
Abstract
Purpose:
To evaluate the durability differences between five different type of guidewires against laser energy in an in vitro experimental ureteral model.
Methods:
The study was performed at the Department of Urology, Medicine Faculty of Ahi Evran University. An in vitro experimental ureteral model was created for the work; a silicon ureteral model in a saline-filled container. Experiments were performed on five different type of guidewires; ZIPwire, Sensor polytetrafluoroethylene (PTFE) Nitinol guidewire, Roadrunner® PC wire guide, Amplatz Super Stiff, and Zebra Urologic Guidewire. These guidewires were grouped from one to five, respectively. Laser fibers were contacted to the guidewire, and laser energy was fired to the premarked tip and body parts in different adjustments.
Results:
The breakage of the guidewires was detected only on the flexible tip parts in group 1a, group 1b, group 2a, group 2b, group 4a, and group 4b. The body parts of the guidewires were resistant to laser energy in all groups and did not break. The breakage of the guidewires occurred after 3 J × 10 Hz (30 W) experiment. Group 1a and 1b were different from group 2a, 2b, 4a, and 4b according to Kruskal–Wallis H test.
Conclusions:
The body parts of the guidewires in all study groups were resistant to laser energy. The tip parts of Zipwire™, Sensor™ PTFE Nitinol, and Amplatz Super Stiff™ guidewire should be kept away from the surgical field when the high power settings of the laser are being used. The body parts of the guidewires can be utilized in the surgical field safely.
Introduction
L
Guidewires are “sine qua non” for endourologic procedures. They are used to understand the luminal continuity during the surgery or to maintain a safety situation in case of complications and to insert a Double-J stent emergently and are used in the course of renal access. Insertion of a safety wire is recommended for a best clinical practice of ureteroscopy. 2 Different types of guidewires are being used in the practice of urology and the differences between them are due to their covering materials, hydrophilicity, stiffness of the body part and the flexibility characteristics. In this study, the durability of five different types of guidewire against laser energy was evaluated in an in vitro experimental ureteral model. The types of selected guidewires for the experiment have frequently been used in the practice of urology. Criticism of any material or company was not aimed in this work.
Materials and Methods
The study was performed in the operating theater of the Department of Urology, Medicine Faculty of Ahi Evran University. An in vitro experimental ureteral model was created for the work; a silicon ureteral model in a saline-filled container (Fig. 1a). The ureteral model was 30F (10 mm) in diameter. Experiments were performed on five different types of guidewire; ZIPwire™ (Boston Scientific, Marlborough, MA), Sensor™ polytetrafluoroethylene (PTFE) Nitinol guidewire (Boston Scientific), Roadrunner® PC wire guide (Cook© Medical, Bloomington, IN), Amplatz Super Stiff™ (Boston Scientific), and Zebra™ Urologic Guidewire (Boston Scientific) (Table 1).
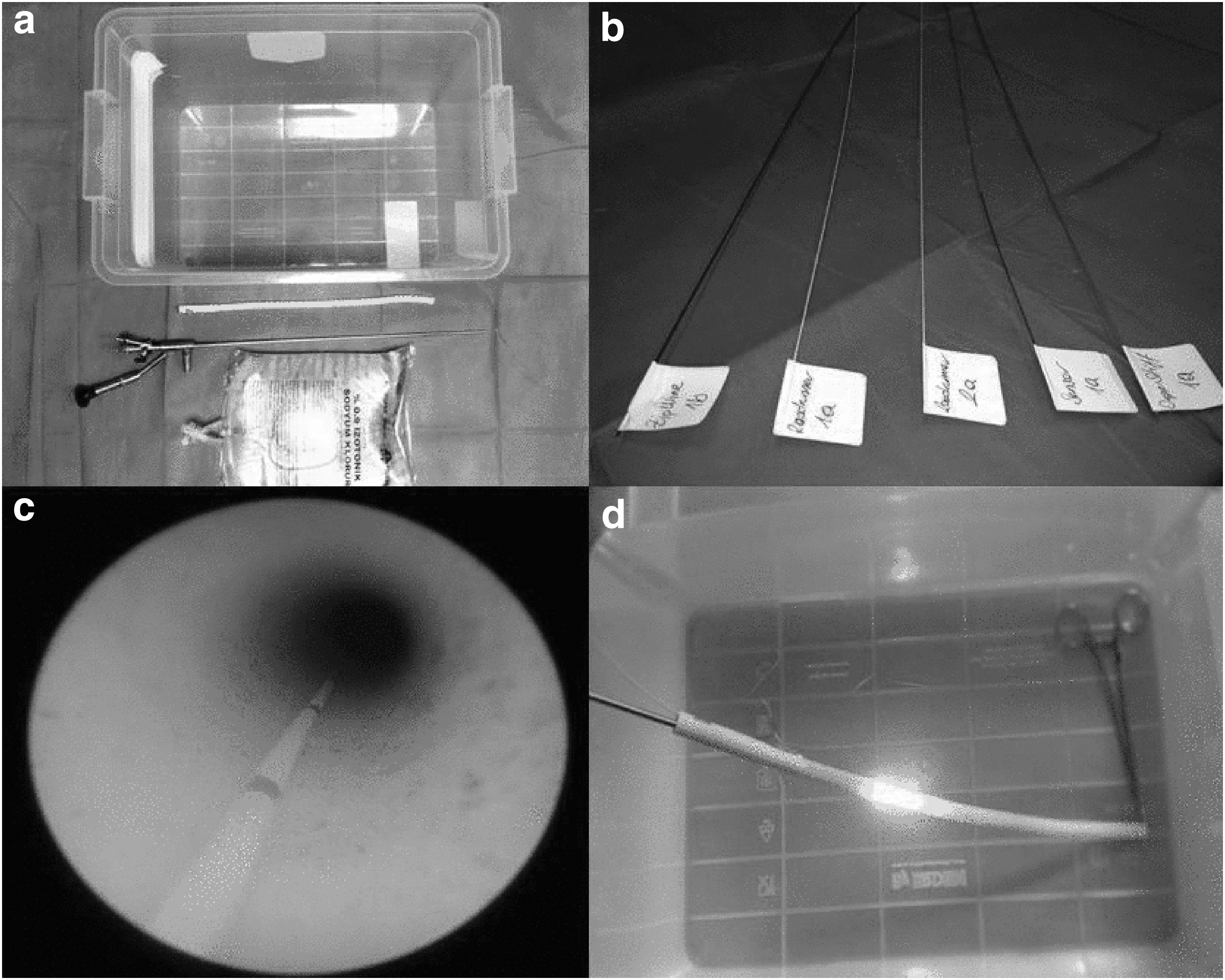
In vitro experimental model.
PTFE = polytetrafluoroethylene.
Guidewires were distributed into five groups; group 1, group 2, group 3, group 4, and group 5 for ZIPwire, Sensor, Roadrunner, Amplatz Super Stiff, and Zebra, respectively. Then, 0.035 and 0.038F guidewires were tested in groups. Five 0.035 and five 0.038F guidewires for each type of guidewire were planned to be tested, in groups. Guidewires were arranged with Arabic numbers from one to five. The 0.035F guidewires were named as “a” and 0.038F guidewires were named as “b.” As an example; the first ZIPwire 0.035F guidewire was appointed as “group 1, 1a” (Fig. 1b).
A red felt-tip pen was used to mark the points of experiments on the guidewires before the experiment. Three points were signed at intervals of 1 cm in the tip part, and three points were marked at intervals of 1 cm on the body part for each guidewire (Fig. 1c). The experiment on the body part was made at about 20 cm from the tip of the guidewires.
Experiments were performed separately for each guidewire in the experimental groups. The durability of the guidewires against the laser energy was tested in a saline-filled container. Silicon ureteral model was immersed into the saline, and guidewires were inserted into the in vitro ureteral model sequentially during each experiment. Afterward, 8/9.8F ureterorenoscope (Richard Wolf, Knittlingen, Germany) was pushed forward into the in vitro ureteral model. Laser fiber was inserted into the working channel and fired through the guidewire under direct vision in the artificial ureter (Fig. 1d).
A Holmium:yttrium aluminum garnet (Ho:YAG) laser system (Sphinx 30 Minimally Invasive Surgical Laser; LISA Laser, Pleasanton, CA) and a laser fiber with a core diameter of 550 μm (LISA Laser) were used for the experiment. The experiment was conducted 2 months after the last annual calibration of the laser machine. Laser fibers were contacted to the guidewire, and laser energy was fired to the premarked tip and body parts in three different adjustments; 1 J × 10 Hz (10 W), 2 J × 10 Hz (20 W), 3 J × 10 Hz (30 W). The flexible tip part and the more stiff body part of the guidewires were tested against laser energy separately for each experiment.
Laser energy was planned to be fired against the premarked parts 200 times per experiment. If the breakage of the guidewire had occurred before the 200 hits, it was recorded at this value. The experiment of the 1 J × 10 Hz (10 W) and 2 J × 10 Hz (20 W) on the tip and body parts were finished after 200 shots. If the breakage had not occurred after 200 shots with 3 J × 10 Hz (30 W), the experiment continued until 1000 hits with this energy output both for body and tip parts. Endurance against different energy levels, the number of shots and total joule that was reached in the experiments were recorded for the tip and body of the guidewires separately and compared.
Statistical analysis
Data were expressed as a minimum, maximum, and mean ± standard deviation for continuous variables and number for categorical variables. Statistical comparisons were made among the groups that the guidewires were broken in the experiments. Kruskal–Wallis H test was used for homogeneity of variables. Normality of distribution was analyzed with Kolmogorov–Smirnov test. Post hoc Duncan's multiple range tests were utilized for the comparison of the groups. Statistical Package for Social Sciences version 21.0 software for Windows (IBM SPSS Statistics for Windows, Version 21.0; IBM Corp., Armonk, NY) was used for the statistical analysis of the findings. p < 0.05 was considered as statistically significant.
Results
A total of 42 guidewires were used for this study; group 1a: five, group 1b: five, group 2a: five, group 2b: five, group 3a: three, group 3b: three, group 4a: five, group 4b: five, group 5a: three, group5b: three. The flexible tip part and the more stiff body part of the guidewires were tested against laser energy separately for each experiment. Each experiment was performed against the premarked points on the wires.
The breakage of the guidewires was detected in group 1a, group 1b, group 2a, group 2b, group 4a, and group 4b. The breakages have occurred only on the flexible tip parts of the guidewires (Fig. 2a, b, and d). The body parts of the guidewires of these three groups were resistant to laser energy and did not break.
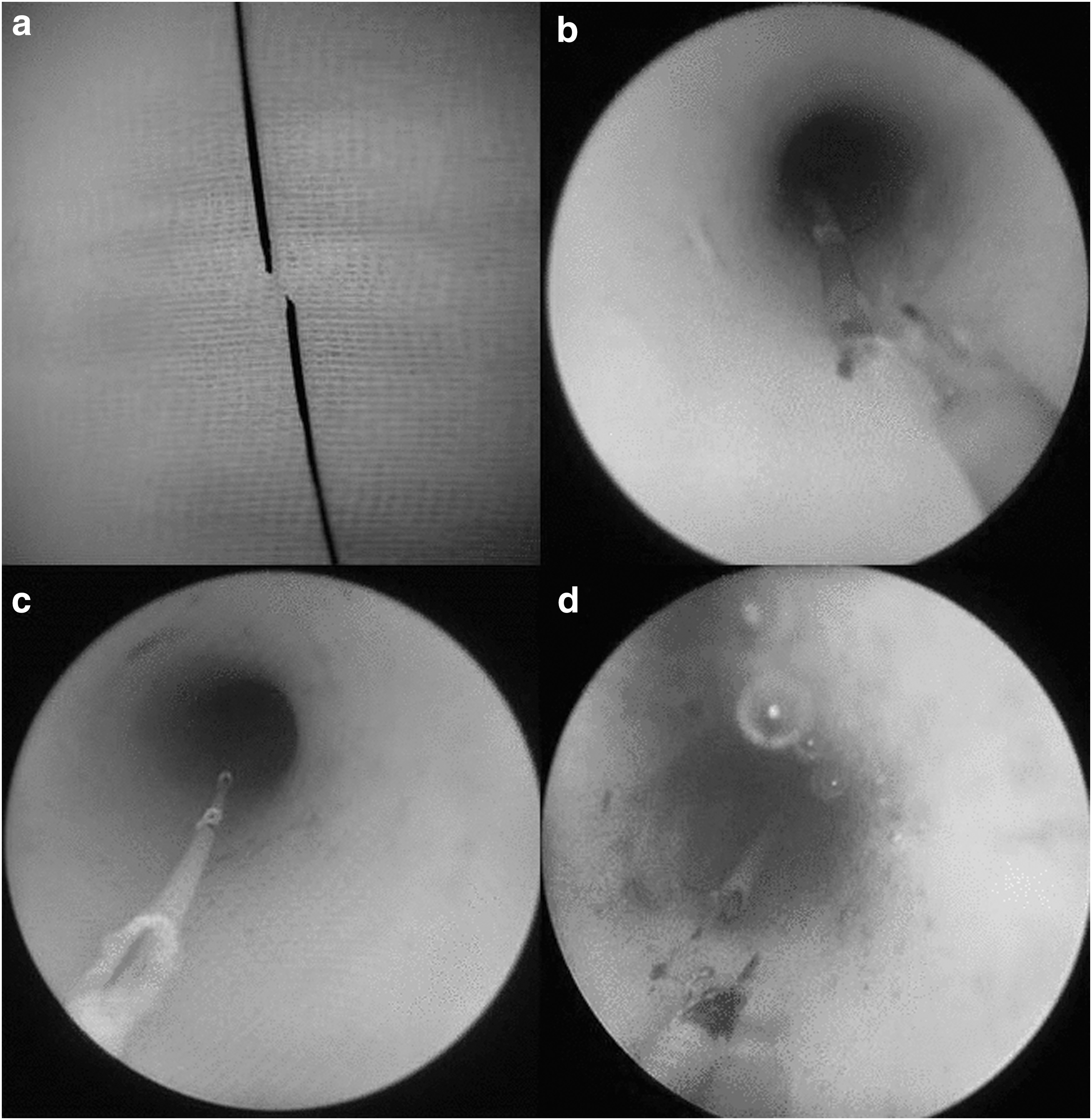
Laser effects on the guidewires.
The breakage of the guidewire was detected on neither the flexible tip part nor the body part of the guidewires in groups 3 and 5.
The breakage of the guidewires occurred after 3 J × 10 Hz (30 W) experiment in group 1, group 2, and group 4. The mean output values that cause breakage were given in Table 2. Statistical comparisons were made between the six subgroups (group 1a, 1b, 2a, 2b, 4a, and 4b). Kruskal–Wallis H test showed that there was a statistically significant difference in “total joule score” between the different subgroups, χ2 = 21.170, p = 0.001, with mean rank total joule of 5.20 for group 1a, 5.80 for group 1b, 19.40 for group 2a, 25.00 for group 2b, 18.20 for group 4a, and 19.40 for group 4b. Group 1a and 1b were different from group 2a, 2b, 4a, and 4b according to this test.
A Kolmogorov–Smirnov test was used to test for normality on group 1a, 1b, 2a, 2b, 4a, and 4b (p = 0.10). There was a statistically significant difference between groups as determined by one-way analysis of variance [F (5,24) = 27.315, p < 0.01]. Post hoc Duncan's multiple range tests revealed that group 1a and 1b are weaker against laser energy than group 2a, 2b, 4a, and 4b.
In group 3, the coating material on the tip or body parts of the wires were damaged by laser energy (Fig. 2c).
In group 5, the tip and body portions of the guidewires were resistant to laser energy. A mild curvature occurred at the tip part after 3 J × 10 Hz experiment. The body part was not affected after the experiments made with different power settings.
The experiments were terminated in group 3 and five after three guidewires were used and no breakage has occurred in each subgroup of these groups.
Discussion
The laser “light amplification by stimulated emission of radiation” is a light energy that produced by stimulating an atom with an external power source. 3 In contrast to ambient light, laser light is monochromatic (one wavelength photons) and coherent (waves are “in phase”). 4 The intense light of the laser is used to cut, coagulate, and vaporize the tissue and other structures.
Ho:YAG laser has been used in urologic practice, since the 1990s. 5,6 The surgical treatment of urinary stones regardless of their composition and ablation of soft tissues can be successfully achieved with Ho:YAG laser. Today, it has a widespread usage in urologic practice. For instance, Ho:YAG laser lithotripsy is a possible gold standard for intracorporeal ureteroscopic lithotripsy. 7
Guidewires have an extensive usage in the practice of urology. During all the endourologic surgeries, which are performed from external meatus to the kidney, they are being used both for finding the luminal continuity and for safety in case of an emergency situation. A false passage, bleeding, mucosal defects, or perforations may be considered as an emergency. Insertion of a safety wire is recommended for a best clinical practice of ureteroscopy. 2 Maybe the most frequent usage of a guidewire is the guidance during the insertion of a Double-J stent and dilatation of a renal tract.
There are different types of guidewires. The most characteristic features that separate them from each other are the hydrophilicity, stiffness of the body part, and flexibility of the most distal tip part. Some types of guidewires are stiffer, and some are more flexible. The metal wherein the body part gives the stiffness and kink-resistance, and the polymer coating, AQ® or Slip-Coat® coating provides the hydrophilicity. In this study, five different types of guidewires were used to evaluate the durability of them against the laser energy.
Laser energy is transferred via a laser-fiber. The direct irradiation of the tissue and stones with laser energy increases the heat. After chemical breakdown with increased temperature, vapor bubble achieves fragmentation or ablation. 8 Laser may damage the surrounding tissues and surgical devices by the same mechanism.
Ho:YAG laser is a solid-state laser with an operational wavelength of 2.1 μm. It is used for tissue ablation, urolithiasis treatment, and dentistry. It has a 0.4 mm tissue penetration capability. 9 If it is not used carefully, it may harm the surrounding tissues and the other surgical devices. 10 Eye injuries, ureteral perforation, bladder perforation, minor skin burns, internal burns, bleeding, and death caused by lasers that are being used in urology has been reported as adverse events. 11 Ho:YAG laser may damage the devices that were used during endourologic operations. 12,13 It has been shown that laser could damage antiretropulsion devices during the endourologic procedures. 1,12 Ho:YAG laser can damage guidewires. 12 During lithotripsy sometimes there may be a sandstorm or bleeding that causes the loss of the high quality of vision. Working with the laser under distorted vision may be dangerous and may harm surrounding tissues and structures. In such a case the guidewire may be damaged. A broken and overlooked guidewire may cause undesired consequences. 14
In this study, after working on five different types of guidewires, it has been understood that there are durability differences among the guidewires against the laser energy. The laser energy can break the tip parts of Zipwire, Sensor PTFE Nitinol, and Amplatz Super Stiff guidewires. The tip parts of Roadrunner PC wire guide and Zebra Urologic Guidewire are more resistant to breakage by laser energy. The tip part of the wires in group 3 and group 5 are different (Table 1). There is platinum in the tip part of the wires in these groups, and this may be the possible explanation of the resistance of these guidewires. The body parts of the wires in all study groups are resistant to laser energy. The laser could not break the body parts of the wires after 1000 shots with 3 J × 10 Hz.
The laser can cut the end portion of a guidewire. In case of such damage, the broken fragment may escape to the kidney. 12 If there is not a flexible ureterorenoscope among the equipment of the clinic, it could be difficult to reach the broken fragment of the guidewire. This situation can be accepted as malpractice. In case of an unnoticed broken guidewire piece, the retained foreign body may cause undesired consequences. Also, the guidewires that were used in this experiment are reusable devices. After an in vivo laser damage, safe reuse is impossible.
The in vitro model was a ureteral model in this study, and the laser fiber was fired to the guidewire with a narrow angle similar to a true ureterorenoscopy. The guidewire may be exposed to a more perpendicular angle to the laser energy during a retrograde intrarenal surgery and may be broken at lower energy levels.
In this study, a 550 μm laser fiber was used for the experiments. In this study 200 and 365 μm laser fibers were not utilized, and this may be accepted as the limitation of this study.
Conclusions
In this study, after working on five different types of guidewires, it has been understood that there is durability difference among the guidewires against the laser energy. The laser energy can break the tip parts of Zipwire, Sensor PTFE Nitinol, and Amplatz Super Stiff guidewire. However, the body parts of the wires in all study groups are resistant to laser energy up to 1000 hits with a 3 J × 10 Hz energy level. The tip parts of Zipwire, Sensor PTFE Nitinol, and Amplatz Super Stiff guidewire should be kept away from the surgical field when the high power settings of the laser are being used. The body parts of the guidewires in all study groups are resistant to laser energy, and they can be safely utilized in the surgical field.
Footnotes
Acknowledgments
This work was supported by Ahi Evran University Scientific Research Projects Coordination Unit. Project Number: TIP.A3.16.010. The author thanks Prof. Dr. Ayhan Karabulut for his scientific support. The author also thanks Dr. Samet Cetinkaya and Fatma Eroglu for their technical support.
Compliance with Ethical Standards
This study have been performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The author has no financial disclosure for this study.
Author's Contribution
S.B.—Protocol/project development, data collection or management, data analysis, article writing/editing.
Disclosure Statement
No competing financial interests exist.