
Abstract
Objectives:
To observe serum creatinine (SCr) and treated side glomerular filtration rate (TGFR) variations in patients with upper urinary tract calculi after minimally invasive percutaneous nephrolithotomy (MPCNL).
Patients and Methods:
A total of 178 patients underwent MPCNL in our institute and they were retrospectively evaluated between May 2014 and February 2016. SCr and TGFR variations were observed with renal scintigraphy using 99mTc-diethylene triamine pentaacetic acid (99mTc-DTPA) preoperatively and after at least 6 months of follow-up (FU). The patients were categorized into two groups according to the number of percutaneous access tracts: group I (single tract, n = 122) and group II (multiple tracts, n = 56).
Results:
At a mean FU of 7.6 months, SCr dropped from 192.9 ± 151.9/L to 167.6 ± 113.9 μM (13.15% decrease, p = 0.008) and TGFR increased from 29.8 ± 21.2 mL/minute preoperatively to 32.7 ± 22.5 mL/minute postoperatively (9.79% increase, p = 0.022) in group I. Similarly, SCr dropped from 238.5 ± 130.1 to 215.8 ± 128.1μ (9.50% decrease, p = 0.013) and TGFR increased from 29.6 ± 21.4 mL/minute preoperatively to 32.9 ± 25.1 mL/minute postoperatively (11.17% increase, p = 0.014) in group II. No statistically significant difference between two groups according to SCr or TGFR variation was observed (p > 0.05).
Conclusions:
Stone clearance resulted in improvement of split kidney function after single tract or multiple tract MPCNL. Single tract or multiple tract MPCNL did not show statistically significant difference in split renal function postoperative recovery.
Introduction
U
Stone removal can improve renal function by resolving obstruction and eradicating underlying infections, but stone-removing procedures can also have a potential negative impact on functional integrity. Performing PCNL in difficult cases, for example, staghorn calculi, may require multiple access tracts to achieve stone-free rate (SFR). It is a worldwide concern that PCNL can potentially cause long-term renal damage as the renal parenchyma is insulted directly.
Since 20 years, we have performed minimally invasive percutaneous nephrolithotomy (MPCNL) for patients with upper urinary tract stones. This procedure has been proven to be effective to treat large and complex stones. 6,7 In the present study, we aimed to compare the impact on renal function of single tract vs multiple tract MPCNL.
Patients and Methods
Patients
This study was conducted at our institution and was approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University.
Patients with upper urinary tract calculi appropriate for MPCNL were admitted in the study. Inclusion criteria have been as follows: patients who were 18–70 years old; patients who signed written informed consent; and patients with unilateral renal or (and) upper ureteral calculi. Patients who experienced following conditions were excluded from the study: previous kidney surgery, hypertension, diabetes, and presence of residual calculi ≥4 mm evaluated with a noncontrasted abdominal CT after 6 months of follow-up (FU). Patients were categorized into two groups according to the number of percutaneous access tracts established: group I (single tract) and group II (multiple tracts).
Methods
All the patients had both preoperative contrasted or noncontrasted CT and intravenous urogram studies. Laboratory tests included routine blood test, blood biochemistry, urinalysis, urine culture and sensitivity, and coagulation study. Kidney function has been evaluated with serum creatinine (SCr) and treated side glomerular filtration rate (TGFR) measured by scintigraphy with 99mTc-diethylene triamine pentaacetic acid (99mTc-DTPA) preoperatively and after at least 6 months of FU. We utilized a modification of the Schlegel program developed by Gates. It involves computer analysis of scintigraphic images of the bilateral kidneys after a single intravenous injection of 99mTc-DTPA to calculate the TGFR. 8 Complications were recorded according to the modified Clavien classification system. 9
MPCNL technique
MPCNL is a modified PCNL using miniaturized nephroscope through a 14F–18F nephrostomy tract. This technique has been previously reported. 6 Single surgeon (Dr. Yongda Liu) performed all MPCNLs. All the procedures were performed under general anesthesia. The patients were first placed in lithotomy position, and an open ended 5F ureteral catheter was inserted in retrograde manner into the affected renal pelvis, and a Foley catheter was placed. The patients were next turned into prone position. An 18-gauge coaxial needle was used to puncture the targeted calix under either fluoroscopic or ultrasonographic guidance. A flexible 0.035-inch flexible guidewire was next inserted into the renal collecting system or passed down into the ureter through the needle sheath. Nephrostomy tract dilation was performed from 8F to a maximum of 18F using fascial dilators. Lithotripsy was performed using pneumatic lithotripter through an 8.5F/11.5F nephroscope. The stone fragments were either removed with forceps or flushed out with pulse perfusion pump. To achieve a satisfactory result, one or more 18F percutaneous tracts were sequentially established to remove all stones in a single session. At the end of the procedure, a 5F Double-J stent was positioned under direct vision, and one or more nephrostomy tubes were placed in the patients. Patients obtained kidney, ureter, and bladder radiograph on the first postoperative day to guide the decision for two-stage treatment, which was generally carried out 3–5 days later. In the two-stage treatment, a second look was performed to remove the residual stone fragment through the existing tract or one or more percutaneous tracts were added to achieve a satisfactory result as required.
Statistical analysis
Numerical data were recorded as mean ± standard deviation. SCr and TGFR were compared preoperatively and postoperatively with Wilcoxon signed-rank test. Comparisons for mean changes in SCr and TGFR between groups have been done with Student's t-test. Values for p < 0.05 were considered statistically significant. SPSS13.0 software was used for the statistical analysis.
Results
Between May 2014 and February 2016, a total of 178 patients were enrolled in the study. One hundred and twenty-two patients (68.5%) underwent single tract MPCNL and were enrolled in group I, while 56 patients (31.5%) underwent multiple tract MPCNL and were enrolled in group II. The characteristics of patients are presented in Table 1, and the outcomes and complications are presented in Table 2.
Statistically significant.
BMI = body mass index.
Statistically significant.
Twelve (9.8%) patients in group I and 14 (25.0%) in group II experienced Clavien grade I complications (fever). It was statistically significant (p = 0.008). Perioperative blood transfusion (Clavien grade II) rate occurred in 1.6% and 7.1%, group I and group II, respectively (p = 0.148). One patient in group I required selective renal artery embolization for severe hemorrhage. We managed all complications conservatively.
Mean FU was 7.6 months (ranged from 6 to 12 months). Mean SCr levels and TGFR of both groups before and after MPCNL are presented in Figures 1 and 2. SCr significantly decreased in both groups of 13.15% and 9.50%, respectively (p < 0.05). TGFR significantly increased in both groups of 9.79% and 11.17%, respectively (p < 0.05). There was no significant difference between two groups according to SCr or TGFR variation (p > 0.05).
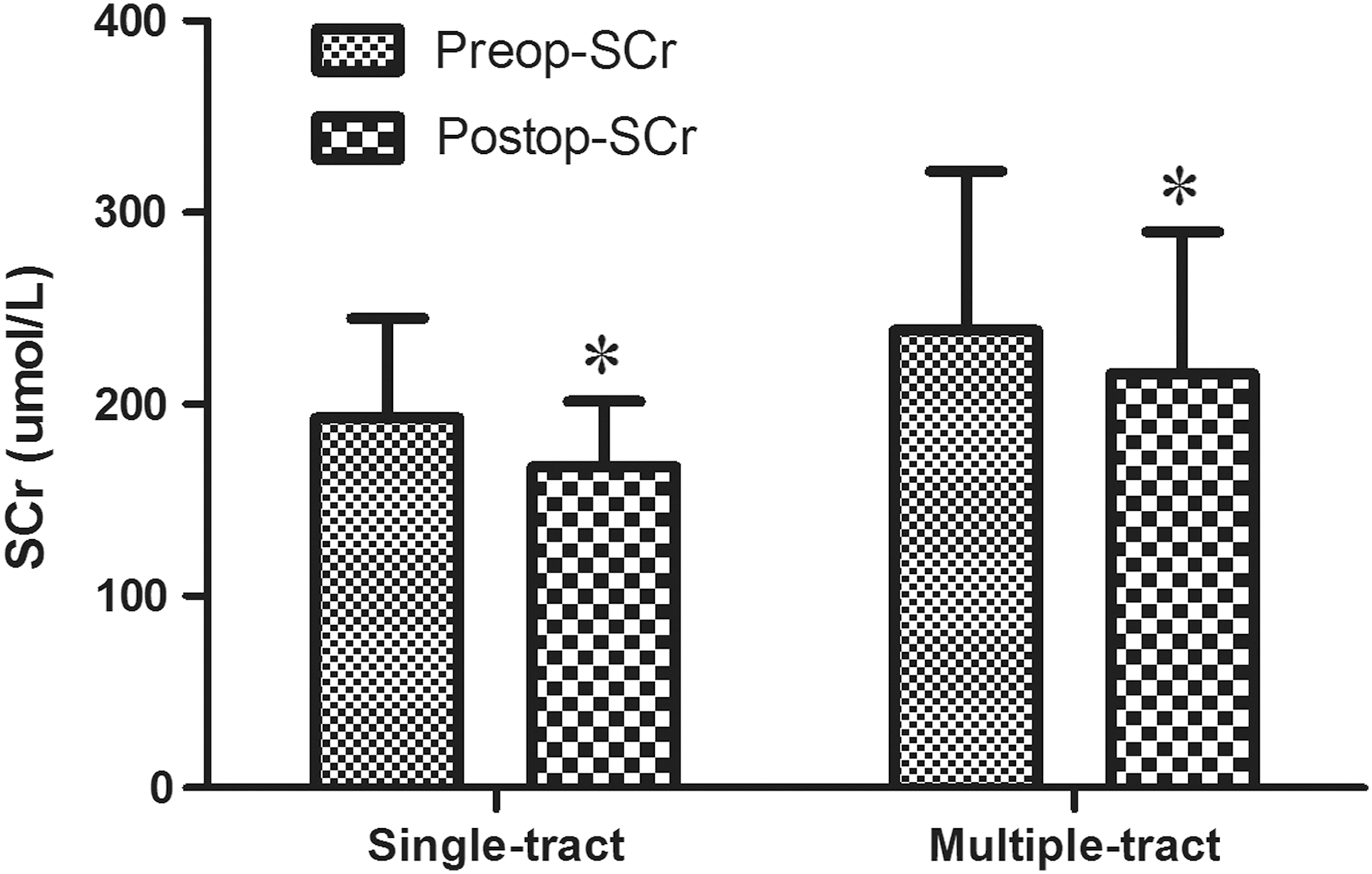
SCr variation in patients treated with single or multiple tract MPCNL. *p < 0.05 from preoperative values. MPCNL = minimally invasive percutaneous nephrolithotomy; SCr = serum creatinine.

TGFR variation in patients treated with single or multiple tract MPCNL. *p < 0.05 from preoperative values. TGFR = treated side glomerular filtration rate.
Discussion
PCNL damages kidney parenchyma determinating a permanent scar at the site of the nephrostomy tract. 10,11 The aim of this study was to determine whether single tract or multiple tract MPCNL would worsen kidney function. To our knowledge, this is the first study designed to analyze renal functional outcomes after MPCNL. Our results showed that patients in both groups had a statistically significant decrease in SCr and significant increase in TGFR regardless of the number of percutaneous access sites, suggesting that stone clearance resulted in significant improvement in renal function after single tract or multiple tract MPCNL.
PCNL is the technique of choice in treating large and complex renal stones. 3 –5,12 Meticulous clearance of stones with nephron preservation should be aimed in the treatment of renal calculi. In the setting of large staghorn calculi, more than one percutaneous access may be required for stone clearance. In performing PCNL, we must also balance the need of high SFR to the demand for minimizing complications and maximal preservation of renal function. It is a worldwide concern that PCNL can potentially cause long-term renal damage as the renal parenchyma is insulted directly. In several reports, improvement in renal function after PCNL has not been found. 13,14
Nevertheless, these analyses use laboratory-based parameters, such as estimated glomerular filtration rate (eGFR) to assess renal function and it provides some bias in evaluating renal function. 15,16 Nuclear renography is a much more accurate technique to assess split renal function in post PCNL patients. 99mTc-DTPA is utilized to assess renal function of each unit; consequently the comparisons of pre- and postoperative 99mTc-DTPA can precisely evaluate the functional effects of PCNL of the affected kidney. 17
Schiff and associates prospectively evaluated 33 patients undergoing unilateral PCNL. A renal scintigraphy using 99mTc-DTPA was performed between 3 and 12 months. They found no significant functional change. 18 Similar results were reported by Ekelund and associates. They found that there was a moderate decrease in renal function 1 day postoperatively, but returned to near baseline values at 14 days. 19 Wadhwa and associates calculated glomerular filtration rate (GFR) using 99mTc-DTPA in nine pediatric renal units and found no overall change in GFR at 3 months after PCNL compared with preoperative levels. 20 Recently, Fayad and associates eGFR using 99mTc-DTPA in 102 patients undergoing PCNL with multiple access tracts (2–4 tracts) and found that GFR of the involved renal unit at 12 months decreased significantly compared with preoperative values. 21
In the current study, the impact on renal function of MPCNL appeared to be different. Our results showed that the treated renal unit had a statistically significant increase in GFR after single tract or multiple tract MPCNL.
First, in our study all cases were performed by a single surgeon under the same protocol to minimize a surgery-effect bias. Previous research found different dilation methods or the dilation technique itself could result in modifying degrees of renal parenchyma injury. 22,23 We also excluded the bias of risk factors such as hypertension and diabetes as they potentially would modify renal function deterioration after PCNL. 21
In addition, over 66% of patients in our study had large stone burden with moderate-to-severe hydronephrosis. In this category of patients, complete stone clearance can improve renal function by eradicating obstruction and underlying infection.
Furthermore, compared to conventional PCNL (24F–34F), MPCNL requires a much smaller nephrostomy tract (14F–18F), which reduces the renal parenchymal injury. These factors promote an improvement in function for stone removal through this approach.
Conversely, the limitation of this study is the small number of patients with more than two tracts. In fact, most of our multiple tract MPCNL had just two access tracts. Thus, it is impossible for us to stratify groups by the number of accesses and find a difference in pre- and postoperative renal function among more than two-tract MPCNL. It is unknown whether the recovery in renal function can be delayed as the number of MPCNL tract increased. However, we believe that additional tracts can increase the risk of parenchymal injury and the cumulative effect could potentially lead to a reduction in kidney function. Therefore, it is advisable to utilize minimal number or smaller MPCNL tracts that achieved optimal stone removal with the least degree of injury to the renal parenchyma.
Conclusion
MPCNL effectively decreases the morbidity associated with multiple access tracts because of their thinner dimensions compared to standard PCNL. The procedure promoted an improvement in split renal function for stone removal.
Footnotes
Acknowledgments
This work was financed by grants from the Science and Technology Department of Guangdong Province, China (No. 2016A020212023) and Science and Technology project in Guangzhou (No. 201507020026).
Author Disclosure Statement
No competing financial interests exist.