
Abstract
Introduction:
With the broadening indications of ureteroscopy (URS) for complex stones and high-risk patients, more URS is being performed and hence there is an increasing risk of major potentially life-threatening complications. We wanted to define the incidence, predisposing factors, management, and long-term sequelae for post-URS perirenal hematoma (PRH).
Material and Methods:
We conducted a systematic review of literature according to Cochrane and preferred reporting items for systematic reviews and meta-analysis guidelines for all studies reporting on post-URS PRH from 1980 to September 2016. A literature search was conducted through PubMed, EMBASE, CINAHL, and Cochrane Library for all English language articles.
Results:
Based on a literature search of 210 articles, seven studies (8929 patients) met the inclusion criteria with an incidence of post-URS PRH reported as 0.45% (40 patients, range: 0.15%–8.9% per study) with a mean age of 53 years and a mean stone size of 1.7 cm. The predisposing factors were moderate–severe hydronephrosis, thin renal cortex, prolonged operative duration, hypertension, and preoperative urinary tract infection (UTI). The management strategy varied from conservative management with blood transfusion and antibiotics (n = 22, 55%) to percutaneous drainage (n = 11, 27.5%). Surgical intervention was needed in seven (17.5%) patients. Two of these were emergency angiography of which one proceeded to open nephrectomy. Open surgery with clot removal was done in three patients, nephrostomy for severe hydronephrosis in one patient, and surgery to correct malpositioned stent in one patient. There was one mortality reported, wherein a patient who had postangiography nephrectomy died of multiple organ failure after the intervention.
Conclusion:
URS related PRH is a rare, but potentially life threatening complication with a small risk of renal loss. Although most cases may be managed conservatively, incidence of PRH can be minimized by control of blood pressure, treatment of preoperative UTI, and reduction in intrarenal pressures and operative time duration.
Introduction
U
A risk that is linked closely to perioperative bleeding is the formation of a perirenal hematoma (PRH). Typically, PRH is known to occur after other procedures, such as PCNL or SWL. They can also result from trauma or interventional radiologic procedures, or may even occur spontaneously, 4 especially in those who are anticoagulated. Post-URS PRH is mentioned recurrently in case series and reports, and although the number of cases remains low, they are an important finding that must be dealt with appropriately to avoid long-term morbidity. Studies have attempted to establish patterns among patients' predisposing factors, and suggest recommendations to minimize the risk of occurrence. This is the first systematic review to collate this evidence to provide a reference point for endourologists. Our objective was to investigate the incidence of post-URS PRHs observed in this literature, identify the common predisposing factors, and report on collected experience on the optimal preventative strategies, the most appropriate management of PRH and its long-term sequelae.
Methods
Search strategy
The systematic review was performed according to the Cochrane review guidelines and the preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines. A literature search was conducted through PubMed, EMBASE, CINAHL, and The Cochrane Library, without data restrictions, using the following search terms: “ureteroscopy,” “ureterorenoscopy,” “renal haematoma,” “renal haemorrhage,” “ureteroscopic,” “haematoma,” “ureterorenoscopic,” and “haemorrhage.” The last search date was September 28, 2016, and covered the time period from 1980 to September 2016.
Inclusion criteria
Articles written in the English language, from the given time period, which reported a PRH after URS, were eligible for inclusion. Patients of all ages and articles of any study type were considered. Single case reports were not included in the review; however, all of their references were examined to avoid missing a relevant study. One of our articles was identified through this method (listed as “other sources” in the PRISMA diagram in Fig. 1). Articles suspected to arise from duplicate studies were excluded.
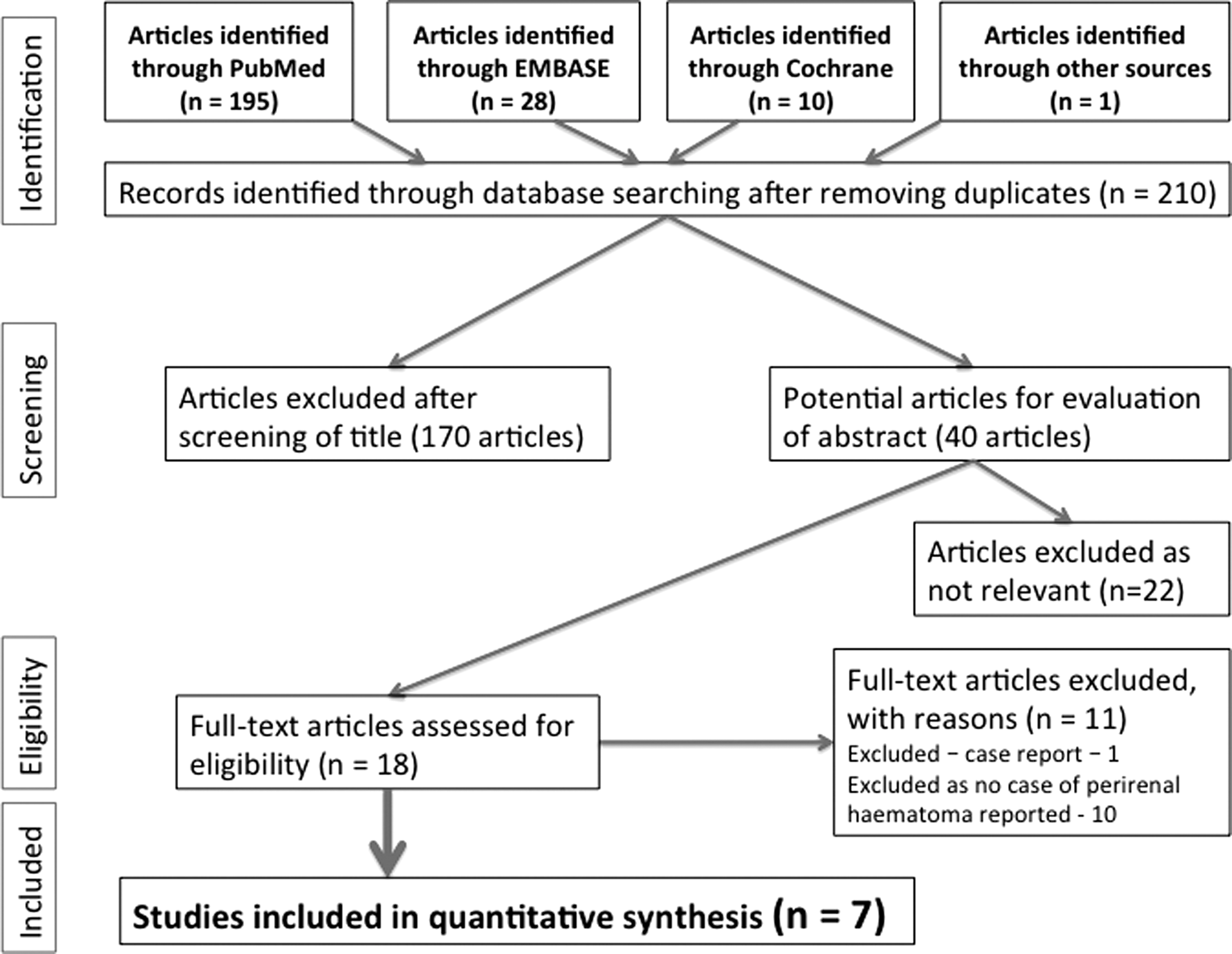
Preferred reporting items for systematic reviews and meta-analyses diagram.
Data extraction
A standardized data extraction form was created and the articles that met the criteria were then analyzed for study type, journal of publication, time period of the study, number of patients, incidence of post-URS PRH, type of URS, predisposing factors, management of the PRH, treatment outcomes, and long-term sequelae.
Results
Our literature search identified 210 articles of potential interest after the removal of duplicates. After screening by abstract and full text, seven articles met the inclusion criteria. All of these articles were full articles. The entirety of this search is detailed in the PRISMA diagram (Fig. 1).
Study design and baseline characteristics
Seven articles identified 8929 patients who underwent URS and of these patients, 40 developed a PRH as a result, with an incidence of 0.45% throughout all studies. The incidence per study ranged from 0.15% to 8.9%. The demographics of the patients who developed PRH were found to be 56.8% female, with an mean age of 53 years and a mean stone size of 1.7 cm. Table 1 shows the summary of all studies that identified PRH after URS. 5 –11 All of the articles reported on patients with kidney stone disease, who were treated with URS and laser lithotripsy, with the exception of Ilic, who compared the effects of laser lithotripsy with those treated with pneumatic lithotripsy as a cohort study. 7 Of the seven studies included, five were retrospective case series, one was a retrospective cohort study, and one was a prospective case series, with data analyzed retrospectively.
PRH = perirenal hematoma.
Most patients with PRH were identified due to fever and loin pain, although there was an exception of one patient who was discovered 1 month later due to nausea, weight loss, and abdominal pain. 9 The method of confirming the presence of PRH was with ultrasound and/or CT scanning. The ureteroscope size varied among studies from 6.5 to 9.8F. The placement of postoperative JJ stent was at the discretion of the surgeon, the majority were left for 4–6 weeks with the exception of pediatric cases.
Predisposing factors
Each of the seven articles identified its own risk factors for the development of PRH. Included in Table 2 are those that were found to be statistically significant. Ilic was predominantly a cohort study comparing laser against pneumatic lithotripsy and although it identified cases of PRH, the article's main focus lay outside of factors that may have caused them. 7 Their study also contained pediatric cases only and therefore some of the risk factors identified in the other studies are not applicable to this patient group. The recurring themes were as follows: a moderate to severe degree of hydronephrosis, thin renal cortex, prolonged operation duration, hypertension, female gender, and UTIs. Other risk factors were higher perfusion pressures, larger stone size, existing chronic kidney disease (CKD), pre- and postoperative ureteral stent usage, ureteral sheath use, and previous renal operation or SWL. There was conflicting evidence on patients' body mass index (BMI), as Chiu's article found that 75% of their patients who developed PRH were overweight or obese (BMI >25). 6 Kao and Wang, on the other hand, found that patients with a low BMI (<18.5) were more likely to develop PRH as 50% of patients with PRH were underweight, compared to 4.8% in the patients who did not develop a PRH. 8 Stone size and perfusion pressures were frequently recorded or mentioned within the article as being an important factor, however, they were only found to be statistically significant in the article by Bai and colleagues. 5
BMI = body mass index; CKD = chronic kidney disease; NM = not mentioned; UTI = urinary tract infection.
Management of PRH
The majority of the articles concluded that conservative treatment was the best initial management of PRH. Conservative treatment varied among authors; some of the studies used blood transfusion and antibiotic therapy, whereas others classed these separately as seen in Table 3. This review classified blood transfusion as part of conservative management. We found that 55% of PRH (22 patients) were managed conservatively and 27.5% (11 patients) required percutaneous drainage. Surgical intervention was needed in seven (17.5%) patients. Two of these were emergency angiography of which one proceeded to open nephrectomy. Open surgery with clot removal was done in three patients, nephrostomy for severe hydronephrosis in one patient, and surgery to correct malpositioned stent in one patient. There was one mortality reported wherein a patient who had postangiography nephrectomy died of multiple organ failure 2 weeks after the intervention.
Outcome of stone treatment
Two articles commented on stone clearance rates in patients who developed PRH. Chiu and Tao found clearance rates of 25% and 66%, respectively, however residual fragments up to 1 cm were identified. No comments on complexity of the procedure were made. Ilic quoted 79.4% stone clearance rate, but there was no detail as to whether the patients who had developed a PRH were included in this number. 7
Long-term sequelae
The majority of hematomas had resolved on the patient's follow-up CT scan, usually undertaken at 6 months. Full details are included in Table 3. Chiu found that one patient developed a perinephric abscess 3 weeks after open evacuation of the hematoma. 6 The abscess was managed with ultrasound-guided aspiration, and CT imaging at 2 months showed complete resolution. The mortality rate of all patients who developed PRH was 2.5% (one patient). As stated above, there was only one case of mortality in this review subsequent to an open nephrectomy, reported by Kao.
Discussion
Findings of our review
Despite current literature existing on “tips and tricks” of flexible URS, 12 there is still a lack of awareness of PRH after URS among endourologists. Post-URS PRH is an infrequent, but notable and potentially organ- or life-threatening complication, with an average incidence of 0.45%. Regardless of its rarity, we encapsulate the common precipitating factors and recommended management and long-term consequences of this complication, so that endourologists are better equipped in avoiding and/or managing them.
The etiology of PRH formation is speculated in several of these articles and based predominantly on the explanation proposed by Bai and colleagues. 5 Authors suggest that post-URS PRH is formed due to trauma to the pelvicaliceal system either after guidewire insertion 13 or due to increased intrarenal pressures precipitating forniceal rupture. 10,11 The significant findings of our review suggested that predictors of PRH can be split into the following patient factors: preoperative moderate to severe hydronephrosis, thinner renal cortex, larger stone size, and presence of UTIs and hypertension; and procedural factors including prolonged operative time and higher perfusion pressures.
Hydronephrosis was quoted by four of the seven articles as predisposing patients to PRH. Bai and colleagues suggested that this could be attributed to hydronephrotic kidneys having higher intrarenal pressures, which can deform or compress major vessels. 5 After URS, ureteral obstruction is relieved, which induces recanalization of weakened vessels causing their rupture. Thus, blood and fluid can accumulate in the subcapsular space of the kidney, separating the capsule from parenchyma, resulting in hematoma formation. 5 Meng and colleagues added that hydronephrosis makes a kidney prone to hemorrhage as its elastic tissue has been damaged. 10 We recommend that extra caution is taken in these patients, knowing their propensity to PRH, through measures such as strict monitoring of the guidewire tip and using the As Low As Reasonably Achievable (ALARA) principle for maintaining intrarenal pressure. 14
Historically, larger renal calculi (greater than 2 cm) were managed by PCNL or open surgery, but advances in technology have allowed URS to progress into a therapeutic tool in this patient cohort too. 15 Patients who formed PRH were found to have a larger stone size compared to the unaffected patients, with a mean stone size of 1.7 cm in patients suffering from PRH. Larger stones would increase the operative duration and hence subject the kidneys to longer duration of elevated intrarenal pressures, potentially increasing the risk of PRH.
UTIs can lead to PRH. This is suggested by two articles in this review and supported by a further case report, where a UTI had a detrimental effect on the patient. The authors advocated early treatment of infection to minimize the inflammatory effect on renal parenchyma, reducing its potential to hemorrhage. 16 The proposed mechanism suggested by the literature is that UTIs can cause damage to renal parenchyma by infiltration of neutrophils into the tissue, making it more inclined to bleed. 8 Therefore, all patients should undergo preoperative urine analysis and treatment of any active urinary infection. Antibiotic usage at induction of the procedure potentially helps to minimize this risk and the associated morbidity of urosepsis.
Two articles suggested that hypertension is another factor which carries an increased risk of PRH. 9,10 Hypertensive patients may be more prone to bleeding after a URS-induced injury, and those with nephropathy may be more predisposed to a renal injury. 9 This is reinforced by a recent large study of nearly 11,000 procedures on 6177 patients. The authors evaluated the risk factors of PRH after SWL and showed a hematoma rate of 0.3% (20 patients). Half of these patients had a history of hypertension and their most common predisposing factors for PRH in the study were hypertension, high BMI, and a large stone size. 17 We recommend that blood pressure is both monitored and treated both pre- and intraoperatively in an effort to decrease hemorrhage.
Conflicting evidence exists regarding the relationship between PRH and BMI. Kao found that 50% of their patients who formed a PRH were classed as underweight. 8 They assumed that patients with a low BMI had less perinephric fat and therefore were unable to cope with high renal pressures as this fat provides a “cushion” against injuries to the kidney and helps to prevent overstretching of the cortex. 8 Conversely, Chiu stated that patients with a higher BMI are more at risk of PRH, as they pose a greater technical challenge to the surgeon in both guidewire placement and scope advancement. 6 A recent review on URS in obese showed a good safety record in these patients, which contradicts Chiu's theory. 18 The review showed that only 11.4% of obese patients had a minor complication after URS, including fever, pain, sepsis, and ureteral perforation, and no major complications were encountered. 18 Only these two articles mention BMI as a predisposing factor to forming PRH and no consensus has been reached. However, it is likely that BMI may not play a big role in PRH, given a systematic review has proved that URS is safe in obesity.
CKD was suggested by one of the articles as predisposing patients to PRH as affected patients' kidneys could be structurally weaker than those in their healthy counterparts, hence easily damaged. 8 CKD is known to be associated with anemia, thrombocytopenia, and impaired platelet function, thus affected patients are more likely to bleed after intervention. Yuruk and colleagues studied CKD patients who underwent URS and found that although these patients have higher number of comorbidities, there was no significant difference in complications. 19 CKD is potentially a risk factor for post-URS PRH, although so far none of the studies have proven it. 20
Other factors listed in Table 2 are not explored in this study as they were observed in a low number of patients and there may be an element of patient cohort bias.
Recommendations for management and long-term sequelae
Post-URS PRH should be given the appropriate attention as a complication advise for serial monitoring of blood pressure and serum determination of renal function. 21 All patients in this review had a similar presentation of flank pain, fever, or a drop in their hemoglobin, and the hematoma was diagnosed by a subsequent ultrasound or CT imaging. Patients who showed signs of hemodynamic compromise proceeded to either percutaneous drainage or open surgery, but the rates were low at 27.5% and 12.5%, respectively. However, the overwhelming agreement is that PRH warrants a prompt diagnosis and in more than half of the cases, a conservative approach with blood transfusion and monitoring would suffice, with further intervention in selected cases. As highlighted by the learning points in Table 4, there are measures that can reduce their incidence and by limiting these risks, the likelihood of occurrence can be minimized. Except for one mortality, all patients in this review showed complete resolution of their PRH. There were no other long-term sequelae reported in any of the other studies.
URS = ureteroscopy.
Learning points
Each of the articles, except Ilic and colleagues, had learning points that could be applied by urologists to either reduce the occurrence of PRH in practice or recommended a management strategy in case PRH was encountered (Table 4). An overall summary of strategies to avoid PRH includes controlling blood pressure, treating UTIs, maintaining a low intrarenal pressure, and reducing operative duration. In patients who form PRH despite these measures, conservative management may be recommended in most cases, with surgical intervention in a selected group of unstable patients. The current European (EAU) and American (AUA) guidelines recommend antimicrobial prophylaxis before URS, use of a safety wire, and laser lithotripsy for stone fragmentation of renal stones. 2,22
Limitations of this review and future research
This review is limited by the quality of the articles included, with the majority of studies being retrospective case series. Although from the reported studies, post-URS PRH is 0.45%, the largest study on URS complications, to date, with nearly 12,000 patients does not mention PRH as a complication, raising uncertainty with possible overreporting of this condition. 3 As each study was performed in a different unit across the world, there was no standardization of the data collected or reporting process. For example, some studies lack information on stone size or irrigation pressure as they were not routinely measured in their hospital, and these data were unavailable for our analysis. An important data set that should be collated in all studies is the patient's coagulation status. SWL and PCNL are relative contraindications in patients with coagulopathy or who are anticoagulated, making URS the only suitable treatment modality available. 23 Of the articles included in this review, four of the seven did not include any data on patients' coagulation status.
Conclusions
We suggest that endourologists performing URS should be aware of the risk factors for PRH. Preoperative treatment of UTI, management of hypertension and adjuncts that reduce intrarenal pressure, and decreased operative duration should be encouraged. In patients who develop PRH, the current evidence advocates its conservative management. Urologists can use these findings to adapt their practice and adequately counsel their patients about this rare, but potentially life-threatening complication.
Footnotes
Author Disclosure Statement
No competing financial interests exist.