to the high thermal effect of monopolar energy (around 400°C), bipolar energy yields temperature not exceeds 40°C to 70°C because of conversion of saline irrigate into highly ionized plasma field. 19
In our study, the mean operative time was ∼77 minutes while the mean removed prostatic tissue was 75.8 g (∼1 minute for each gram of enucleated volume). Indeed, many authors reported that the operative time is approximately around 1 minute for each enucleated 1 g of prostate in terms of time for weight, 16,20,21 compared with 72.09 to 197 minutes for 56.2 to 106 g in HoLEP and 57.5 to 173 minutes for 62.6 to 151 g in OP procedures. 22 –24
Previous study by Chen and colleagues compared PKEP with OP. They reported that no patient (0/80) in the PKEP arm required postoperative blood transfusion, while four patients (4/80) required transfusion in the OP group. 16 Another study demonstrated that there was a lower transfusion rate of 1.4% in favor of PKEP group vs 8.6% in OP group. 9 Similarly, our results demonstrated that only 2 patients out of 245 patients (0.8%) required transfusion of only 1 U of blood. One of those patients had a prostate of 230 g and his main presentation was hematuria with clot retention that required preoperative transfusion. The second patient was on anticoagulant medication preoperatively.
With regard to the occurrence of TUR syndrome, none of our patients experienced TUR syndrome. Using saline as an irrigate eliminated this risk. This finding is consistent with several previous reports concerning plasmakinetic energy, 6,8,9,20 and this is considered one of the major advantages of this technique.
Short catheterization time and hospital stay had a positive impact on our patients as they greatly appreciated it. In fact, most of patients involved in this study had their catheter removed and were discharged next day after surgery. This is similar to a study by Neill and colleagues who reported catheter time and hospital stay of about 1 day. 25 Other studies reported longer catheter time and hospital stay as they included in their works large prostate only, which is contrary to our study that included a wide range of prostate sizes. 8,9,16,20
Regarding the early postoperative complications, our results revealed that urinary retention requiring catheterization was noticed in 5 (∼2%) patients. Indeed, previous trials have reported that rate of urinary retention requiring catheterization to be 1.4% to 4.2%. 9,20 In another study, none of patients developed postoperative urinary retention. 16 The mean rate of recatheterization after HoLEP varied from 1.2% to 3%. 26,27 In addition, we observed postoperative irritative LUTS in 3.6% of patients and urinary tract infection in 2.4% of them. Chen and colleagues reported irritative symptoms and UTI in 11.4% and 2.9%, respectively. 16
Concerning the long term adverse events, we reported 3 (1.2%) cases suffered from post procedural urethral stricture and 2 (0.8%) patients suffered from bladder neck contracture and required bladder neck resection as an auxiliary procedure for relieve of their symptoms.
In our study, no patient suffered from permanent urinary incontinence. Two studies used the same technique have reported urethral stricture rates between 3.1% and 3.75% and bladder neck sclerosis rates of 1.6% and 1.25%, respectively. 9,16 In our study, no patient had residual adenoma necessitating reoperation, which is the same as that of Chen et al. 16 On the contrary, in a study of 96 patients treated by HoLEP, 3 patients had reoperation because of having residual adenoma. 28
Prostatic capsule perforation and bladder and/or ureteral orifice injury are well-known complications of morcellation due to entrapment of bladder mucosa during the procedure, 11,15,28,29 a complication that did not occur with us. In a recently published study using PKEP, 1 out of 180 patients had a capsular perforation. 30
During the 3-year period of postoperative follow-up, function outcomes such as IPSS, Qmax, and PVRU were excellently improved compared to the baseline of these parameters. In addition, there were no statistically significant changes in comparison with different follow-up periods. When comparing these parameters to different procedural types, such as HoLEP, transurethral vaporization of the prostate, and OP, the results are summarized in Table 5.
After 2 years.
HoLEP = holmium laser enucleation of the prostate; PKEP = plasmakinetic enucleation of the prostate; TUVP = transurethral vaporization of the prostate.
As shown in Table 5, there is no significant difference in functional results of different techniques after a mean 6 months of postoperative follow-up.
Conclusion
This study confirmed that PKEP is a safe, easy to learn, and durable technique with good functional results and low morbidity.
The technique is suitable for any prostate size and even a patient on anticoagulant drugs can be treated safely.
Footnotes
Acknowledgment
The authors thank Dr. S.A. Salama, Professor of Pharmacology and Toxicology, Al Azhar University, for carefully revising the article and for his generous help.
Author Disclosure Statement
No competing financial interests exist.