
Abstract
Objective:
To compare the oncologic and functional outcomes of partial vs whole-gland cryotherapy for men with intermediate-risk prostate cancer.
Subjects/Patients:
Men with intermediate-risk prostate cancer treated with primary prostate cryotherapy from 1993 to 2013 were selected from the Cryo On-Line Data Registry for a 1:1 matched comparison between those undergoing whole-gland and partial prostate cryotherapy (targeted ablation, unilateral/bilateral nerve-sparing ablations). A propensity score was developed based on age, prebiopsy serum prostate-specific antigen, biopsy Gleason score, clinical stage, prostate volume, neoadjuvant androgen deprivation status, year of surgery, and pretreatment potency. Outcomes were biochemical progression-free survival (BPFS) using the American Society for Therapeutic Radiation Oncology (ASTRO) and Phoenix criteria, 12-month continence (strictly pad free), and sexual function (potency sufficient for sexual intercourse). After propensity score matching, BPFS was compared using Kaplan–Meier analysis and functional outcomes using chi-square tests.
Results:
In all, 897 men were identified (731 whole gland and 166 partial). Postmatching, 166 pairs of men were analyzed (mean follow-up 31 months). The 2/5-year BPFS rate was 87.2%/76.4% for whole-gland vs 80.7%/70.0% for partial ablation using Phoenix (p = 0.26) and 72.3%/69.6% for whole-gland vs 82.1%/75.0% for partial ablation using ASTRO criteria (p = 0.10). Of 164 pairs, the 12-month continence rate was similar, 94.1% vs 95.1% (p = 0.803). Of 139 pairs, the 12-month rate of effective intercourse was 29.5% for whole-gland and 46.8% for partial ablation (odds ratio 2.1, p = 0.003). The incidence of post-treatment urinary retention was 6.0% and 6.6% (p = 0.88) following whole-gland and partial ablation, respectively, and that of rectourethral fistula was 1.2% and 0% (p = 0.50).
Conclusion:
Partial ablation results in better post-treatment sexual function compared with whole-gland ablation in men with intermediate-risk prostate cancer. We did not observe a difference in early BPFS between the two groups.
Introduction
P
It is currently thought that low-risk prostate cancers are highly representative of latent cancers that would be unlikely to harm men with observation alone. 3,4 On the contrary, high-risk prostate cancers have a highly aggressive potential and there is often concern that they are metastatic early in their course. 5 These tend to present at a later stage and a high proportion of them require multimodality treatment with radical surgery, radiation, and/or androgen deprivation. 6 The two ends of the spectrum were eloquently summarized by Whitmore that cure seems possible only in those whom it is really unnecessary and impossible in those whom it is truly necessary. 7
Intermediate-risk prostate cancer as defined by D'Amico criteria, a maximum of Gleason sum 7 or a prostate-specific antigen (PSA) >10 to 20 ng/mL or a maximum clinical stage T2b, represents a mid-spectrum range of diseases that might potentially be cured with local treatment. 8 Furthermore, a subset of these patients with low-volume intermediate-risk cancer could be treated with focal therapy to downgrade them to a criteria through which they become suitable for active surveillance. 9 Focal therapy would theoretically lower the functional impact of treatment that is seen with traditional radical therapies.
Our objective is to compare the oncologic and functional outcomes of men with D'Amico intermediate-risk prostate cancer undergoing partial gland cryotherapy vs whole-gland cryotherapy in the Cryo On-Line Data (COLD) registry. Herein, we report our findings.
Patients and Methods
The COLD Registry is supervised by a scientific board of urologists, and an independent audit of the scientific data is conducted yearly at randomly chosen centers to ensure the accuracy of data. Although industry sponsored (HealthTronics, Austin, TX), all registry data collection was performed by an independent research company (Watermark Research Partners, Indianapolis, IN). All participating sites that were required to do so had approval from their institutional review board (IRB) before submission of any data to the registry database. A global IRB protocol has been in place since 2006. 10,11
In this report, we adopted the Strengthening The Reporting of Observational Studies in Epidemiology (STROBE) guidelines for a complete and accurate description of our methods. 12
Patients
We queried the COLD registry for all patients with D'Amico intermediate-risk (Gleason 7 or PSA >10–20 ng/mL or clinical stage T2b) prostate cancer undergoing primary prostate cryotherapy from 1993 to 2013. We excluded patients who had received prior treatment with radiation, surgery, or ablation to the prostate gland.
Cryotherapy procedure and patient grouping for ascertainment of therapeutic effect
The COLD registry classifies the type of cryotherapy as whole-, subtotal, or partial gland treatment. As a community-based registry, the type of cryotherapy device used, patterns of cryoprobe placement, and extent of nerve sparing (unilateral vs bilateral) vary according to the user and this information is not always available in sufficient quantity or quality for analysis. In general, the community standard practice is a double freeze/thaw cycle with a nadir temperature goal of −20°C to −40°C. 13 The use of a urethral warming catheter and temperature probes to monitor the Denonvilliers' fascia and the urethral sphincter has been the standard of care since the early 2000s. 14 We excluded men who underwent subtotal cryotherapy and grouped the remaining men into those who had undergone whole-gland cryotherapy vs those who had undergone partial gland cryotherapy for further analysis.
Outcome measures
Oncologic control was defined by biochemical progression-free survival (BPFS) and for-cause postprocedure biopsy. Biochemical progression was defined by the Phoenix criteria (PSA nadir +2 ng/mL) and the American Society for Therapeutic Radiation Oncology (ASTRO) criteria (three consecutive rises of PSA with date of failure the midpoint between post-treatment nadir and the first rise). 15,16
Continence was defined as strictly no pad use reported by the patient to the physician at the 12-month visit after cryotherapy. Potency was defined as the ability to have sexual intercourse with or without erectile aids, determined by the physician at the 12-month visit after primary cryotherapy. Complications recorded in the COLD registry include post-treatment urinary retention and the incidence of rectourethral fistula. The data were independently entered and verified by Watermark Associates.
Statistical analysis
Statistical analysis was performed using Stata 13.1 (StataCorp, TX). The key factors affecting the choice of partial vs whole-gland ablation were clinically determined to be age (years), prostate volume (mL), initial PSA (ng/mL), Gleason score (≤6 vs 7), clinical stage (≤cT1c, cT2a, or cT2b), the year of surgery (1993 to 2013 in quartiles), the use of hormonal therapy (yes or no), and potency (ability to have sexual intercourse—yes or no) before treatment. Using Psmatch2, propensity scores based on these covariates were created with probit regressions separately for the outcomes of biochemical progression using Phoenix criteria, ASTRO criteria, 12-month potency rate, 12-month continence rate, post-treatment urinary retention, and incidence of rectourethral fistula, respectively. 17
Men undergoing partial gland cryotherapy were matched 1:1 with those undergoing whole-gland cryotherapy using a nearest neighbor method. Reduction in bias was determined by observing the distribution of the covariates, statistical testing using t-test for continuous covariates, and chi-squared tests for categorical covariates, as well as graphically observing the standardized difference in means before and after adjustment. The risk of significant bias was thought to be low if the standardized difference in means was less than ±0.1.
The impact of treatment selection on BPFS was determined using Kaplan–Meier analyses. The impact on 12-month continence and potency as well as post-treatment urinary retention and incidence of rectourethral fistula was determined using chi-squared tests. A p-value of <0.05 was accepted as the threshold of statistical significance and, where appropriate, the odds or hazard ratios and the 95% confidence intervals (CIs) were determined. When a significant risk of bias was observed in one or more covariates, we performed further sensitivity analyses using multivariate methods (Cox proportional hazards or logit regressions) to assess their impact on the effect of treatment.
Results
A total of 897 men with D'Amico intermediate-risk prostate cancer and complete data were identified from the COLD registry, with 166 men undergoing primary partial gland cryoablation and 731 men undergoing primary whole-gland cryoablation.
Biochemical progression-free survival
After propensity scoring and resampling with a 1:1 match, 166 matched pairs of men were available for analysis of our primary outcome. Patient demographics are shown in Table 1, and the postmatching change in standardized means is shown in Figure 1. The mean follow-up was 31 months (median 24). At Kaplan–Meier analysis, using the Phoenix criteria, while there was a trend toward poorer BPFS with partial vs whole-gland ablation (2-year BPFS 80.7% vs 87.2% and 5-year BPFS 70.0% vs 76.4%), this difference was not statistically significant (log rank, p = 0.26). Using the ASTRO criteria, there was a trend toward better BPFS with partial vs whole-gland ablation (2-year BPFS 82.1% vs 72.3% and 5-year BPFS 75.0% vs 69.6%), but this trend was not statistically significant either (log rank p = 0.10). The survival curves are demonstrated in Figures 2 and 3.
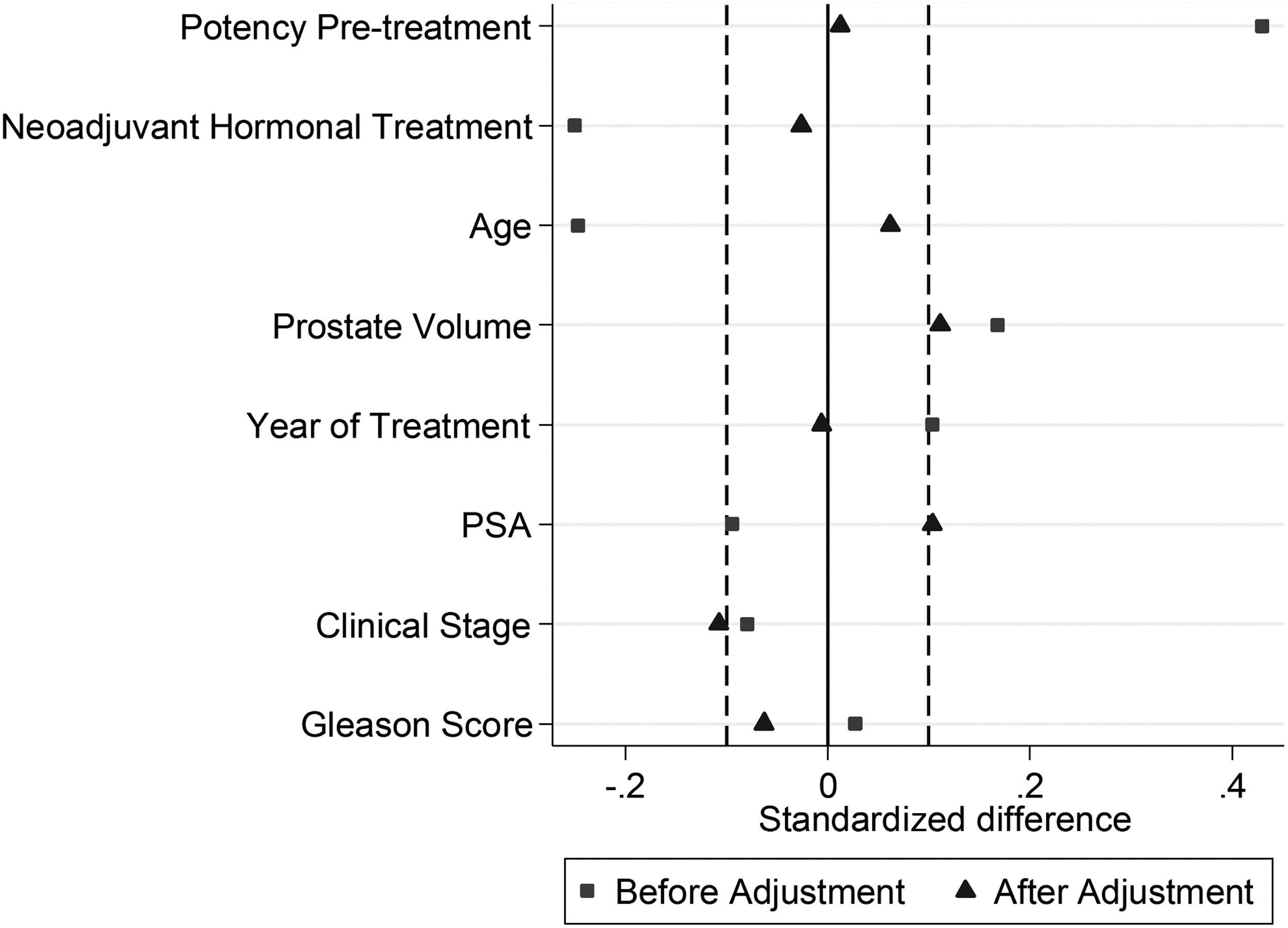
Standardized difference in means after matching for oncologic outcomes (biochemical progression-free survival). PSA = prostate-specific antigen.

Kaplan–Meier chart for partial vs whole-gland cryoablation using Phoenix criteria.
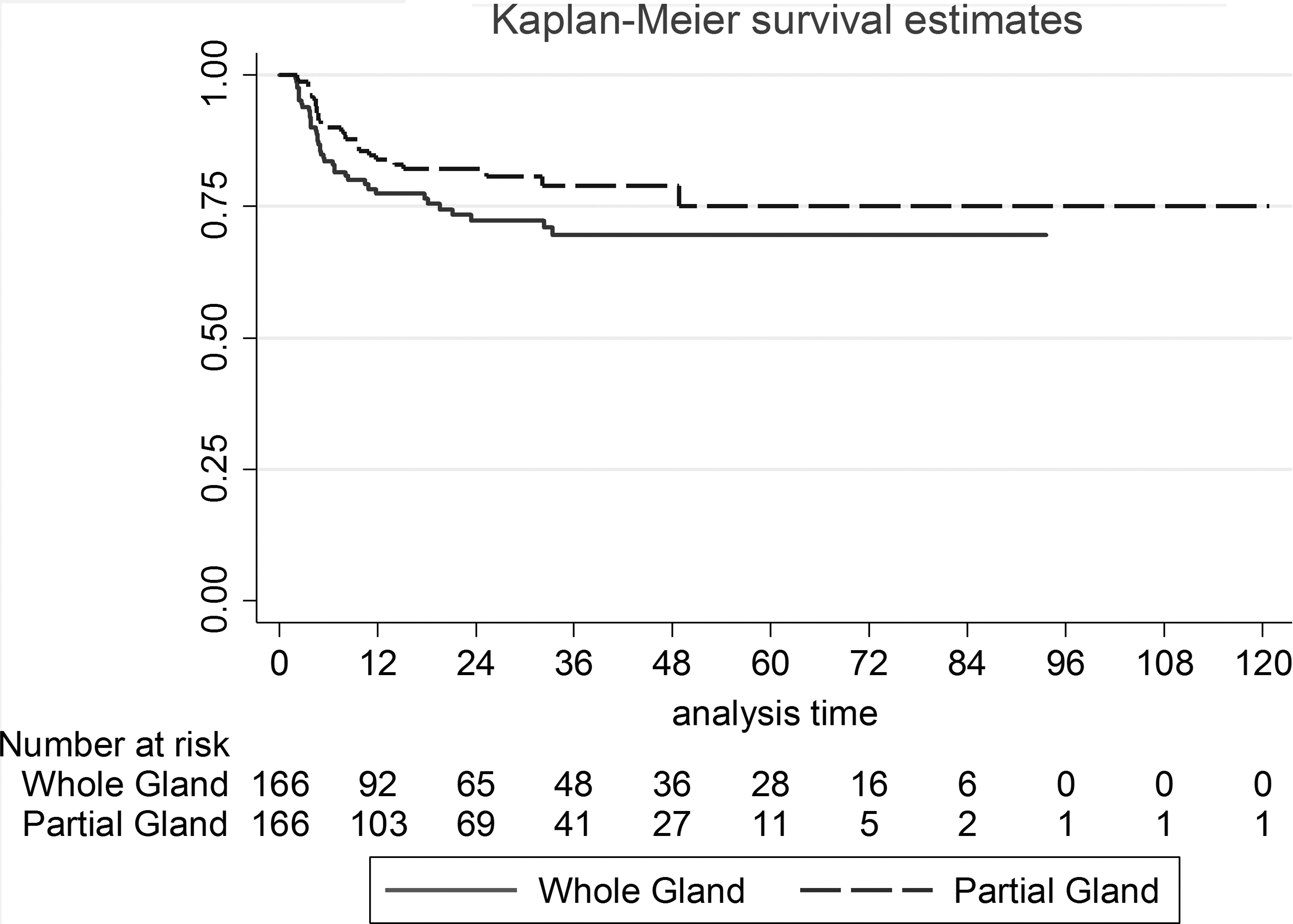
Kaplan–Meier chart for partial vs whole-gland cryoablation using ASTRO criteria.
BPFS = biochemical progression-free survival; PSA = prostate-specific antigen; SD = standard deviation.
Biopsy
Of the entire matched cohort, 26.2% of men underwent post-treatment biopsy (8.7% for-cause) with an overall biopsy positivity rate of 2.1%. The detailed biopsy outcomes are summarized in Table 2.
ASTRO = American Society for Therapeutic Radiation Oncology; WG = whole gland.
Functional outcomes
For the analysis of continence, 164 pairs of men were available. The 12-month continence rate was 94.5% for whole-gland ablation and 95.1% for partial ablation (p = 0.803). For the analysis of potency, 139 pairs of men were available. The 12-month potency rate was 29.5% for whole-gland ablation and 46.8% for partial ablation, with an odds ratio of 2.1 (95% CI 1.3, 3.4; p = 0.003). The demographics for both groups are shown in Table 3, and the postmatching change in standardized means is shown in Figure 4.
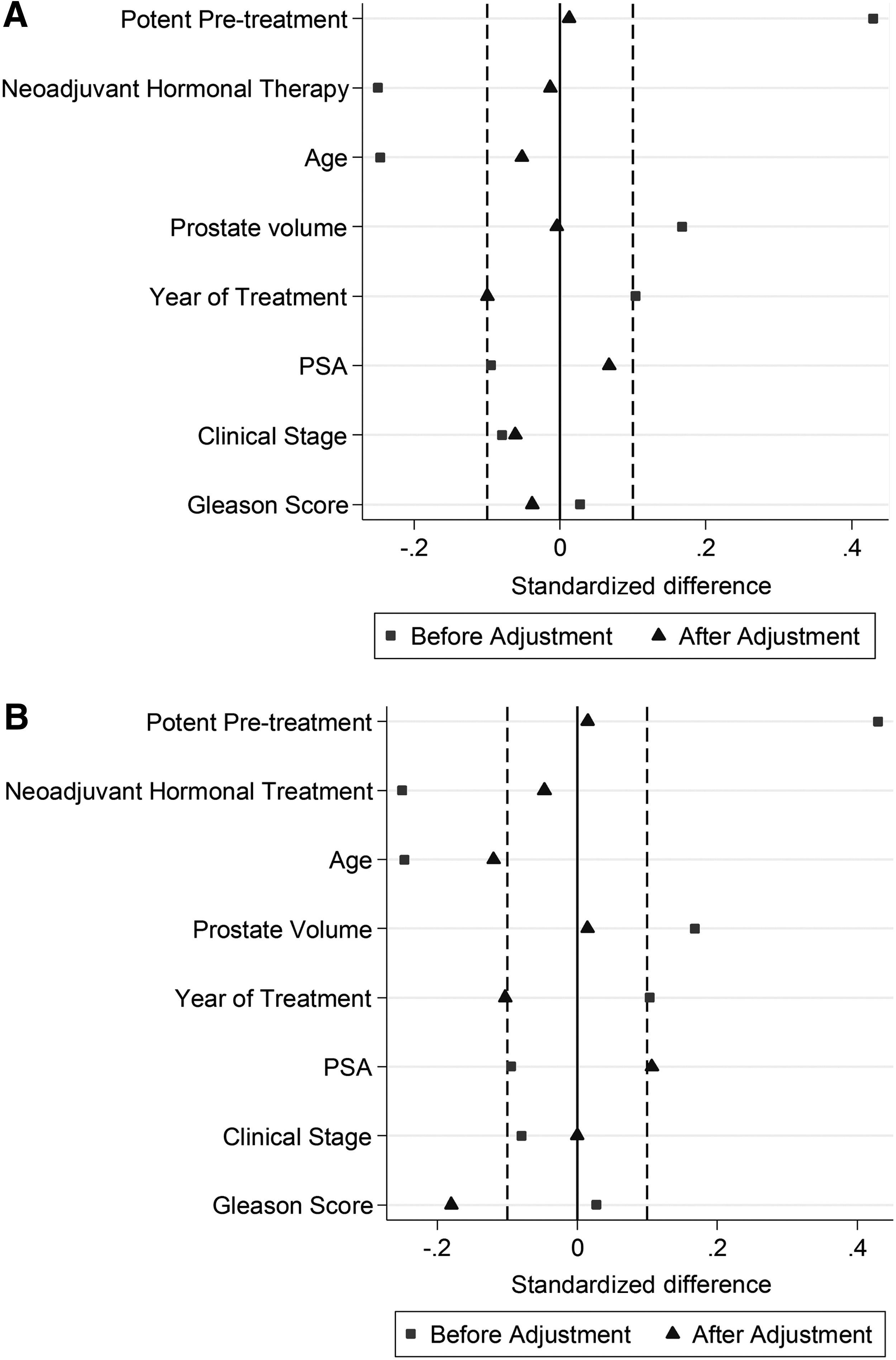
Standardized difference in means after matching for outcomes of
Complications
For the analysis of post-treatment retention and rectourethral fistula, 166 pairs of men were available. The incidence of urinary retention requiring prolonged catheterization was 6.0% for whole-gland ablation and 6.6% for partial gland ablation (p = 0.882). The incidence of rectourethral fistula was 1.2% for whole-gland ablation and 0% for partial gland ablation (p = 0.498).
Sensitivity analysis
Inclusion of covariates with a risk of bias due to imbalance in the groups did not significantly alter the observed treatment effects on BPFS and functional outcomes. Restriction of the analysis to men with a minimum follow-up of 24 months or 36 months extended the median follow-up to 48/56 months (Phoenix criteria) and 42/53 months (ASTRO criteria). No statistically significant difference was observed in biochemical progression rates (Table 4).
Too few events for analysis.
BPR = biochemical progression rate; NA = not applicable.
Discussion
When treatment is necessary, radical prostatectomy remains the gold standard as an extirpative oncologic therapy of prostate cancer. Radical radiation is also an established treatment option and the choice between the two is often made based on patient needs and side-effect profiles. With the advent of readily available advanced prostate imaging, there has been great interest in prostate focal therapy as a means to treat highly selected men with small targetable foci of clinically significant prostate cancer while sparing the remainder of the gland. This is thought to improve functional outcomes, but most current reports are early-phase cohort studies with no comparison arm. 18
It would thus be of great interest to compare the oncologic and functional efficacy of prostate focal therapy with radical whole-gland treatment. A randomized trial comparing focal ablation to the gold standard extirpative treatment would be decisive but onerous to implement. Whole-gland cryotherapy in the primary treatment setting has largely been utilized in older men with comorbidities who are excluded from established treatments. The present analysis of the COLD registry that includes both partial and whole-gland cryotherapy offers a unique opportunity to explore the concept of whole-gland vs partial gland treatment in a relatively homogenous group of patients with clinically significant prostate cancer.
In our analysis, the matched comparison for oncologic outcome using the Phoenix criteria showed a statistically nonsignificant trend toward poorer BPFS with partial gland ablation and an opposite trend with the ASTRO criteria. This likely represents the earlier detection of failures using the Phoenix criteria, although ultimately, we were unable to demonstrate a significant difference due to limited power.
On the contrary, sexual function after partial prostate ablation was twice as good as that after whole-gland ablation. After matching, 67% of men were sufficiently potent for sexual intercourse before treatment, of whom 70% remained so at 12 months after partial gland ablation compared with 45% after whole-gland ablation (odds ratio of 2.1). The overall recovery of sexual function in our cohort may have been impaired by older age (mean 69 years) and the use of neoadjuvant hormonal therapy (25%). Moreover, functional outcomes in focal ablation are highly dependent on the relationship of tumor location to the neurovascular bundle and this information was not captured by the registry, although the majority of partial ablations are likely to be hemiablations with unilateral nerve sparing, reflecting the practice in the community. Nonetheless, the findings in our partial ablation arm are comparable to the 58% to 100% potency rate reported in the literature. 18 It is unknown whether further functional recovery will occur out to 2 years with dissipation of the effect of hormonal therapy. Our present findings extend those of a prior matched-pair analysis of low-risk prostate cancer patients undergoing whole-gland or partial prostate ablation, which could be seen as a safety or phase I-type study given that most men with low-risk prostate cancer today are usually managed without active intervention. 19 The present data in men with intermediate-risk disease are highly relevant in the future deployment of focal therapy as there is likely to be a broader zone of ablation to ensure that negative margins are achieved.
Our study does have several limitations and must be interpreted within context. First, while post-treatment reductions in PSA of up to 30% to 60% have been observed, biochemical progression is not well established as a clinically meaningful endpoint after prostate focal therapy, largely due to the confounding effects of the remnant PSA-producing prostate parenchyma. 20 –23 An ideal early/intermediate-term endpoint would be a mandatory post-treatment biopsy. In our series, only 26% of men underwent post-treatment biopsy as biopsies were not mandatory. In a recent systematic review, the majority of men undergoing focal cryotherapy were followed with biochemical progression criteria only, with only 17% of men undergoing post-treatment biopsy. 18 In five cohort studies with a mandatory biopsy protocol, the compliance rate was 79%, highlighting the difficulties in the implementation of a mandatory follow-up biopsy strategy. 21,24 –27 Regardless, mandatory post-treatment biopsy, supplemented by multiparameteric MRI (mpMRI), should be an endpoint in future oncologic assessment of focal therapy.
Second, the duration of follow-up in our series is relatively short at a mean of 31 months (median 24 months), which impacts the sufficiency of duration for biochemical recurrence to occur. A sensitivity analysis restricting the analysis to men with a minimum follow-up of 24 or 36 months led to a much longer median follow-up, but did not change our findings that partial vs whole-gland ablation did not have a statistically different biochemical progression-free rate. Nonetheless, data should be interpreted with caution as an indication of the early post-treatment course only.
Third, accurate estimation of the treatment effect, or in this case, the effect of partial vs whole-gland cryotherapy, depends to a large extent on whether we were able to accurately match the two groups of patients. Propensity scoring allowed us to satisfactorily match for an aggregate of eight variables, all of which we determined to have some effect on choice of treatment, with less risk of overfitting than a multivariate regression. While the COLD registry does not capture the number of positive diagnostic biopsy cores, a critical detail factor in choosing focal therapy, we matched PSA and prostate volume as cancer volume surrogates for balancing the two groups. The reader should bear in mind that matching does not account for unmeasured factors that may bias the selection of one modality over the other.
Fourth, we did not use standardized quality-of-life tools to define functional outcomes. At the time the COLD registry was formed, there was no provision for the use of such tools. While these are in the process of being implemented, the patients in the relevant time period did not have these data available for analysis. The registry has used an extremely strict “no pad” definition of continence and erection sufficient for intercourse definition for erectile function, which were adopted before the recognition of the value of quality-of-life tools.
Last, mpMRI is now routinely recommended before prostate focal therapy. 28 It is able to better grade and localize the cancer within the prostate. 29,30 Our data set did not capture the use of imaging, and given the time period and the fact that the majority of contributors to the COLD registry are community practitioners, it is likely that mpMRI was minimally utilized. Pilot reports of MRI-ultrasound (MRI-US) fusion for delivery of cryotherapy have been published and we await further comparative data arising from these endeavors. 31
Despite these limitations, these data are worthy of being reported. First, using an extremely strict “no pad” definition of continence, 95% of men achieved this goal with cryosurgery at the 1-year mark. Second, focal therapy has become more targeted during the last few years, and a more refined application of lethal ice may further improve functional outcomes particularly when compared with a broader, hemiablation prototype that the majority of the men had received in this registry. Finally, the COLD registry represents a community experience of cryosurgery and thus has broad applicability as a snapshot of what is occurring across the United States in contrast to a single-institution or small clinical trial protocol.
Conclusion
Men with intermediate-risk prostate cancer undergoing partial prostate cryotherapy are more likely to achieve potency after treatment compared with those undergoing whole-gland cryotherapy. We did not observe a difference in early BPFS between the two matched groups.
Footnotes
Author Disclosure Statement
Dr. Tay received fellowship funding from the National Medical Research Council, Singapore. Dr. Polascik serves on the board of the COLD registry and has consulted for Endocare. Dr. Jones is Principal Investigator and Board Chairman of the COLD registry and has consulted for HealthTronics.