
Abstract
Purpose:
To propose and evaluate a new endoscopic technique using only a retrograde ureteroscopic approach for the removal of heavily encrusted ureteral stents.
Methods:
Data from 51 consecutive patients with encrusted and retained ureteral stents were prospectively collected. Description of the successive steps of surgery is detailed. The holmium yttrium aluminum garnet (Ho:YAG) laser properties offer the opportunity for fragmentation of stent-attached encrustation and the ability to cut the stent itself. Reducing the length of the stent is critical to creating space in the ureter and to allow free access for ureteroscopes or ureteral access sheath placement. The primary outcome of this study was the feasibility and the safety of this retrograde intrarenal approach. Some factors of encrustation and outcomes are also discussed in comparison with lithotripsy, percutaneous, laparoscopic, open surgery, or a combination of these techniques.
Results:
The removal of the encrusted stent was possible with only this retrograde technique in 98% of patients. The transection of the encrusted stent with the Ho:YAG laser was useful in 71% of the patients. Mean operative time was 110 minutes and mean hospital stay was 2.33 days. Postoperative complications were mainly nonobstructive pyelonephritis (10%). The most significant predictor of this life-threatening complication was the presence of struvite stones with the encrusted stent (p = 0.018). Contrariwise, operative time, body mass index, gender, and encrustation rate were not associated with postoperative pyelonephritis. Both cystine stone disease and pregnancy led to faster stent encrustation.
Conclusions:
Retrograde ureteroscopic surgery is efficient and safe for removing retained stents and associated stone burdens. The Ho:YAG laser is essential to perform the encrustation removal and sectioning of the stent.
Introduction
U
Stent encrustation and stone formation can occur at varying rates depending on patient and environmental factors. 5 Risk factors for encrustation include history of urolithiasis, prolonged stenting, chronic urinary infection, pregnancy, and the type of stent biomaterial. 1,6,7
The removal of encrusted and retained ureteral stents is challenging for the urologist. 8 Multimodal approaches for the removal of encrusted stents have already been set out using various combinations of endoscopic litholapaxy, ureterorenoscopy, extracorporeal shock wave lithotripsy, laparoscopy, and percutaneous nephrolithotomy. 8 –13 Weedin and colleagues suggested that proximal loop encrustation is a determinant factor in the therapeutic approach to such complex cases. 14 Some algorithms have been suggested to help the practitioners in their management. 15,16 In our study, we proposed an integral retrograde ureteroscopic approach to remove encrusted retained ureteral Double-J stents using the holmium yttrium aluminum garnet (Ho:YAG) laser. 17
Over the past two decades, the rise of the Ho:YAG laser has revolutionized the treatment of stone disease and proved able to fragment every type of stone composition. 18 The photothermal fragmentation provided by the laser fiber is extremely precise with minimal traumatic risk for the adjacent urothelial mucosa. We used the ability of Ho:YAG laser to cut the ureteral stent, allowing more working space and admitting complete retrograde access to safely manage the upper encrustations of the stent.
Materials and Methods
Patients
The data of 51 consecutive patients, treated for encrusted and retained ureteral stents from April 2004 to September 2014, were collected prospectively. Most of them (92%) were referred to us from other urologic units for retrograde intrarenal surgery (RIRS). Four indwelling stents were in patients with a solitary kidney (8%) and one in a horseshoe kidney (2%). Patients' mean age was 46 years (range 19 to 80) and the median time the stent had been in place was 6 months (range 1 to 144 months, average 10.4 months). The patients included 30 men and 21 women. The reasons for stent insertion were stone disease (92%), UPJ obstruction (4%), and ureteral catheterization for digestive oncologic surgery (4%). The demographic population characteristics are summarized in Table 1.
A retained encrusted stent was defined as one that could not be removed by the usual cystoscopic methods. Patients who had only encrustation of the bladder curl and were treated cystoscopically were excluded from this study. For all patients in our cohort, we applied the FECal classification proposed by Acosta-Miranda and colleagues 16 to describe the location and the degree of encrustation of each calcified stent (Table 1). Negative urine cultures were documented before each procedure, but nine patients received preoperative antibiotics (19%).
Surgical procedure
One experienced endourologist executed all endoscopic procedures under general anesthesia in the standard lithotomy position (Table 2 and Fig. 1). Antibiotic prophylaxis was given in all patients. First, a 0.035-inch Teflon-coated guidewire (safety wire) was introduced, under fluoroscopic guidance, into the collecting system beside the retained stent. Subsequently, fragmentation of the bladder curl encrustations was achieved cystoscopically with Ho:YAG. If possible, the distal part of the stent was pulled out of the urethral orifice and fixed by a stitch to maintain a gentle traction on the stent and facilitate the achievement of the procedure. This step was sometimes impossible in male patients because of the length of the urethra.
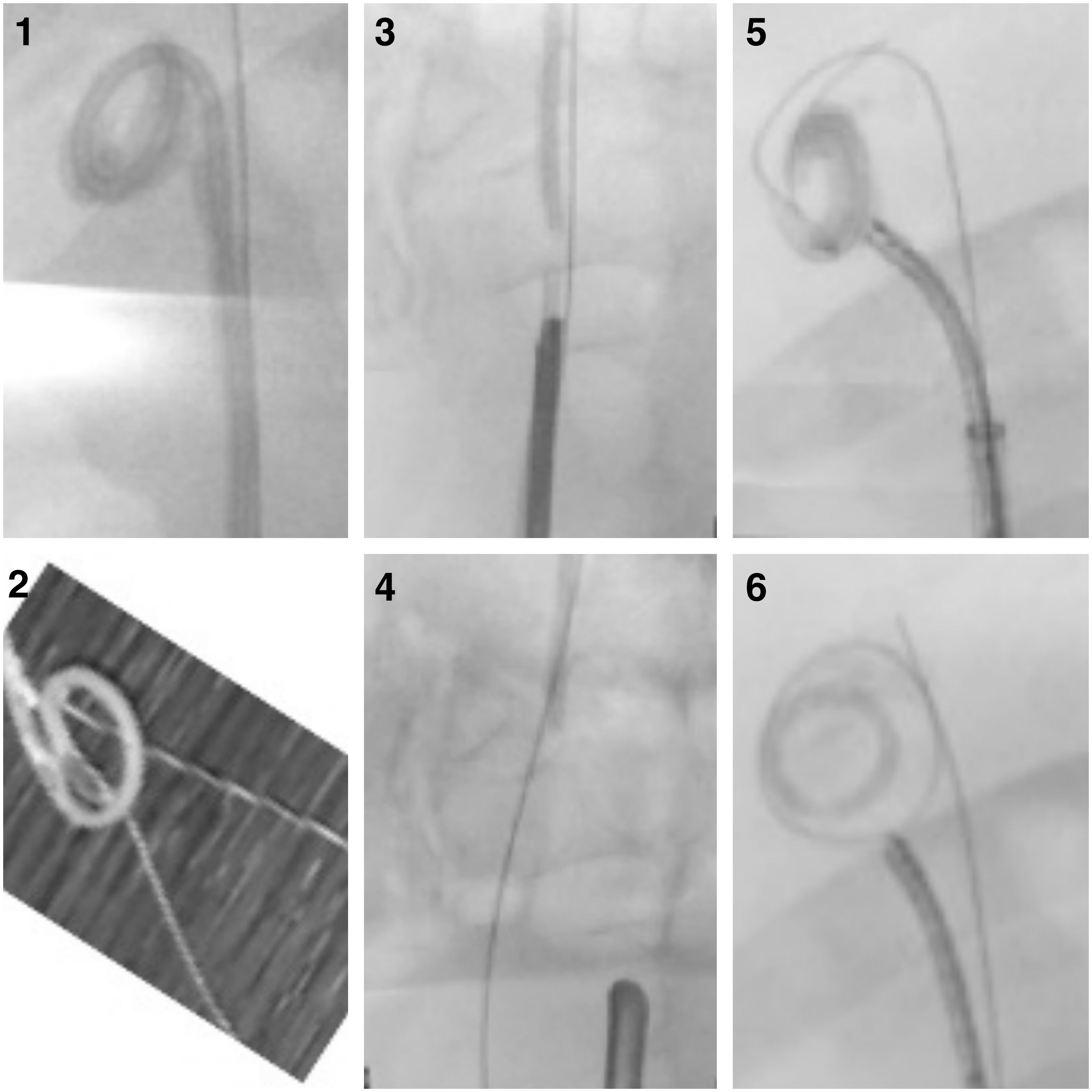
Steps of surgery:
UAS = ureteral access sheath.
An ureteroscopic approach to the middle part of the stent was then performed using a semirigid ureteroscope (6.4/7.8F). In all cases, ureteral distension provided by the indwelling stent allowed enough space for endoscope progression along the stent, regardless of its diameter (range to 4.8–7F). Indeed, the encrusted stent did not adhere to the ureteral mucosa in its middle section. The aim of this technique is to advance as proximal as possible next to the ureteral portion of the encrusted stent. If the renal pelvis was reachable, the cleansing of the proximal loop was sufficient to allow the uncoiling of the stent and its free removal. However, in most of the cases it was impossible to progress beyond the ureteral part of the encrusted stent. Thus, the Double-J stent was divided using the Ho:YAG laser cutting setting (10 Hz–1.0 J) to create space and allow further progression of the ureteroscope. The distal free portion of the stent was removed with a hooked-prong grasping forceps. The stent was usually cut twice to permit access to the upper encrusted curl. When the proximal part of the remaining stent was short enough, it was flushed into the renal pelvis to have more space to work. Then, a ureteral access sheath (UAS) could be easily inserted and flexible ureteroscopy (FURS) could be used to achieve fragmentation of the upper encrusted curl and its removal. Depending on the surgery length, any concomitant kidney stones could be treated in the same session or during the next procedure. In our series, owing to the complexity and length of the procedure, we almost always placed a new Double-J stent or ureteral stent at the end of the surgery.
Statistical analyses
A number of patient- and surgery-related parameters were assessed. Spectrophotometric analysis of encrusted components was carried out whenever possible. Immediate outcomes were recorded. Statistical analyses were computerized with the StatView® statistical software package using the chi-squared test for nominal variables and the Mann–Withney test for continuous variables. A value of p < 0.05 was considered statistically significant.
Results
The retrograde ureteroscopic approach with Ho:YAG laser allowed us to remove almost all of the encrusted and retained ureteral stents (98%) during a single general anesthetic procedure. Only one upper loop of an encrusted stent was unreachable owing to severe proximal ureteral stenosis, which necessitated percutaneous nephrolithotomy access. The operative and postoperative data are summarized in Table 3.
RIRS = retrograde intrarenal surgery.
Most of the patients (88%) had concomitant kidney stones not associated with the encrusted stent. In 23 patients, these residual stones and the encrusted stent were removed after only one RIRS procedure. The other patients required multiple surgical procedures to remove associated intrarenal stones. One additional RIRS was performed in 15 patients (29%) and two additional procedures in five patients (10%). In the patient with ureteral stenosis, a percutaneous tube was placed at the end of the retrograde procedure and percutaneous extraction of the proximal loop was achieved.
The ureteroscopic procedure was performed with semirigid ureteroscopes, flexible ureteroscopes, or the combination of the two. Ho:YAG laser transection of the stent was useful in 36 patients (71%). The stent was cut once in 10 cases (20%) and twice in 26 cases (51%). The calcification of the proximal component of the stent was sometimes achieved by semirigid ureteroscopy but mainly with FURS after UAS insertion.
At the end of the procedure, a new Double-J stent was placed in 40 patients (78%) and a ureteral stent was placed in eight patients (16%).
The mean operative time was 110 ± 35.2 minutes (range 42–225 minutes). Mean postoperative hospital stay was 2.33 days, and four patients (8%) were discharged home on the day of surgery.
No major intraoperative complications were recorded. The incidence of immediate postoperative complications was 12% and included mainly nonobstructive pyelonephritis. The oldest female patient developed major sepsis, requiring admission in the intensive care unit. No prolonged hematuria or ureteral fistulae were recorded. No blood transfusions were required.
In our study, there was not statistically significant relationship between the emergence of pyelonephritis and operative time (p = 0.12), body mass index (p = 0.56), gender (p = 0.87), or with the degree of encrustation of the stent (p = 0.16). On the contrary, the presence of struvite was positively correlated with postoperative pyelonephritis (p = 0.018).
The spectrophotometric stone analysis is shown in Figure 2.
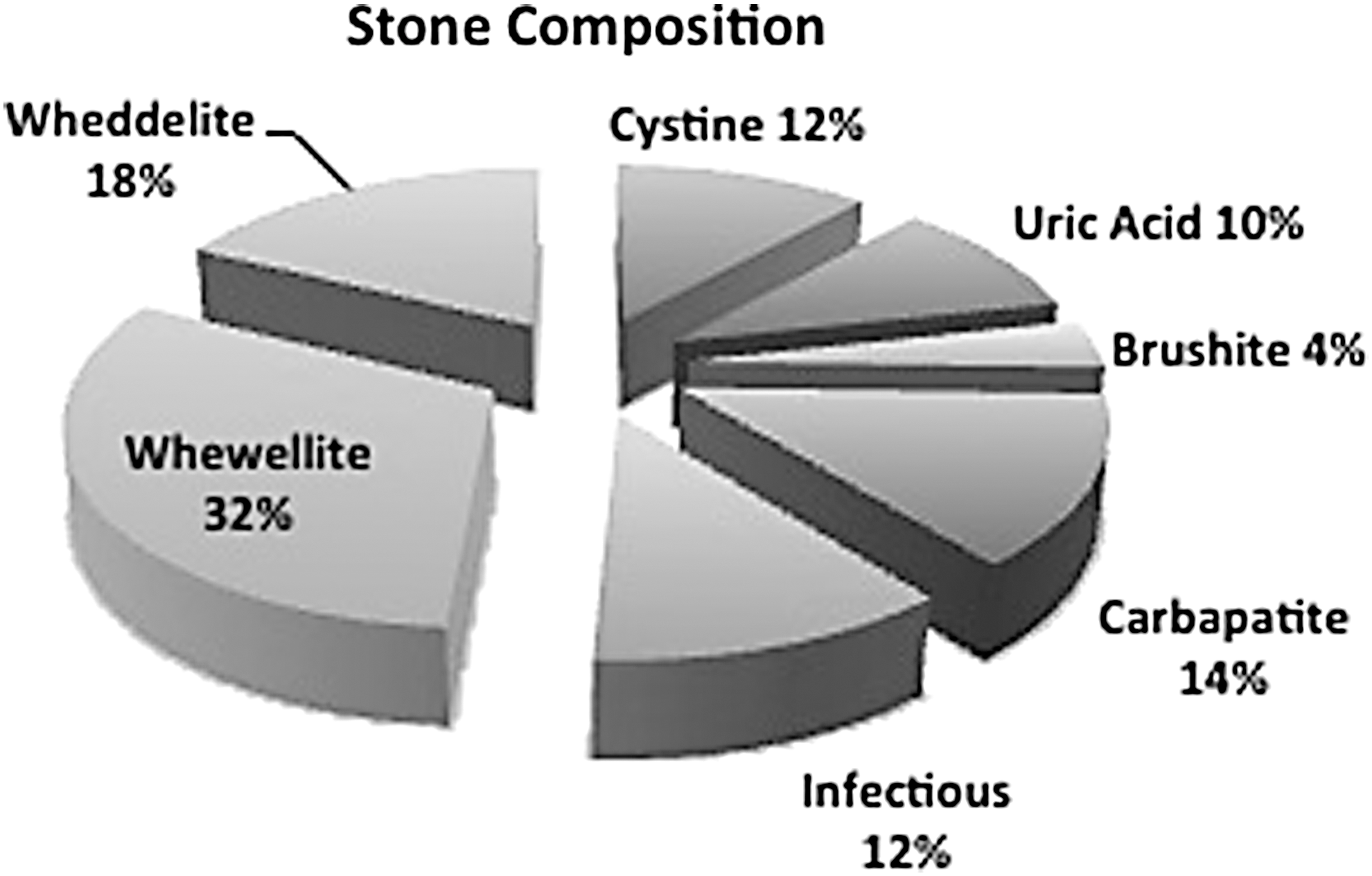
Stone composition.
Discussion
Retrograde ureteroscopic treatment of encrusted stents has been previously described in the literature 19 but often included percutaneous access to treat the proximal loop. 10 Here, we propose a new technique for retained encrusted stent management using only retrograde ureteroscopic access. We report the dividing of indwelling stents using the Ho:YAG laser to allow access to the intrarenal collecting system. This must be done without overdistension of the renal pelvis to avoid contaminated fluid reabsorption, iatrogenic trauma, or bleeding. The urologist should alternate filling and draining the irrigation fluid to prevent intrarenal overpressure. FURS has the advantage of being less invasive than the percutaneous approach. Another main advantage of our proposed technique is to render the ureter stent free, allowing UAS introduction and thus a low-pressure RIRS procedure. The proximal loop can also be removed through the UAS to avoid injury to the ureteral wall.
Bedke and colleagues 20 previously reported in vitro foreign body fragmentation, in particular ureteral stent catheters, using Ho:YAG laser fibers. In our in vitro experimentation, all biomaterial components of the Double-J stent could be cut. Richards and colleagues reported effective treatment of a stent knot in the upper ureter by cutting the stent with the laser. 21 According to our knowledge, nobody has described this technique for treating encrusted ureteral stents. In our series, we split the Double-J stent either once or twice in each patient. Although a single operative session allowed us to remove the stent in almost all patients, many of them (41%) required several FURS procedures to handle associated stone burdens.
This technique appears as reliable as other combination techniques in the literature. Nevertheless, FURS has the disadvantage of low efficacy in the removal of large stones. Thus, given the miniaturization of the percutaneous approach, patients with large associated stone burdens could benefit from a minimally invasive endoscopic combined intrarenal surgery to limit complementary surgical sessions. 22 However, therapeutic strategy is also determined by the accessibility of advanced equipment and availability of one or more experienced surgeons. With high-performance endourologic possibilities, open surgery becomes necessary more rarely.
The results of spectrophotometric stone analysis revealed that cystinuric patients represented 12% of our population. In this specific subgroup, the mean indwelling time leading to encrustation was much lower than in the overall study population (average 4.8 months) but with fewer complications. Pregnancy has also been reported as a risk factor for encrustation, probably because of the higher rate of asymptomatic gravid bacteriuria. 2 In this specific population, the mean time that the stent was in place was 3.3 months, with no postoperative complications reported.
Our principal postoperative complication (12%) was pyelonephritis, which was associated with severe sepsis requiring intensive care in one older woman. We did not register any postoperative deaths but this kind of procedure can lead to potentially lethal infectious complications, as previously described in the literature. 3 It seems that a pure retrograde approach did not raise the risk of severe complications when compared with the combination of percutaneous and retrograde techniques. 2,17,23
Despite the fact that urine cultures were negative before the procedure, the encrusted stent is usually covered by a biofilm, including bacterial colonization that is not affected by oral or intravenous antibiotic therapy. Bacterial cultures of the stent and stone fragments were generally positive, indicating that antibiotic therapy was not effective. A potential disadvantage of all endourologic techniques in such a compromised patient is the risk of bacteremia and sepsis arising from endoscopic manipulation of colonized stents and stone fragments. All precautions should be taken against urinary sepsis, as it carries a high mortality rate, especially in impaired patients. The occurrence of urinary sepsis after endoscopic intervention is extremely unpredictable. In our study, the most significant predictor of this life-threatening complication was the presence of struvite stones associated with the encrusted stent.
The limitations of this study include the lack of quantification of the encrustation rate and associated stone burden. However, appreciation and measurement of the calcified proximal stent loop and associated stones is extremely complicated and does not predict the outcome of endourologic procedures or potential bacterial spread.
In our study, the reasons for delayed management of patients were essentially misinformation, poor compliance, concomitant medical problems, and the availability of tertiary centers for coverage of complex pathologies. Because the mean time until a stent becomes moderately or heavily encrusted is difficult to determine and likely patient and situation dependent, we recommend removing Double-J stents as soon as possible to avoid potential encrustation. 7 It is essential to robustly inform patients about this risk and keep track of stented patients. Misinformation and iatrogenic complications of long time indwelling stents can also lead to legal ramifications.
Conclusions
Encrusted ureteral stents can be effectively managed with a retrograde ureteroscopic approach alone, using semirigid and flexible endoscopes. Fragmentation of encrustation over the stent and cutting the stent itself can be achieved safely with the holmium laser.
Footnotes
Author Disclosure Statement
All authors have made a substantial contribution to the information or material submitted for publication. All have read and approved the final manuscript. O.T. is consultant for Rocamed/Socomed, American Medicals Systems (AMS)/Boston Scientific, Coloplast, Olympus, and Lumenis. All authors declare that no funding or other agreement has limited their ability to fairly complete and publish this research study. There has been no extra-institutional funding for this study. A.T. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.