
Abstract
Objective:
To assess the efficacy and safety of tadalafil in facilitating the spontaneous passage of distal ureteral stones.
Methods:
The relevant studies were identified by searching MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials up to November 2016. Randomized controlled trials evaluating effects of tadalafil for distal ureteral stones were included.
Results:
Six publications involving 921 patients were included. Compared with tamsulosin monotherapy, tadalafil monotherapy or combined with tamsulosin has a significantly higher stone expulsion rate (relative risk [RR], 1.16; 95% confidence interval [CI], 1.05 to 1.29; p = 0.004; RR, 1.24; 95% CI, 1.09 to 1.42; p = 0.001, respectively) and shorter time to stone expulsion (mean difference [MD], −1.33 days; 95% CI, −2.44 to −0.23; p = 0.02; MD, −1.98 days; 95% CI, −3.08 to −0.88; p = 0.0004, respectively). Statistically significant differences were noted in pain episodes and analgesic use in favor of group tadalafil alone compared to group tamsulosin alone. The analgesic use was significantly lower in the combined group than in the tamsulosin alone group. Although the occurrence of drug-related adverse events in the tadalafil alone or combined with tamsulosin was higher than that in the use of tamsulosin-alone group, the most common adverse events were mild and tolerable.
Conclusions:
Our study suggested that medical expulsive therapy for the distal ureteral stones using tadalafil alone or combined with tamsulosin is safe, efficacious, and well tolerated.
Introduction
U
Previous high-quality meta-analyses showed a statistically significant benefit for both tamsulosin and nifedipine over controls for the outcome of spontaneous stone passage. 3,4 Recently, a large multicenter randomized controlled trial (RCT) found that neither tamsulosin nor nifedipine showed any clinically useful benefit for promoting stone passage measured by the absence of need for further intervention in 4 weeks for patients with ureteral colic. 5 Therefore, the benefits of MET seem unclear with such conflicting data.
Previous studies have identified nitrergic fibers in the distal ureter and demonstrated a relaxant effect of nitric oxide pathway on ureteral smooth muscle. 6,7 Since then, investigators focus on how treatment of the nitric oxide pathway can be effectively implemented in clinical practice until phosphodiesterase-5 inhibitors (PDE5Is) emerged. Tadalafil, a PDE5I, acts on the nitric oxide-mediated pathway of smooth muscles and maybe can induce ureteric relaxation. Recently, several investigators 8,9 have assessed the effect of PDE5Is on spontaneous stone passage in patients with expectantly managed ureteral stones. The results of these studies showed a positive benefit with PDE5Is.
Despite the growing number of published trials with a few patients focused on tadalafil facilitates the ureteral stone expulsion, to our knowledge, a quantitative systematic review of RCTs is lacking to date. Therefore, we performed the first meta-analysis including the most recent evidence to assess the efficacy of tadalafil in patients with ureteral stones.
Methods
This study was performed according to the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement.
Literature search and data sources
We searched the literatures through MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials up to November 2016, with the terms tadalafil, ureteral stone, and RCTs (multiple synonyms for each term). The reference lists from the retrieved documents were also searched. Two authors independently screened all citations and abstracts selected by the search strategy to identify potentially eligible studies.
Inclusion and exclusion criteria
Relevant studies were required to meet the following inclusion criteria: prospective RCTs in humans, evaluate the efficacy and safety of tadalafil for the management of distal ureteral stones, and provide sufficient data for analysis. The primary outcome variables were stone expulsion rate and time to stone passage during treatment period. Secondary variables included the number of pain episodes during follow-up, analgesic use, and adverse effects. We excluded the articles as follows: (1) articles not in English; (2) review or meta-analysis articles; (3) duplicated or updated data; and (4) comments, editorials, letters, and case reports.
Data extraction and quality assessment
Data were independently extracted from the included studies by two authors. The data extracted included the data source, eligibility, methods, participant characteristics, interventions, and results. Any discrepancies among the extracted data were resolved by discussion. The Jadad scoring system 10 was used to assess the quality of the RCTs.
Statistical analysis
The meta-analysis was performed by the Review Manager, version 5.3. Continuous outcomes are presented as a mean difference (MD) with 95% confidence interval (CI). Dichotomous data are presented as relative risk (RR) with 95% CI. Statistical heterogeneity among trials was evaluated using the I2 test, with significance set at p < 0.05. Pooled estimates were calculated with the fixed-effect model if no significant heterogeneity was detected (I2 ≤ 50%); otherwise, the random-effect model was used. For all statistical analyses, a two-sided value of p < 0.05 was considered statistically significant.
Results
Description of the included studies
The study selection procedure is described in Supplementary Figure S1 (Supplementary Data are available online at
Tadalafil vs tamsulosin
Stone expulsion rate and time to stone passage
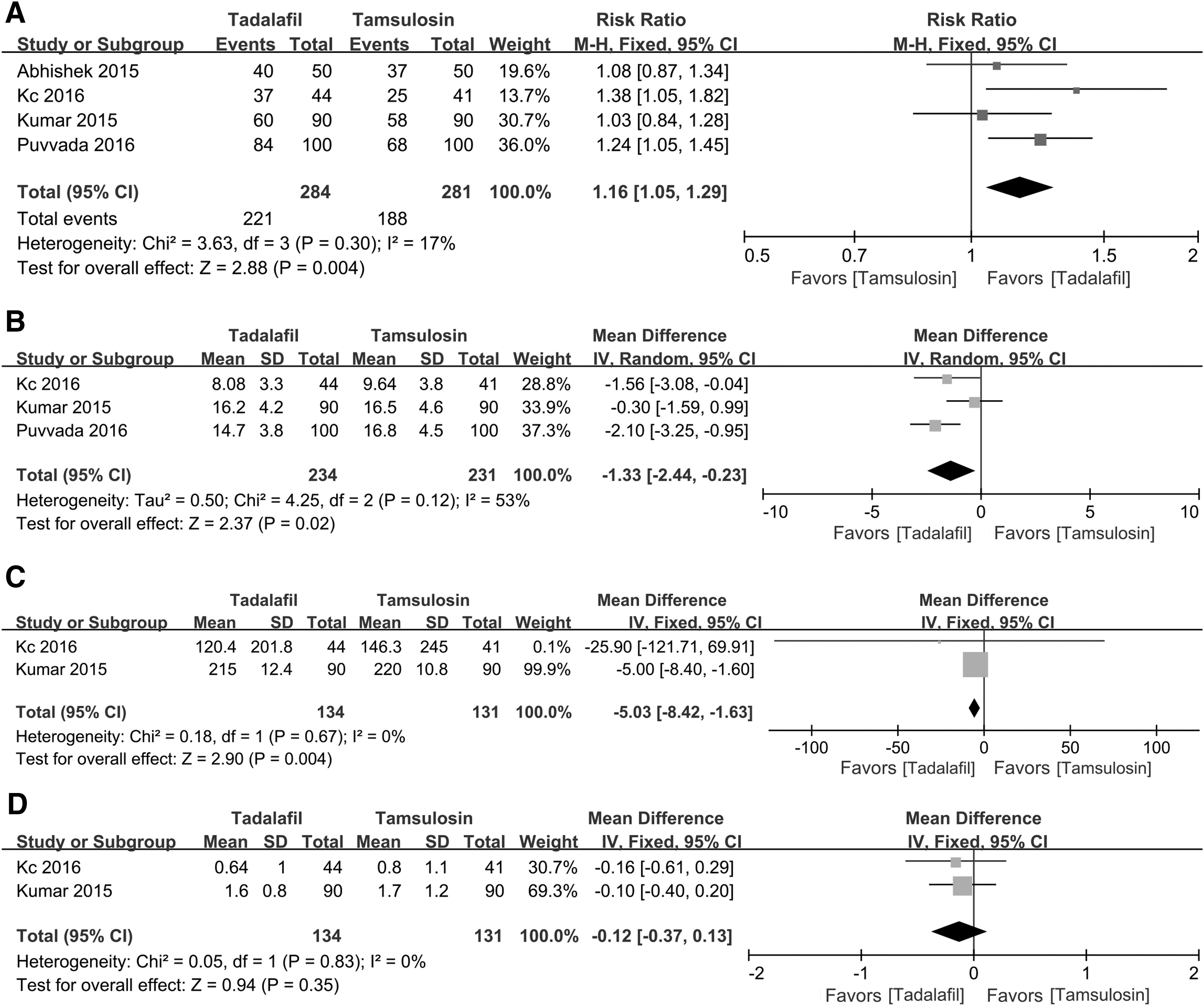
Four 8,11,13,15 of the RCTs were selected evaluating tadalafil vs tamsulosin for lower ureteral stones. Our pooled analysis showed that treatment with tadalafil significantly improves stone expulsion rate when compared to tamsulosin in the fixed-effect model (Fig. 1A) (Table 2). The result was not affected by using the random-effect model (RR, 1.17; 95% CI, 1.04 to 1.31; p = 0.008)
Tadalafil vs tamsulosin:
Bold values are statistically significant.
CI = confidence interval; MD = mean difference; RR = relative risk.
Three studies 8,13,15 were quantitatively analyzed for the stone expulsion time as the outcome. Our pooled analysis showed that the stone expulsion time was significantly shorter in the tadalafil group than in the tamsulosin group in the random-effect model (Fig. 1B). The result was not affected by using the fixed-effect model (MD, −1.36; 95% CI, −2.11 to −0.61; p = 0.004).
Analgesic use and pain episodes
Although four studies 8,11,13,15 reported the analgesic use during treatment, some studies could not be used for meta-analysis as it was given without a standard deviation and different measure unit from others. Therefore, meta-analysis of the remaining two studies 8,13 revealed that compared with tamsulosin, the analgesic use was significantly lower in the tadalafil group (Fig. 1C). The result was not affected by using the random-effect model. Three studies 8,13,15 reported the number of pain episodes during follow-up. Meta-analysis of two studies 8,13 revealed no statistically significant difference between tadalafil and tamsulosin, and there was no evidence of statistical heterogeneity between studies (Fig. 1D). The result was not affected by using the random-effect model. The later inclusion of the study by Puvvada and colleagues 15 as a sensitivity analysis did not affect the results; however, it introduced significant heterogeneity into the analysis (I2 = 89%, p = 0.83), which may result from differences in inclusion criteria.
Safety
Three studies 8,13,15 compared adverse effects between tadalafil and tamsulosin groups. Although our pooled results of three studies showed that the number of headache, dizziness, backache, and orthostatic hypotension of patients in the tadalafil group was higher than the tamsulosin group, no statistically significant difference appeared in these terms (Fig. 2). Meta-analysis of two studies 8,15 revealed no statistically significant difference between tadalafil and tamsulosin for the incidence of abnormal ejaculation (Fig. 2). All the results about the incidence of adverse events were not affected by using the random-effect model.

Pooled estimate of drug-related adverse effects between tadalafil and tamsulosin.
Tadalafil plus tamsulosin vs tamsulosin
Efficacy
Two 12,14 of the RCTs evaluated tadalafil plus tamsulosin vs tamsulosin alone for lower ureteral stones (Table 2). Our pooled analysis showed that treatment with tadalafil plus tamsulosin significantly improves the stone expulsion rate when compared to tamsulosin alone in patients with lower ureteral stones in the fixed-effect model (Fig. 3A). The result was not affected by using the random-effect model (RR, 1.24; 95% CI, 1.09 to 1.41; p = 0.001). The stone expulsion time was significantly shorter in the combined group than in the tamsulosin-alone group (Fig. 3B). The result was not affected by using the random-effect model (MD, −2.00; 95% CI, −3.14 to −0.85; p = 0.0007). The analgesic use was significantly lower in the combined group than in the tamsulosin-alone group (Fig. 3C). The result was also not affected by using the random-effect model.

Tadalafil plus tamsulosin vs tamsulosin alone:
Safety
Adverse effects seem to be more common with tadalafil plus tamsulosin than tamsulosin alone, which included headache, dizziness, backache, and orthostatic hypotension. There was no statistically significant difference between the two groups for the incidence of abnormal ejaculation (Fig. 3D). All the results about the incidence of adverse events were not affected by using the random-effect model.
Sensitivity analyses
Sensitivity analyses were conducted to determine the effect of each study on the pooled analysis and no substantial changes occurred for the corresponding RRs or MDs.
Discussion
Economic burden for stone disease has rapidly increased over the years and most patients with ureteral colic need medical care. Spontaneous passage will occur in most of these stones, associated with stone size and location. This evidence indicates that a potential benefit of MET is most likely for distal ureteral stones >5 mm. 1 The present meta-analysis is the first to evaluate the efficacy and safety of tadalafil as MET for distal ureteral calculi. The main findings are that the use of tadalafil alone or combined with tamsulosin in patients with ureteral stones results in a higher stone expulsion rate and a shorter time to stone expulsion. Also, the use of tadalafil alone or combined with tamsulosin slightly reduces the need for analgesic medication. Adverse effects were more present in the tadalafil group, however, mostly mild to moderate and did not lead to cessation of therapy.
Spontaneous passage chance of distal ureteral stones sized 5–10 mm is 53%. 16 Faster stone expulsion will decrease the rate of complications, the need for invasive interventions, and eventually decrease healthcare costs. A recent study 16 evaluated the efficacy of sexual intercourse in the expulsion of distal ureteral stones (5–10 mm) and found that sexual intercourse 3–4 times/week for married male patients with distal ureteral stone leads to an increase in the expulsion rate. This effect is assumed to be associated with nitric oxide released during sexual intercourse, which will be able to induce ureteral relaxation. As we know, tadalafil acts on the nitric oxide-mediated pathway of smooth muscles. A previous study 17 demonstrated the role of phosphodiesterase inhibitors in relaxation of ureteral muscles in the sequence vardanafil > sildenafil > tadalafil. Basis on the aforementioned, recently, Kumar and colleagues 8 conducted an RCT to evaluate the potential role of tadalafil in comparison with tamsulosin in ureteral stone expulsion. They found that tadalafil has shown a high ureteral stone expulsion rate and significant pain control. The results are consistent with our meta-analysis. In addition, pooled data analysis of our study showed that the combined use of tadalafil and tamsulosin results in additive favorable effects for ureteral stones compared with tamsulosin monotherapy.
PDE5Is are the first-line medication for erectile dysfunction. Hence, the prescription of tadalafil in cases of lower ureteral stones with erectile dysfunction may provide an additional advantage in the erectile function. Kc and colleagues 13 reported that 75% patients felt a mild degree of penile tumescence after the intake of tadalafil lasting for 20–30 minutes and no patients developed priapism. Kumar and colleagues 14 found that 12.9% of patients in the tadalafil plus tamsulosin group experienced improvement compared with the tamsulosin-alone group. Therefore, tadalafil is an alternative proposal for patients of lower ureteral stones with erectile dysfunction.
Although tadalafil may induce many adverse events for erectile dysfunction, compared with other PDE5Is, tadalafil 10 mg had the lowest overall rate of all adverse events. 18 Tadalafil has also been approved for treatment of lower urinary tract symptoms from benign prostatic enlargement on the account of it being safe and well tolerated. 19 Recent studies explored the potential role in distal ureteral stones. Our study shows that headache, dizziness, backache, and orthostatic hypotension were the most commonly reported adverse effects in patients treated with tadalafil, and abnormal ejaculation was the most commonly reported with tamsulosin; however, the differences between the two groups were not significant. In addition, even though the occurrence of drug-related adverse effects in the combination use group was higher (no statistical significance) than that in the use of tamsulosin-alone group, the most common adverse effects were mild and tolerable.
Although this study is the first meta-analysis to examine the effect of tadalafil for distal ureteral stones, several limitations should be clarified. First, although we collected all the eligible studies, only six RCT, the sample size was not large enough; this could increase the likelihood of type I and type II errors. Furthermore, well-designed, double-blinded, placebo-controlled, large-scale, multicentric RCTs are suggested to address the clinical question. Second, positive studies are more likely to be published than negative; these results might have been affected by publication bias. Third, only two studies assessed the combination therapy for ureteral stone. Therefore, future research should investigate whether combination therapy with tadalafil and tamsulosin is efficacious in these patients than monotherapy. Fourth, the absence of description of the allocation concealment in all included trails may result in some undetected bias of this study. Finally, the most included study did not assess the impact of tadalafil on the frequency of sexual intercourse of the study population, which also has a potential role in the distal ureteral stone spontaneous expulsion.
Conclusion
MET for the distal ureteral stones using tadalafil alone or combined with tamsulosin is safe, efficacious, and well tolerated. Because of limited quantity and small sample size of included studies, further well-designed, double-blinded multicentric RCTs are strongly encouraged to address the clinical question.
Footnotes
Acknowledgments
This work was collectively supported by grant from National Natural Science Foundation of China (No. 81270841). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.