
Abstract
Purpose:
To validate plasma fibrinogen and serum cholesterol levels as prognostic factors for patients with renal cell carcinoma (RCC) and to explore the prognostic value of their combination.
Patients and Methods:
Medical data for 1360 RCC patients after nephrectomy were collected. X-tile software was used to determine the cutoff values. The association between clinicopathological factors and fibrinogen and cholesterol levels was determined, and factors predicting survival were examined by multivariate analysis.
Results:
The median follow-up was 67 months (interquartile range 36–74 months). On univariate and multivariate analysis, both preoperative plasma fibrinogen and serum cholesterol were independent prognostic factors of cancer-specific survival (CSS) and progression-free survival (PFS). By combining the two factors, we developed a novel index, fibrinogen-cholesterol (FC) score and found it to have better prognostic accuracy than the two factors alone. FC was an independent prognostic factor for both CSS (FC score = 1: hazard ratio [HR] = 3.207, 95% confidence interval [CI] = 1.775–5.793; FC score = 2: HR = 5.516, 95% CI = 2.891–10.527) and PFS (FC score = 1: HR = 2.178, 95% CI = 1.545–3.071; FC score = 2: HR = 3.709, 95% CI = 2.355–5.840).
Conclusion:
Both preoperative plasma fibrinogen and serum cholesterol levels are independent prognostic factors for CSS and PFS in RCC patients after nephrectomy. A novel indicator, FC score, could be considered a novel preoperative prognostic index in RCC.
Introduction
R
Increasing evidence has revealed that tumor behavior and also hematological parameters could be considered prognostic factors in cancer, including RCC. 5 –9 Among those factors, plasma fibrinogen and serum cholesterol levels were recently suggested to be associated with outcomes with RCC. 10 –14
Here, we aimed at validating plasma fibrinogen and serum cholesterol levels as prognostic factors and at exploring prognosis with their combination in a large consecutive series of patients after nephrectomy at a single institution.
Patients and Methods
Patients
The medical records of 1360 RCC patients who underwent nephrectomy in Peking University First Hospital were retrospectively collected. Laboratory data of all patients, including preoperative plasma fibrinogen and serum cholesterol levels, were collected within 7 days before nephrectomy. The pathologic staging was determined according to the seventh TNM classification of the American Joint Committee on Cancer guidelines and Fuhrman grading system. 15,16 Histologic subtyping was determined by at least two experienced pathologists. The study was approved by the Institutional Ethical Review Board of Peking University First Hospital.
Treatment and follow-up
All RCC patients who underwent partial or radical nephrectomy were regularly followed according to institutional practice. Follow-up, including abdomen ultrasonography or abdomen CT, chest X-ray, and laboratory data, was collected every 3 months for the first 2 years, every 6 months until year 5, and then annually.
The clinical outcomes were 5-year cancer-specific survival (CSS) and progression-free survival (PFS). CSS was defined as time from nephrectomy to RCC-associated death. PFS was determined as the period between surgery and the date of RCC-associated death or first tumor progression.
Statistical analysis
Statistical analysis involved the use of SPSS for Windows v20.0 (SPSS, Chicago, IL). The optimal cut-points were analyzed and calculated by X-tile software (Version 3.6.1, Yale University). 17 The Mann–Whitney U-test was used to determine the association of clinicopathological factors and fibrinogen and cholesterol levels. The Kaplan–Meier method was used to estimate survival, and univariate analysis involved the use of log-rank statistics. Variables with significant difference (p < 0.05) on univariate analysis were included in a Cox proportional-hazards model for multivariate survival analyses, estimating hazard ratios (HRs) and their 95% CIs. For all tests, p < 0.05 was considered statistically significant.
Results
Patient and tumor characteristics
The clinicopathological characteristics of 1360 RCC patients are in Table 1. The median age was 55 years (interquartile range [IQR] 46–65), and 408 patients (30%) were women; 1228 patients (90.29%) had clear-cell RCC. The median fibrinogen level for all patients was 320 mg/dL (IQR 274–384.25), and the median serum cholesterol level was 168.98 mg/dL (IQR 147.33–192.96). The median follow-up was 67 months (IQR 36–74); 221 patients (16.3%) showed disease progression, and 139 (10.2%) died due to RCC during follow-up.
ASA = American Society of Anesthesiologists; ccRCC = clear cell renal cell carcinoma; IQR = interquartile range.
Association of clinicopathologic characteristics and preoperative fibrinogen or cholesterol levels
Increased median fibrinogen level was associated with older age (p < 0.001), high Fuhrman grade (p < 0.001), T stage (p < 0.001), high American Society of Anesthesiologists grade (p = 0.001), positive lymph node status (p = 0.001), sarcomatous differentiation (p < 0.001), necrosis (p < 0.001), metastasis (p = 0.001), tumor thrombus (p < 0.001), lymphovascular invasion (p < 0.001), high alkaline phosphatase (p = 0.002), high neutrophil count (p = 0.018), hypoalbuminemia (p = 0.002), and anemia (p < 0.001) (Table 2).
Bold types indicates p < 0.05.
Decreased median cholesterol level was associated with male sex (p < 0.001), increased T stage (p < 0.001) and Fuhrman grade (p < 0.001), positive lymph node status (p = 0.004), sarcomatous differentiation (p < 0.001), necrosis (p < 0.001), metastasis (p < 0.001), tumor thrombus (p < 0.001), lymphovascular invasion (p < 0.001), low serum calcium (p = 0.001), high alkaline phosphatase (p = 0.032), high neutrophil count (p = 0.019), hypoalbuminemia (p < 0.001), and anemia (p < 0.001) (Table 2). In addition, fibrinogen level was increased but cholesterol level was decreased with increasing tumor stage (Fig. 1).

The association of tumor stage and plasma fibrinogen level
Determining cutoff values
We applied X-tile software to determine the cutoff values of plasma fibrinogen, serum cholesterol, neutrophil-to-lymphocyte ratio (NLR), and lymphocyte-to-monocyte ratio (LMR) (Fig. 2). The cutoff values of CSS were calculated as 148 mg/dL for cholesterol, 387 mg/dL for fibrinogen, 2.9 for NLR, and 4.2 for LMR. The cutoff values of PFS were calculated as 148 mg/dL for cholesterol, 429 mg/dL for fibrinogen, 3.8 for NLR, and 4.32 for LMR. According to the cutoff values, all patients were divided into two groups by fibrinogen and cholesterol level.
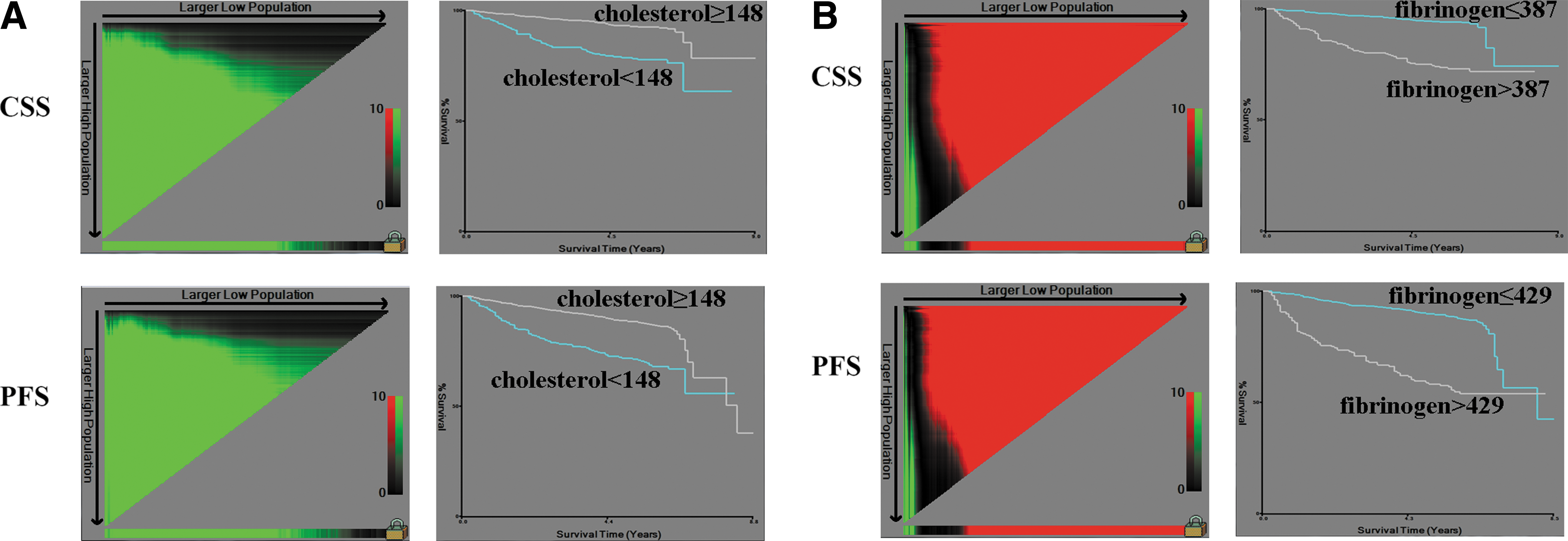
The cutoff values for cholesterol level
Independent prognostic factors of RCC
Five-year CSS and PFS was 78.4% and 64% with an elevated plasma fibrinogen level and 95.4% and 91% with a reduced level. Five-year CSS and PFS was 80.7% and 71.8% with a reduced serum cholesterol level and 93.7% and 88.5% with an increased level. Log-rank test showed significant differences for CSS and PFS by plasma fibrinogen and serum cholesterol level (all p < 0.001) (Fig. 3). On multivariate analysis, both elevated plasma fibrinogen and decreased serum cholesterol levels were independent prognostic factors for CSS and PFS (Table 3).

Kaplan–Meier survival curves for cancer-specific survival and progression-free survival by plasma fibrinogen level
Bold types indicates p < 0.05.
CI = confidence interval; HR = hazard ratio; LMR = lymphocyte-to-monocyte ratio; NLR = neutrophil-to-lymphocyte ratio.
New prognostic index: fibrinogen-cholesterol score
To improve the predictive value of one indicator, we combined plasma fibrinogen and serum cholesterol levels to generate a new prognostic factor, fibrinogen-cholesterol (FC) score. The FC score was defined for CSS and PFS with the following conditions (CSS: plasma fibrinogen level ≥387 mg/dL and serum cholesterol level <148 mg/dL; PFS: plasma fibrinogen level ≥429 mg/dL and serum cholesterol level <148 mg/dL). Therefore, the FC score range was 0, 1, and 2.
On univariate analysis, high FC score (1 and 2) conferred a worse outcome than a score of 0 (Fig. 4). On multivariate analysis, FC score remained an independent risk factor of (FC score = 1: HR = 3.207, 95% confidence interval [CI] = 1.775–5.793; FC score = 2: HR = 5.516, 95% CI = 2.891–10.527) and PFS (FC score = 1: HR = 2.178, 95% CI = 1.545–3.071; FC score = 2: HR = 3.709, 95% CI = 2.355–5.840) (Table 4). The FC score may be considered an effective preoperative prognostic factor in RCC.

Kaplan–Meier survival curves for cancer-specific survival
Bold types indicates p < 0.05.
FC = fibrinogen-cholesterol.
Metastatic status might influence the prognostic ability of prognostic factors. In the subgroup analysis, FC score showed significant differences in localized disease rather than metastatic disease for both CSS and PFS (Fig. 5).
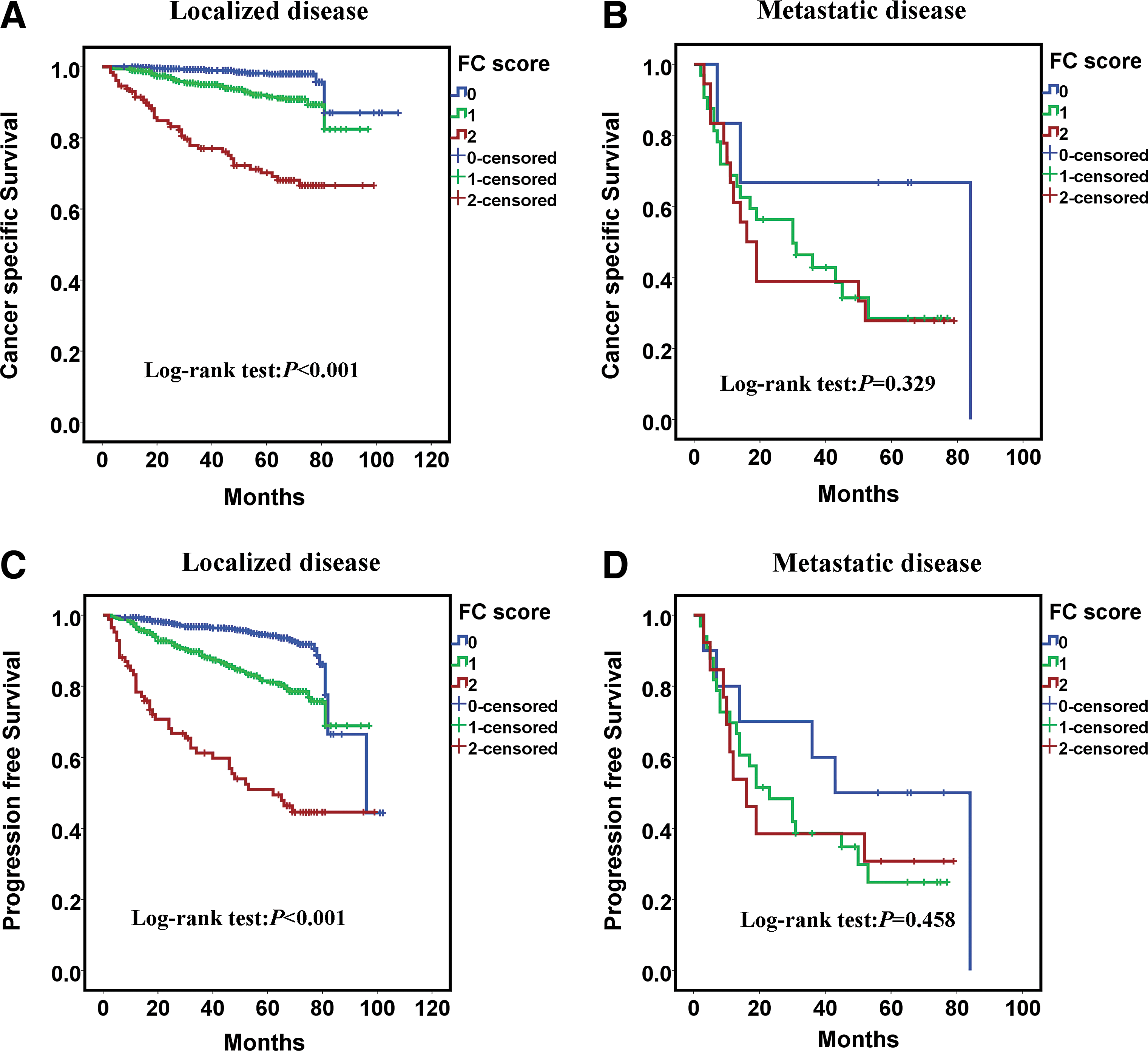
Subgroup analysis by FC score for cancer-specific survival
Discussion
Inflammation and nutrition biomarkers are important factors predicting the prognosis of cancer. Among these biomarkers, preoperative plasma fibrinogen and serum cholesterol levels have been reported to have prognostic value in various types of cancers, including RCC. In the present study, we found preoperative plasma fibrinogen and serum cholesterol levels to be associated with CSS and PFS in RCC and both as independent prognostic factors together with TNM stage and Fuhrman grade on multivariate analysis. Furthermore, we developed a novel index, FC score, combining preoperative plasma fibrinogen and serum cholesterol levels, which may be an effective prognostic factor for CSS and PFS for RCC after nephrectomy.
Du and colleagues 18 first evaluated the association of preoperative plasma fibrinogen level with outcomes for RCC patients. High plasma fibrinogen level was related to Fuhrman grade, tumor size, and T stage. On multivariate analysis, plasma fibrinogen level remained an independent prognostic factor for disease-free survival and overall survival. In several studies, plasma fibrinogen level was higher with metastasis than without metastasis and high plasma fibrinogen level was significantly associated with poor outcomes without metastasis. One study revealed reduced incidence of cancer-specific mortality after surgery in a subgroup analysis of patients with elevated preoperative plasma fibrinogen level that decreased to the normal level after surgery. 12 Lee and colleagues 13 first reported increased cholesterol level that was associated with longer survival with RCC treated with temsirolimus. Then, several studies confirmed the association between clinicopathology factors and low cholesterol level and found that low cholesterol level could be an independent predictor of survival for RCC. 14,19
Consistent with previous studies, we also found high plasma fibrinogen and low serum cholesterol levels to be associated with worse clinicopathologic characteristics such as high TNM and tumor stage, tumor thrombus, lymphovascular invasion, and anemia. Multivariate analysis revealed both high fibrinogen and low cholesterol levels as independent risk factors for both types of survival.
The mechanisms of the worse outcomes caused by high plasma fibrinogen level have been revealed by several previous experimental and clinical studies. Fibrinogen could be considered a bridging molecule between tumor cells and host cells. By enhancing the cell-to-cell adhesion between cancer cells and the extracellular matrix component, fibrinogen promotes cellular adhesion, proliferation, and migration. 20 As well, fibrinogen could help platelets adhere to cancer cells, which could protect cancer cells against the immune system such as natural killer cells. 21 Moreover, fibrinogen plays a central role in the coagulation cascade. The coagulation cascade has been found to be related to vascular endothelial-cell growth factor-dependent angiogenesis, which could promote each other during carcinogenesis. 22
The relationship between cholesterol and tumor prognosis has not been fully elucidated. Cancer cells could acquire cholesterol from serum with elevated activity of low-density lipoprotein (LDL) receptor. 23 Therefore, cholesterol uptake could reduce the serum level, and low serum cholesterol level could reflect abnormal metabolism and proliferation of tumor cells. In addition, LDL and high-density lipoprotein levels were found to be associated with tumor proliferation and invasion. 24
The combination of inflammatory and nutritional indicators can improve the accuracy of the prognosis and cancer outcomes. Ji and colleagues 25 combined neutrophil count with lymphocyte ratio as an index as well as a ratio of aspartate aminotransferase activity to platelet count and found a more precise prediction of outcomes. Sun and colleagues 26 created a Canton score based on prognostic nutritional index, neutrophil/lymphocyte ratio, and platelet/lymphocyte ratio and suggested a novel prognostic index for gastric cancer. In our study, we combined plasma fibrinogen and serum cholesterol levels to develop a novel index, FC score, and showed it to have better predictive significance than either level alone and to be an independent prognostic factor for both CSS and PFS. In addition, FC score was not significant in the metastatic group. This indicated that the predictive significance of FC score might be greater in localized RCC, and metastasis status may be a greater factor than FC score for patients with metastatic disease.
Based on our findings, patients with FC score = 2 may have a greater probability of disease progression and mortality and should be followed closely. Furthermore, it might be possible to improve survival by improving the immunity and nutritional status for those patients. In addition, early targeted therapy or immunotherapy may benefit these patients.
Our study still has some limitations. This is a retrospective and single-institution study. Finding the most effective predictors for RCC still needs more multi-center and prospective studies.
Conclusion
Both preoperative plasma fibrinogen and serum cholesterol levels are independent prognostic factors for CSS and PFS in RCC after nephrectomy. Furthermore, a novel indicator combining both levels, FC score, may be a novel preoperative prognostic index for RCC.
Footnotes
Acknowledgment
This work was supported by the National Natural Science Foundation of China (Grant Nos.: 81372746 and 81672546).
Author Disclosure Statement
No competing financial interests exist.