
Abstract
Purpose:
Minimally invasive surgery is in constant further development and has replaced many conventional operative procedures. If vascular structure movement could be detected during these procedures, it could reduce the risk of vascular injury and conversion to open surgery. The recently proposed motion-amplifying algorithm, Eulerian Video Magnification (EVM), has been shown to substantially enhance minimal object changes in digitally recorded video that is barely perceptible to the human eye. We adapted and examined this technology for use in urological laparoscopy.
Materials and Methods:
Video sequences of routine urological laparoscopic interventions were recorded and further processed using spatial decomposition and filtering algorithms. The freely available EVM algorithm was investigated for its usability in real-time processing. In addition, a new image processing technology, the CRS iimotion Motion Magnification (CRSMM) algorithm, was specifically adjusted for endoscopic requirements, applied, and validated by our working group.
Results:
Using EVM, no significant motion enhancement could be detected without severe impairment of the image resolution, motion, and color presentation. The CRSMM algorithm significantly improved image quality in terms of motion enhancement. In particular, the pulsation of vascular structures could be displayed more accurately than in EVM.
Conclusions:
Motion magnification image processing technology has the potential for clinical importance as a video optimizing modality in endoscopic and laparoscopic surgery. Barely detectable (micro)movements can be visualized using this noninvasive marker-free method. Despite these optimistic results, the technology requires considerable further technical development and clinical tests.
Introduction
N
Thus, structures located beneath the visualized surface (such as blood vessels) cannot be identified manually. 6 The improvement of these limiting conditions is being investigated intensively and addressed by many working groups worldwide. 7 –10
Our research focuses on technological validation of the open-source software Eulerian Video Magnification (EVM) for its use during endoscopic procedures in urology (e.g., identification of vessel branches during partial and nephrectomy) and to investigate whether the pulsation of vascular structures in the abdominal cavity can be sufficiently enhanced to make them easily identifiable to the surgeon. 11,12 Furthermore, we modified this technology, developing the novel CRS iimotion Motion Magnification (CRSMM) algorithm, which is optimized for applications in laparoscopy.
Materials and Methods
Eulerian Video Magnification
EVM was developed at the Massachusetts Institute of Technology's Computer Science and Artificial Intelligence Laboratory and Quanta Research Cambridge, Inc. 12 Its original intended use was to visualize subtle changes in video images over time, such as color variations or slight movement within videos (e.g., to detect subtle changes in facial expression). Although invisible to the naked eye, these changes manifest in numerical changes in the matrices of the digital image, which can be amplified and visualized. While many uses for this algorithm can be fathomed, such as changes in emotional states within a person's face or the health of a person, the feasibility of this algorithm was first shown through the detection of a person's pulse.
EVM thus tracks the color variation over the whole image over time, providing a temporospatial representation of the video's numerics that can then be filtered and amplified in the temporal dimension (as opposed to spatial image processing such as is used when processing images). A temporal filter is then applied that includes all frequencies that are within a chosen frequency band and suppresses other frequencies. With this method, not only slight color changes, but also very subtle motion can be detected.
The video signal is thus analyzed for intensity changes over time that occur periodically within the specified frequency band. The extracted areas that fluctuate within this band can then be numerically magnified, highlighting those parts of a video that show a certain color fluctuation or movement.
If the video shows, for example, the face of a human, his/her pulse can be calculated. After the fluctuation in numerical value (color change) is detected, the pulse can be determined as follows: If a digital camera captures a video with fC
= 30 frames per second (fps) and detects a maximum in color intensity every NM
= 40 frames, the heart rate fH
must be around 1333 beats per second or 80 beats per minute (bpm).
CRSMM
The CRSMM algorithm, which was developed by CRS iimotion Gesellschaft mit beschränkter Haftung (GmbH), is based on the EVM source code, which has been released free for noncommercial use. It is optimized for endoscopic video imagery to enhance the visibility of vascular structures rather than detecting the pulse. In CRSMM, the frequency band filter of a human pulse (0.4–4 Hz or 24–240 bpm) is applied pixel-wise to the temporal dimension of the video.
Those areas exhibiting strong color fluctuations within the specified frequency band are magnified. The areas that are within the band then appear highlighted and thus are assumed to be vascular structures. With this algorithm, pulsating parts of living tissue can also be made visible.
Algorithm
Let I (x, y, t) be the pixel intensity at coordinates x, y at time t. The EVM algorithm tracks the magnitude of the intensity change due to motion in relation to time (i.e., from one frame to the next). The same method can be applied to colored video images as well.
To detect pulsating tissue, only a certain range of intensity changes over time is relevant, specifically the aforementioned range of 0.4–4 Hz or 24–240 bpm. In CRSMM, the areas in which intensity changes occur inside this frequency range are detected and amplified.
In the experiment prerecorded, 1080p full HD camera resolution videos were analyzed within several minutes using EVM and CRSMM. However, the amount of data in a full HD video signal does not allow real-time processing of the video images without significant computing power. Although, it would be possible to include specialized digital image processing hardware capable of performing such tasks, financial and engineering limitations do not suggest this to be feasible at the current time.
For this reason, the image provided was full HD resolution, but the video was scaled down for processing in real-time. In addition, the frame rate of the enhanced image was not at the full frame rate of 24/30 fps. The video resolution and frame rate of an image enhanced in real-time were at 320 × 240 pixels (or 640 × 480 pixels maximum) with a frame rate of ∼12 fps. We used about 45 minutes of video material from five different urological procedures for algorithm training. These recordings were cut in shorter sequences and utilized accordingly in the software development process. Finally, the processed sequences were evaluated in terms of proper imaging and identifiability of enhanced structures by surgeons experienced in urological laparoscopy (A.M. and M.S.). The doctors were asked to answer a question if the software-based visualization is improved. At this stage of development, we had not performed any comprehensive trials.
Results
Initial testing using EVM showed that the pulsating motions and color fluctuations of living tissue could indeed be visually enhanced and improved so that it becomes visible to the human eye. The first examples displayed the diastolic and systolic states detected through Motion Magnification (Fig. 1).
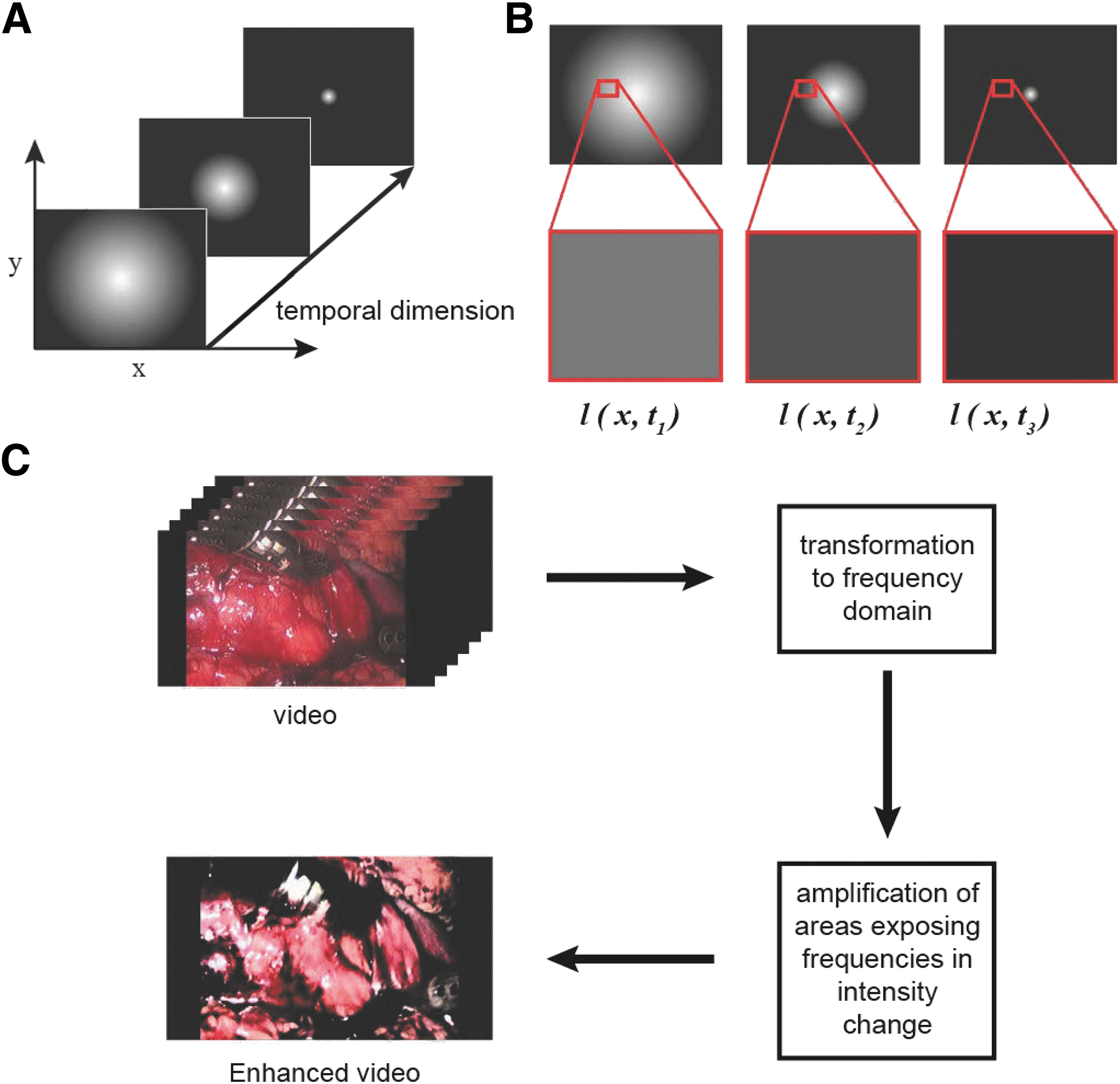
Mathematical background of motion magnification video processing.
Without coupling with a pulse oximeter, the algorithm was not able to give a satisfactory degree of visual enhancement to the vascular structures. This must have been attributed to the fact that, in videos of surgical interventions, motion occurs within the same frequency range as a pulse without being actually caused by a pulse. This could lead to false readings and the amplification of areas within the images that are not vascular structures.
Therefore, CRSMM algorithm adapted to laparoscopy videos was utilized. In this setting, coupling to a pulse oximeter was realized that resulted in significant precision improvement for detecting vascular structures. If the algorithm had reliable data regarding the pulse, the frequency band could have been narrowed down such that tissue movement due to other reasons had not been highlighted.
Figure 2 shows the strongly enhanced visibility of vascular structures when the enhancement algorithm was applied. However, it must be noted that this amplification comes with a significant loss of image quality. In future applications, the option to switch the amplification on or off depending on the situation will be integrated.
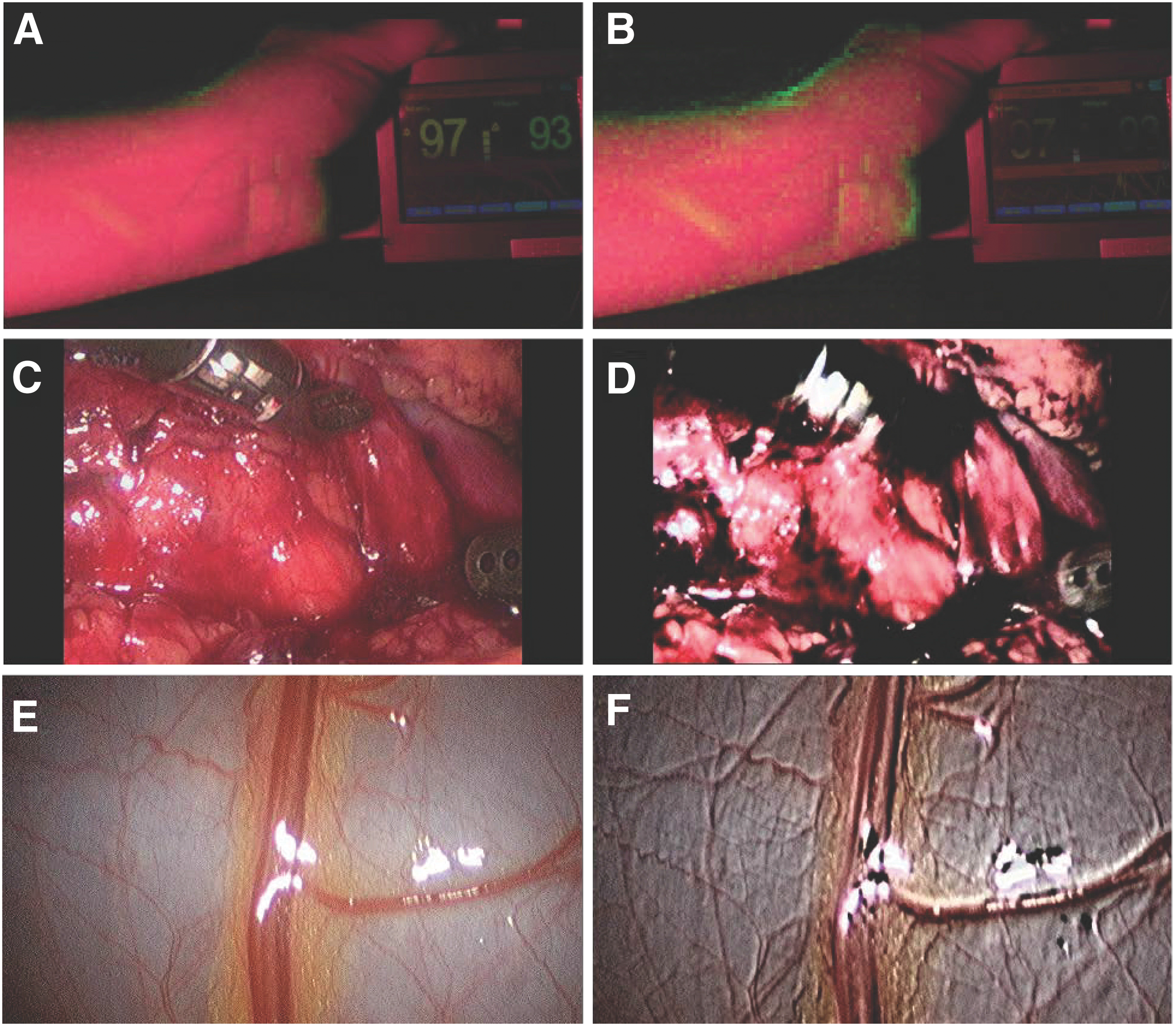
Practical examples of the motion magnification technology.
Discussion
Today, minimally invasive surgical techniques play an important role in operative medicine. Their ascendency started in 1987 with the first successfully performed laparoscopy by Mouret. 13,14 In addition, the Hopkins rod-lens system, the dramatic miniaturization of video cameras has allowed a surgeon to visualize the interior of the human body in a way that was at least equivalent to open surgery. First and foremost, avoiding large wounds has led to less postoperative pain followed by a faster mobilization of the patient with fewer complications like atelectasis or thrombosis that can be caused by immobilization. Ultimately, shorter hospitalization times can result in faster convalescence. In addition, improved cosmetics because of minor surgical scars can be considered as a further positive effect, paradoxically often the most important advantage of the treatment in the patient's perception.
However, laparoscopic surgery can still be potentially hazardous under certain circumstances. The lack of haptic feedback can cause severe restrictions in intraoperative orientation and the identification of relevant anatomic structures. 15
Given these and other points of consideration, the surgeon may be forced to convert to open surgery. The rate of conversion in laparoscopic surgery depends on the particular procedure, and this factor is important for patient counseling. However, the most common indication for conversion in laparoscopy is inadvertent vascular injury and bleeding. A substantial vascular injury is usually difficult to manage in a laparoscopic manner, therefore forcing the surgeon to rapidly terminate the intervention. The absolute number of necessary conversions per year has declined significantly over the last three decades, reaching a low of <1%. Accidental vascular injuries, which account for 38.5% of these conversions, are the main cause. 16 Furthermore, a conversion is frequently associated with serious risk to the patient. Research on technologies for the detection of vascular structures is therefore needed and might possibly minimize that risk.
The new motion magnification technology in humans was first applied in 2009 by Park and Kim. They presented a method for transforming subtle facial expressions into exaggerated movements by using motion magnifying video processing algorithms. 17
The main strength of our study at this point of development lies in the exploration of new possibilities in atraumatic marker-free visualization of vascular structures during laparoscopic surgery. This work should be considered as an example of technology transfer into a new medical application and a feasibility test.
Motion magnification technology has therefore a real potential to be used in the future as a supportive image processing tool in endoscopy/laparoscopy. It can amplify subtle motions in video sequences to visualize structures that would otherwise not be visible. 17 The ability to amplify miniscule movements in real-time and thus visualize them could make small and/or deep unfavorably located vascular structures intraoperatively visible (e.g., under fatty tissue). Such noninvasive and label-free assistance to the surgeon might have the potential to reduce both the risk of intraoperative bleeding and conversion rate as well as significantly decrease operation times. Despite all the optimistic first results, motion magnification technology is not yet mature enough to be reliably utilized in the operation room (OR).
We have developed a new algorithm, based on the freely available EVM software that is adapted for intraoperative endoscopic image processing. However, the presented work has substantial limitations.
First, patient vascular structure pulsation can be highly heterogeneous, considering the target operative field. The organs might be covered partially by blood or blood clots resulting in a strong absorption of the oscillation signal. Furthermore, the constant patient-related pulsation of the vessels can be transferred to the recording video system through simultaneous vibration of the laparoscopy ports. This phenomenon, in combination with trembling caused by the hand of the surgeon holding the camera, generates additional artefacts that have to be extracted while processing the video signal. From this point of consideration, video material recorded for motion magnification editing should be captured in a tremor-free setting. This might be only possible using a special camera-holding system attached, for example, to the operating table. However, these requirements cannot be often guaranteed under sterile conditions in the OR.
Therefore, a patient's heartbeat rate has to be considered for mathematical processing of the video signal and hence included in the algorithm. The complexity of the calculation model thus exponentially increases, resulting in unstable image reproduction conditions, artefacts, and longer processing times. The respiratory rate is another factor that can interfere with the reconstruction process of endoscopic videos. Breathing might also cause organ (micro)movements, in particular, in the upper parts of the abdominal cavity. In urology, retroperitoneal structures are accessed frequently during different treatment modalities. For this reason, the respiratory rate has to be considered when developing video processing modalities suitable for endoscopy.
During the experimental evaluation, several further engineering issues were discovered, which need to be addressed to obtain reliable results, such as a low signal-to-noise ratios, color noise, and low or fluctuating brightness. Additionally, naturally moving tissue and jiggling motions of the instruments can generate false readings. These problems require further development, but we are confident that they can be resolved. There are several possibilities that will be investigated, such as coupling the system to a pulse oximeter to determine a narrower frequency band, utilizing specialized imaging electronics and optics, and providing better lighting technology.
This research focuses on basic questions regarding (micro)movement enhancement in video processing in urologic endoscopy and provides first evidence on this technology in laparoscopy. Both extensive technical development efforts and clinical trials are needed to make this idea suitable for the OR. The clinical relevance of motion magnification in surgery also should be evaluated in the future. Nonetheless, modern algorithm-based video processing methods that operate marker-free have already achieved noticeable results. Further research in this field is therefore needed and will most likely result in novel technical modalities. We conclude that it is technologically feasible to visualize blood vessels in real-time during endoscopic surgery. This kind of digitally enhanced visualization system is expected to further reduce the risk of accidental blood vessel injury, reduce patient recovery time, and improve overall surgical efficiency.
Conclusions
Motion magnification image processing technology has the potential to gain clinical importance as a video optimizing modality in endoscopic and laparoscopic surgery. Movements barely detectable to the human eye can now be visualized using this noninvasive marker-free method. We showed that it is technologically feasible to visualize blood vessels in real-time during endoscopic surgery. In laparoscopy, this might result in reduced bleeding and conversion rates, improving the overall outcome of surgery. Despite optimistic results, the technology requires considerable further technical development and clinical tests.
Footnotes
Acknowledgments
The authors thank the Schoelly Fiberoptic GmbH, Denzlingen, Germany, and CRS iimotion GmbH, Germany, for providing the technical support for this study. Sources of financial support: own institutional funding (Medical Faculty of the University Freiburg) and nonfinancial industrial funding (providing the instruments and technical support for the above study) by Schoelly Fiberoptic GmbH, Denzlingen, Germany. IRB approved protocol number: 282/15 leading ethics committee: Ethik-Kommission der Albert-Ludwigs-Universität Freiburg. German Clinical Trial Register ID: DRKS00009732 (approved WHO primary register).
Authors' Contributions
F.A.: data collection, data management, and article writing/editing. R.S.: article writing/editing and data analysis. D.S.: article writing/editing. M.S.: data analysis and article writing/editing. D.S.S.: article writing. K.W.: data collection, management, and analysis. S.H.: article and figure editing. U.W.: data interpretation and supervision. A.M.: protocol/project development, data collection, data analysis, article writing/editing, and supervision.
Ethical Standards
The study has been approved by the local ethics committee and has therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All experiments were performed according the guidelines of GLP (Good Laboratory Practice).
Author Disclosure Statement
F.A.: no conflicts of interest or financial ties to disclose. R.S.: shareholder of Schoelly Fiberoptic GmbH, Denzlingen, Germany. D.S.: no conflicts of interest or financial ties to disclose. M.S.: consultant contract with Schoelly Fiberoptic GmbH, Denzlingen, Germany, and NeoTract, Inc., Pleasanton, California. D.S.S.: no conflicts of interest or financial ties to disclose. K.W.: no conflicts of interest or financial ties to disclose. S.H.: no conflicts of interest or financial ties to disclose. U.W.: advisory board, DR. KADE Pharmazeutische Fabrik GmbH, Berlin, Germany. A.M.: consultant contract with Schoelly Fiberoptic GmbH, Denzlingen, Germany.