
Abstract
Introduction:
Ureteroscopy is increasingly used to treat upper tract urinary stone disease. A negative ureteroscopy is a ureteroscopy performed with the intent of removing a kidney or ureteral stone, but in which ultimately no stone is removed. Negative ureteroscopy may occur when the stone is found to have already passed, or the presumed stone is found to be outside of the collecting system. We sought to determine the rate of negative ureteroscopy in a large population-based sample as well as factors associated with its use.
Patients and Methods:
We examined nonpublic data from the Office of Statewide Health Planning and Development (OSHPD) Database for all patients in California undergoing outpatient surgery from 2010 to 2012. We identified all patients with an International Classification of Diseases, Ninth Revision (ICD-9) diagnosis code for upper tract urinary stone disease, who underwent a ureteroscopic procedure. After excluding patients undergoing second look procedures or who had diagnosis codes for separate urologic pathology, the negative ureteroscopy rate was defined as the proportion of those ureteroscopy cases coded as a diagnostic ureteroscopy. We fit logistic regression models to evaluate patient factors associated with negative ureteroscopy.
Results:
During the years 2010 to 2012, 20,236 eligible patients underwent ureteroscopic procedures for upper tract stone disease. Of these, 1287 patients underwent diagnostic ureteroscopy and 19,039 underwent ureteroscopy with stone removal accounting for a negative ureteroscopy rate of 6.3%. The odds of receipt of a negative ureteroscopy rate were higher in females compared to males (odds ratio [OR] 1.41, 95% confidence interval [CI] 1.25, 1.58) and lower in self-pay patients compared with insured patients (OR = 0.55, 95% CI 0.33, 0.91).
Conclusions:
Negative ureteroscopy is common, occurring in nearly 1 in 16 procedures to treat urinary stone disease.
Introduction
U
Negative ureteroscopy may be akin to negative appendectomy (where an operation for appendicitis is undertaken only to find a normal appendix), a concept well established in the general surgery literature. The current negative appendectomy rate is thought to be ∼5%, down from as high as 10% to 20%. This has been attributed to the increased use of more sensitive imaging. 6 –8 However, the rate of negative appendectomy is unlikely to become zero as imaging is imperfect and physicians must often balance providing timely care, minimizing pain, and limiting the risks/costs of imaging studies. A similar situation can also be found in upper tract urinary stone disease.
Negative ureteroscopy has previously been reported to be more common in patients with small stones 5 and those who are pregnant. 9 However, negative ureteroscopy has not been evaluated using large population-based data. We sought to determine the rate at which negative ureteroscopy occurs in California, a diverse and populous state. We also sought to determine if certain patient characteristics are associated with receipt of a negative ureteroscopy.
Materials (Patients) and Methods
After receiving permission from the California Office of Statewide Health Planning and Development (OSHPD) and the California Protection of Human Subject Committee, we analyzed all outpatient upper tract stone surgeries performed from 2010 to 2012. Specifically, we queried nonpublic data sets of both the Ambulatory Surgery Database and the Patient Discharge Database. 10 The Ambulatory Surgery Database includes all nonfederal outpatient procedures performed at ambulatory surgery centers in the state, and the Patient Discharge Database includes data on all inpatient hospitalizations. In both data sets, up to 25 diagnostic codes (The International Classification of Diseases, Ninth Revision [ICD-9]) and 20 procedural codes (Current Procedural Terminology [CPT] or [ICD-9]) for each unique visit are coded. In addition, in the nonpublic data sets, each individual has a unique record linkage number that allows them to be followed longitudinally.
Analytic cohort
We identified all patients who underwent an outpatient ureteroscopy procedure (CPT code 52351, 52352, or 52353) and had an ICD-9 diagnosis code for upper tract urinary stone disease (Fig. 1). If a patient had more than one procedure code on the same day, we assigned them one CPT code based on the hierarchy 52353 > 53352 > 52351. We defined a positive ureteroscopy procedure as those patients with an ICD-9 diagnosis code for upper tract nephrolithiasis, who underwent ureteroscopy with either basketing of stone or lithotripsy of stone (CPT 52352 or 52353). We defined our negative ureteroscopy group as patients who underwent a diagnostic ureteroscopy (CPT 52351). We determined the rate of negative ureteroscopy using the number of individuals with a negative ureteroscopy over the total number of ureteroscopic procedures.
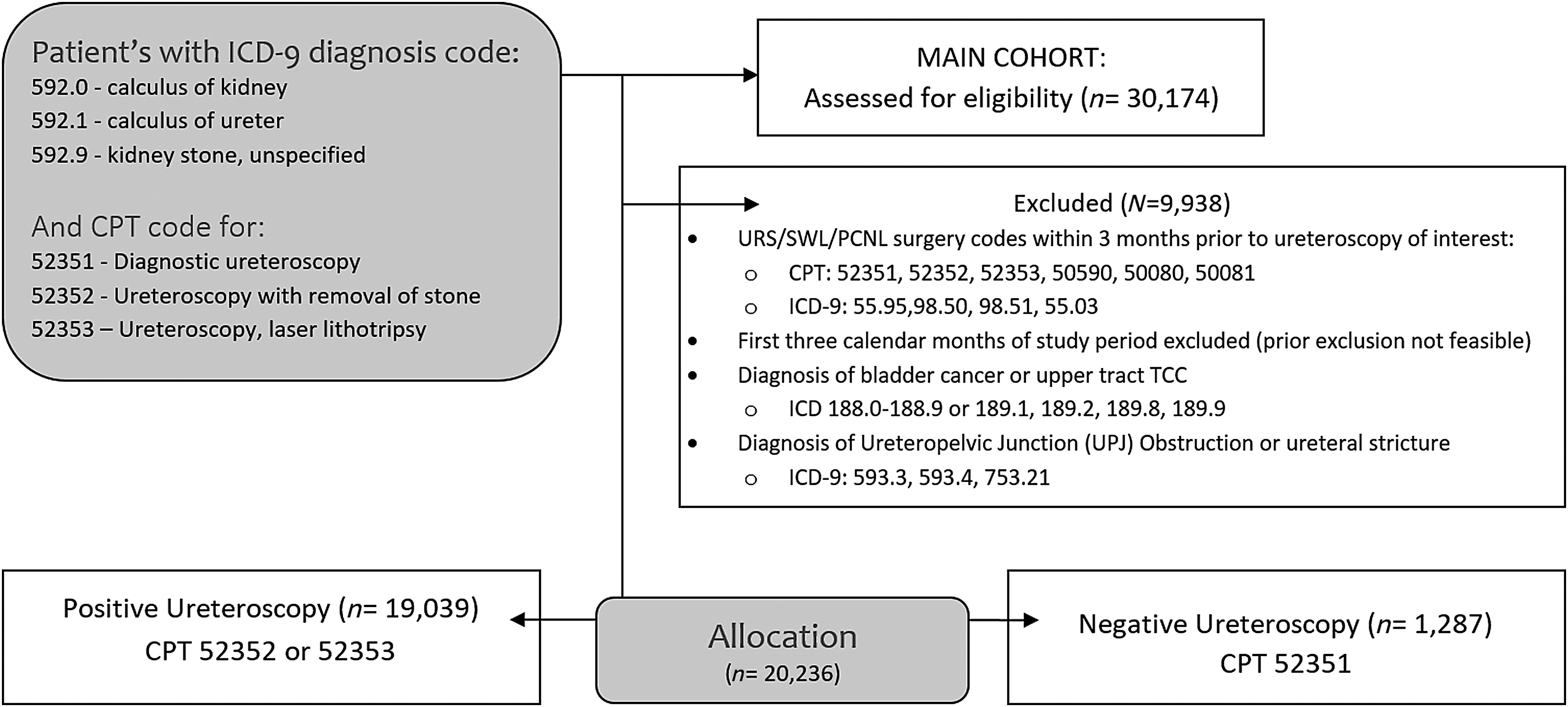
Consort diagram of inclusion and exclusion criteria. CPT, Current Procedural Terminology; ICD-9, International Classification of Diseases, Ninth Revision; PCNL, percutaneous nephrolithotomy; SWL = shockwave lithotripsy; TCC = transitional-cell carcinoma; URS = ureteroscopy.
To prevent analysis of “second look” procedures, we excluded any ureteroscopies that had a separate endoscopic, open, or extracorporeal shockwave lithotripsy stone surgery performed 90 days prior (Table 1). Similarly, ureteroscopy procedures that occurred in the first 90 calendar days of the study period were also excluded as this prior ureteroscopy period could not be confirmed. In addition, we excluded any ureteroscopic procedure associated with bladder cancer, upper tract urothelial cancer, ureteral stricture, or ureteropelvic junction obstruction. Some diagnostic ureteroscopies may be explained by an initial ureteroscopy that is aborted due to a tight ureter or ureteral perforation. We therefore also performed an additional sensitivity analysis, in which we excluded patients completely if they had any stone procedures done within 30 days of each other.
CPT = Current Procedural Terminology; GU = genitourinary; PCNL = percutaneous nephrolithotomy; ICD-9, International Classification of Diseases, Ninth Revision; SWL = extracorporeal shockwave lithotripsy; URS = ureteroscopy; UPJ = ureteropelvic junction.
Statistical analysis
We identified patient characteristics, including gender, age, race/ethnicity, and insurance type. We fit univariable and multivariable logistic regression models to identify factors associated with the receipt of a negative ureteroscopy. We used STATA programming software (Version 14, State College, TX). All tests were two sided, and a p-value of 0.05 was considered significant.
Results
During the years from 2010 to 2012, 30,174 patients underwent a ureteroscopic procedure in California. Our analytic cohort included 20,236 primary ureteroscopies performed for urinary stone disease. The patient demographics and characteristics are listed in Table 2. The majority of our patients were between the ages of 40 to 79 (78.4%). Only 0.8% of our patients were <19 years of age. The cohort included more men than women (59.6% vs 40.8%, respectively). Although diverse, the majority of patients undergoing ureteroscopy were white (66.5%).
BC/BS = Blue Cross/Blue Shield; EPO = exclusive provider organization; HMO = Health Maintenance Organization; POS = Point of Service, PPO = preferred provider organization.
The overall rate of negative ureteroscopy was 6.3% (1287 negative ureteroscopies and 19,039 positive ureteroscopies). Negative ureteroscopy was least common in the oldest age group (age 80 or more = 5.2%) and most common in the youngest age group (age 19 or less = 9.8%; Table 3). Females underwent negative ureteroscopy at a greater rate than males (7.6% vs 5.4%), and African Americans tended to have a lower rate of negative ureteroscopy (5.2%) than other racial/ethnic groups. The rates of negative ureteroscopy varied based on insurance type; rates were lowest (3.3%) among self-pay patients and greatest (9.6%) among patients with Medi-Cal. Patients with BlueCross/BlueShield or Medicare Part A/B also had higher rates of negative ureteroscopy (7.9%, 7.9%, respectively). The rate of negative ureteroscopy did not significantly change appreciably based on the year (6.6% in 2010, 6.4% in 2011, and 6.1% in 2012). In our sensitivity analysis model where we excluded patients who had any stone procedures performed within 30 days of each other, the negative ureteroscopy rate was 5.5%, not dissimilar from the rate we originally determined.
ORs in bold indicate statistical significance threshold of p < 0.05.
CI = confidence interval; OR = odds ratio.
In our multivariate model, patient age, year of surgery, and race/ethnicity were not associated with the odds of receipt of a negative ureteroscopy (Table 3). Female sex was independently associated with increased odds of negative ureteroscopy (odds ratio [OR] 1.41, 95% confidence interval [CI] 1.25, 1.58). Several insurance types were also significantly associated with increased odds of negative ureteroscopy: BlueCross/BlueShield or other commercial insurance (OR 1.42, 95% CI 1.19, 1.70), Medicare Part A/B (OR 1.61, 95% CI 1.32, 1.96), and Medi-Cal (OR 1.58, 95% CI 1.26, 1.98). Self-pay was independently associated with decreased odds of negative ureteroscopy (OR 0.55, 95% CI 0.33, 0.91), while Health Maintenance Organization (HMO) Medicare preferred provider organization (PPO), and “other” insurance were not associated with receipt of negative ureteroscopy.
Discussion
We found that 6.3% of ureteroscopy procedures for urinary stone disease in California were negative ureteroscopies. To our knowledge, the rate of negative ureteroscopy in the general population has not been previously described. In a study including patients treated by a single fellowship-trained urologist at a single hospital, Kreshover and colleagues reported negative ureteroscopies in 25 of 256 of “renal units” (9.8%). 5 Our study encompasses a much larger population and may better reflect the rate of negative ureteroscopy occurring in the community. In the only other prior study, 14% of ureteroscopies performed in pregnant patients were classified as a negative ureteroscopy. 9 It is likely that this increased rate of negative ureteroscopy is attributable to the desire to avoid diagnostic procedures requiring radiation in this population.
The concept of negative ureteroscopy parallels that of negative appendectomy, where there is growing pressure to reduce the rate of surgery for a normal appendix. 6 The general surgery community has developed algorithms to optimize care, while limiting cost and radiation exposure. 11,12 In the Netherlands, the implementation of these guidelines reduced the negative appendectomy rate from 22.9% to 6.2% over a 3-year period, and the average cost per patient was also reduced. 11 To date, the appropriate or acceptable rate of negative ureteroscopy remains unknown. It is likely that there is an acceptable rate of negative procedures, which minimizes costs by reducing the number of diagnostic imaging studies and radiation exposure, yet still provides timely and appropriate care to the patient.
We identified several disparities in the receipt of negative ureteroscopy. It is not clear why female patients would have increased rates of negative ureteroscopy. One possible explanation is the increased prevalence of pelvic phleboliths on imaging that could be mistaken for urinary stone. 13 –15 Women also have a higher prevalence of medullary sponge kidney, where differentiation between true urinary stone disease and parenchymal calcifications may be more difficult. 16 There are several possible explanations why a woman may be less likely to observe a passing stone making them more prone to undergo a ureteroscopy where no stone is found. It is possible that women, who typically sit during urination may have more difficulty visualizing a passed stone. Alternatively, passing of the stone through the shorter female urethra with a lower voiding pressure may result in less overall dysuria. 17
In our cohort, there were significant differences in negative ureteroscopy based on a patient's type of insurance. Most notably, those who were responsible for the cost of their procedure (“self-pay”) had a negative ureteroscopy rate of only 3.3%. This may reflect limited access to ureteroscopy, or a preference to pursue conservative management of urinary stone disease in this group. Conversely, it may also indicate that in the uninsured, ureteroscopic procedures are only performed in cases of obvious stone obstruction or when longer trials of stone passage fail. 18 –20 Similarly, uninsured patients with appendicitis are more likely to present with complicated appendicitis and require open surgery. 21 Conversely, those with certain types of insurance such as BlueCross/BlueShield, Medicare Part A/B, and Medi-Cal were associated with increased odds of receipt of a negative ureteroscopy. It is possible that this may simply reflect better access to services, even in low-income publically insured adults, 22 however, our reference group also had similar access to the services, and the reason for this finding is unclear. The financial burden of urinary stone disease in the United States continues to increase, 23 and this report underscores the need for urologists to balance the risks and costs of surgery, imaging, and observation.
The limitations of this study include a lack of clinical information on stone complexity (e.g., stone size, location) and prior care (e.g., diagnostic imaging tests). Our study of administrative claims data is also subject to procedure misclassification. However, urologists are incentivized to code for a ureteroscopy with intervention (basket or laser), as this generates higher reimbursements. Thus, our negative ureteroscopy rate is not likely to be overestimated. We also did not have access to CPT modifiers, hindering our ability to identify bilateral procedures when the same code was used on more than one side. Consequently, we could not fully account for renal units as reported by Kreshover and colleagues. For example, if a patient has an effective ureteroscopy with laser lithotripsy on the right and a diagnostic ureteroscopy on the left, our analytic methods considered them to have undergone a “positive” ureteroscopy. As a result, our analysis may be biased to underestimate the negative ureteroscopy rate in these cases.
Despite these limitations, this study has several notable strengths. First, our study population of >20,000 plus patients is significantly larger than previously reported and population based. We also capture a diverse cohort of patients treated during a contemporary 3-year period. As a result, our findings are likely to be generalizable to patients with kidney and ureteral stones receiving care across the United States.
Conclusions
We found that 6.3% of ureteroscopies for urinary stone disease were classified as negative ureteroscopy. Female sex was associated with an increased risk of negative ureteroscopy. The insurance status of the patient may also influence the rate of negative ureteroscopy. Future studies aimed at minimizing costs, optimizing care, and decreasing radiation exposure could help reduce negative ureteroscopy rates.
Footnotes
Author Disclosure Statement
No competing financial interests exist.