
Abstract
Purpose:
When accidental tumor incision (ATI) has occurred during open partial nephrectomy (PN), scissors can be changed easily. In contrast, during laparoscopic partial nephrectomy (LPN) or robotic partial nephrectomy (RPN), it is time consuming and expensive especially during RPN to change scissors. This study investigates whether tumor cells remain on the surface of scissors after ATI during PN and investigates an alternative way to avoid changing scissors during LPN and RPN.
Materials and Methods:
We subcutaneously injected 786-O renal-cell carcinoma (RCC) cells containing enhanced green fluorescent protein (786-O/EGFP) into six mice. We incised the subsequent tumor with straight or Microline scissors. The scissor surfaces were then examined by microscopy for detection of EGFP immunofluorescence. In addition, the scissor surfaces were treated in three ways: no electrical treatment, electrical treatment of 20 W for 5 seconds, and electrical treatment of 40 W for 5 seconds.
Results:
Strings or dots of EGFP were detected on every scissor surface, and 786-O/EGFP cells were alive and able to proliferate in medium in 33% of the nonelectrically treated samples. However, no 786-O/EGFP cells treated with monopolar electricity survived. In another experiment, we also found that 100 786-O cells placed on scissor surfaces could not survive after the same electrical treatment.
Conclusions:
RCC cells remained on scissors after ATI; however, electrical treatment eliminated tumor cells, possibly preventing recurrence or metastasis after surgery.
Introduction
S
Complete resection of cancer without spillage is an oncologic principle. Previous studies have suggested that avoidance of tumor violation or traumatic manipulation is important to prevent tumor seeding and metastasis. 14 However, we occasionally encounter cases of accidental tumor incision (ATI), especially when a cancer is present inside the kidney like an intraparenchymal tumor or endophytic tumor. In addition, most surgeons expand the surgical margin into normal tissue without changing scissors after ATI during LPN and RPN because it is time consuming and expensive especially during RPN to change scissors, even though it is unknown whether tumor cells remain on the scissor surface.
A characteristic of RCC is metastasis or recurrence even long after surgery, 15,16 but this seems difficult to associate with a PSM or ATI. Thus, we aimed to determine whether RCC cells remain on scissors after ATI by using mouse experiments. In this study, we utilized 786-O RCC cells containing enhanced green fluorescent protein (786-O/EGFP) to distinguish between RCC and normal cells. Using this cell line, we created tumors in mice, incised the tumors with scissors to mimic a surgical procedure, and then determined whether cells remained on scissor surfaces. We also determined whether remaining cells could proliferate in cell culture medium. In addition, we treated scissors with electricity to determine effectiveness for eliminating cells on scissor surfaces. To our knowledge, this is the first experimental study to evaluate tumor cells on instruments during oncologic surgery after ATI and to assess the use of electricity for cell elimination.
Materials and Methods
Cell line
786-O/EGFP cells were kindly provided by Dr. A.T. Sasaki (University of Cincinnati, Cincinnati, OH). 786-O cells were derived from a primary clear cell RCC. This cell line was incubated in RPMI 1640 medium (Invitrogen, Carlsbad, CA) supplemented with 10% fetal bovine serum and maintained in humidified incubators (5% CO2) at 37°C.
In vivo tumor xenograft model
To confirm whether RCC cells remained on scissor surfaces, 100 μL sample containing 4 × 106 (786-O/EGFP) cells and 100 μL Matrigel Matrix (Corning, Bedford, MA) mixture were injected subcutaneously into the right flanks of six female nude mice (BALB/c nu/nu, 6–8 weeks old). The mice were anesthetized 21 days after inoculation, and the skin was incised and tumors were exposed. Then, ∼5 mm tumor incision was done once, and scissor surfaces were examined (Fig. 1). Sterilized normal straight scissors and Microline scissors (Microline Surgical, Beverly, MA) were used for incising the tumors, because straight scissors were flat and easy to photograph, and because Microline scissors are often used in operations. All animal experiments were performed in accordance with institutional guidelines and were approved by the animal care review board of Kagoshima University.
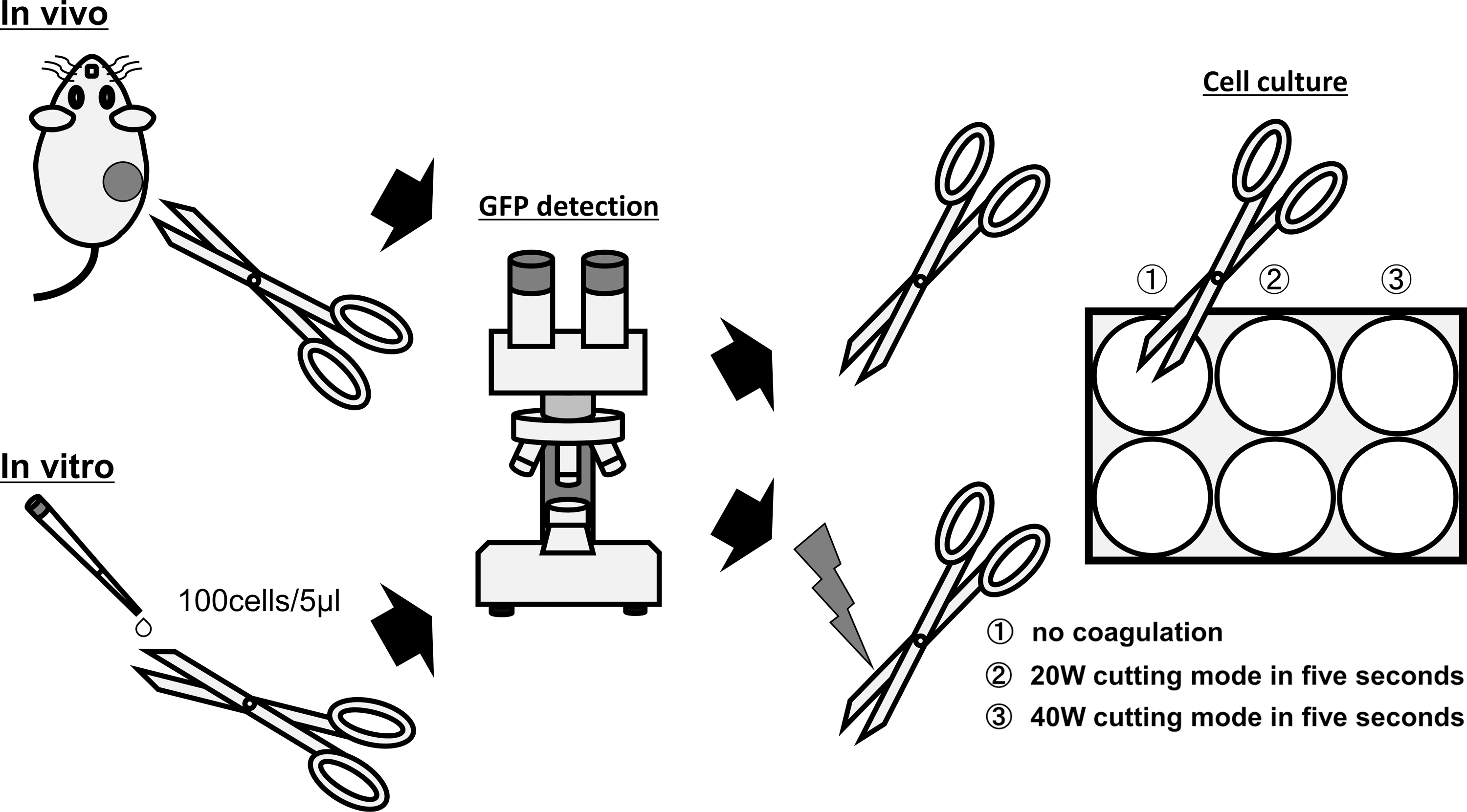
Schema of in vivo and in vitro experiments.
Identification of RCC cells on scissors
EGFP-positive cells were identified and photographed under a Keyence fluorescence microscope (Keyence Corporation, Osaka, Japan). We applied the same exposure time in each experiment and took multicolor photographs to obtain simultaneous bright-field and green immunofluorescence images: 1/6 second for bright-field and 1/3 second for green immunofluorescence images. In these exposure times, we confirmed no background was observed before starting experiments. Then, scissors were treated in three ways: no electrical treatment, electrical treatment of 20 W for 5 seconds, and electrical treatment of 40 W for 5 seconds, using a monopolar device. Scissors were dipped into the medium and shaken several times to shed cells onto a six-well plate (Fig. 1).
In vitro experiments
To determine whether electrical treatment was effective in destroying RCC cells, we performed similar experiments with a fixed number of 786-O cells. First, 100 786-O cells were placed onto scissor surfaces, and the scissors were closed once. Then, the scissors were treated in three ways according to the protocol of the in vivo procedure. Ten days later, cells were observed by microscopy and stained with 0.04% crystal violet (Nacalai Tesque, Kyoto, Japan) (Fig. 1). Experiments were performed in sextuplicate.
Results
In vivo experiments
Figure 1 describes the in vivo experiment. First, we examined the scissor surface and set the exposure time to filter out green. After incision of tumor was done once, using straight or Microline scissors, we examined the scissor surfaces. In this experiment, we used six mice: three were incised with straight scissors and three with Microline scissors. Fluorescence microscopy showed that every scissor surface had strings of green color caused by squeezing cells between the blades and green-colored dots showing 786-O/EGFP (Fig. 2A, B). After culturing, 33% of wells exposed to straight or Microline scissors that were not electrically treated showed proliferation of 786-O/EGFP cells (Fig. 3A), whereas no cells were observed in all 12 plates in which electrically treated scissors were dipped.
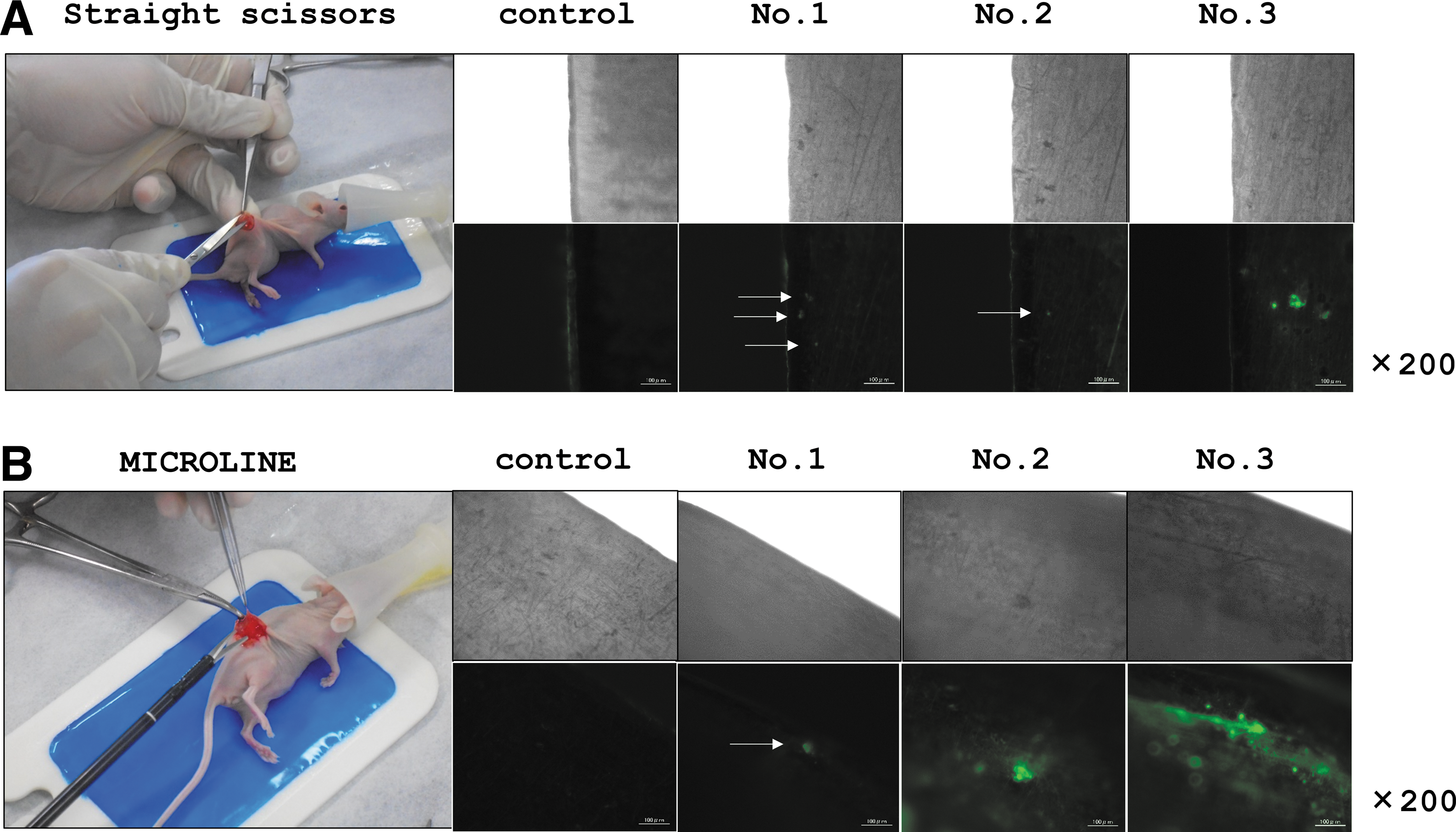
Representative images of mouse experiments and scissor surfaces by using bright-field (upper) and green immunofluorescence (lower) multicolor images.
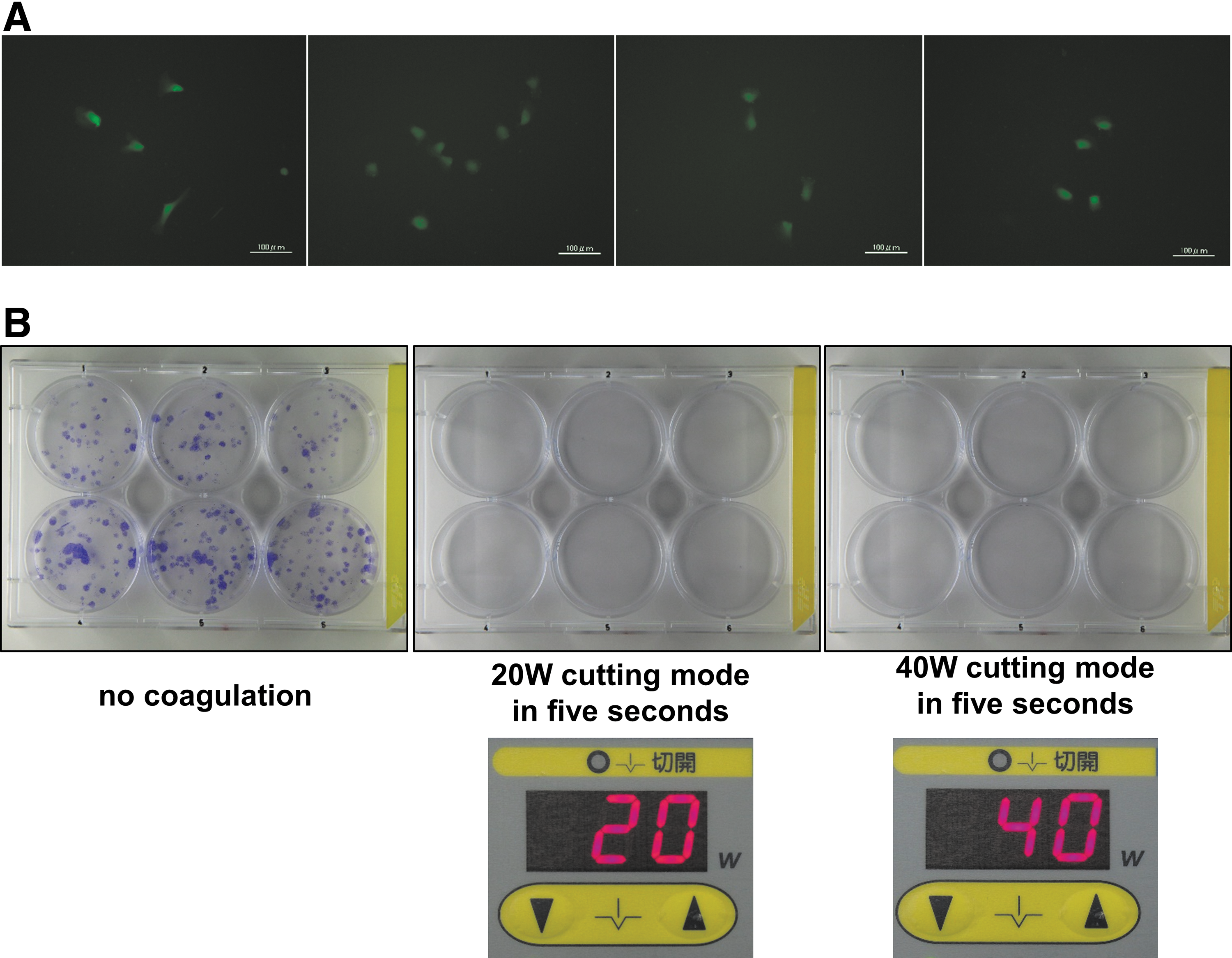
In vitro experiments
We also performed similar in vitro experiments by using a fixed number of 100 786-O cells. After placing cells on scissor surfaces, proliferation was observed in all six wells exposed to scissors that were not electrically treated (Fig. 3B, left). However, no cells were observed or proliferated in all six wells in which electrically treated scissors were dipped (Fig. 3B, middle and right). Photographs of the experimental setup in a monopolar device are also shown in Figure 3B.
Discussion
Recently, PN has been adapted for use in T1b renal masses, an upgrade from the use in T1a masses. 17 In addition, some reports have shown that PN for renal masses ≥7 cm has acceptable oncologic, technical, and functional outcomes. 18,19 Therefore, PN for larger tumors and those with central localization is likely to become even more widely accepted. It is assumed that more surgeons will encounter a PSM or ATI as the use of PN increases. However, whether a PSM increases the incidence of metastasis or recurrence remains controversial, as contradictory results have been reported. 8 –13 Recently, Ito et al. reported the effect of ATI during LPN on oncologic and clinical outcomes. 20 In that study, ATI was influenced by the presence of a pseudocapsule and, to some degree, by tumor size, but was not associated with negative oncologic outcomes such as tumor recurrence or a PSM. Interestingly, local recurrence and PSM occurred more often in cases without ATI. However, their study included a small number of patients and relatively short median follow-up (<3 years), and they did not discuss how they managed instruments after ATI.
The incidence of port site metastasis, tumor seeding, and local recurrence after laparoscopic urologic surgery has been estimated as low, especially in RCC. 21 However, when recurrence or metastasis occurs, there is no curative treatment for RCC. In addition, basic research suggests that tumor dissemination is inevitable once tumor cell spillage occurs, even though in vivo experiments indicate that dissemination can be reduced or delayed with water or antiseptic lavage. 22,23 In addition, the presence of disseminated single tumor cells detected by real-time quantitative polymerase chain reaction in peritoneal lavage fluid during surgery was associated with a high recurrence rate and poor overall survival in colon cancer patients compared with patients without dissemination. 24 Therefore, complete resection of cancer without spillage is a major oncologic principle. However, we occasionally experience ATI during an operation or a PSM after receiving the pathology report. Even though several studies have tried to elucidate a correlation between PSM and metastasis or recurrence, there has been no report about whether tumor cells can remain on an instrument after ATI or with a PSM. We identified tumor cells on scissors after ATI and tried to destroy the cells on the scissor surfaces using electricity; we found that no cells survived electrical treatment. During LPN or RPN, small gauze pads are always prepared in the operative field; therefore, when ATI or a PSM is encountered, it is easy to apply electricity to scissors for 5 seconds to destroy tumor cells by using a small, moistened gauze pad and a monopolar device. If bipolar scissors are used, the same efficacy can be obtained by setting scissors on current, because cells will be destroyed by heat. If these procedures are difficult to perform during an operation, the scissors have to be exchanged.
Our study is not without drawback. First, the experimental sample size was small. Second, we used only 786-O clear cell RCC cell line, even though RCC is usually heterogeneous mass of several cell population, and we do not know which type of cells can contribute to tumor recurrence after surgical intervention. 25 Finally, this experiment does not show the development of metastasis in animals. However, as we mentioned previously, metastasis or recurrence of RCC could develop a long time after surgery. 15,16 In these perspectives, our study suggested that instrument contamination of tumor cells may contribute to develop tumor recurrence and metastasis.
In this article, we found the effectiveness of electricity application after ATI or PSM through in vitro and in vivo experiments, but did not demonstrate its effectiveness in patients. Therefore, clinical validation will be necessary in the next stage.
Conclusions
Our data suggested that tumor cells can remain on scissor surfaces after ATI and can proliferate in medium. To the best of our knowledge, this is the first report of cell persistence on scissor surfaces after the occurrence of ATI. Moreover, electrical treatment of scissors can eliminate tumor cells, thus possibly preventing metastasis or recurrence. This is an easy but powerful technique for use by surgeons in the event of ATI, not only during PN but also during other operations.
Footnotes
Acknowledgments
This study was supported by JSPS KAKENHI (C) Grant number 16K11015. 786-O RCC cell having EGFP cells was kindly given by Dr. A.T. Sasaki. We thank Kei Ono for the great help of preparing Microline scissors.
Author Disclosure Statement
No competing financial interests exist.