
Abstract
Objective:
The aim of the study was to test the hypothesis that high levels of preoperative C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are associated with an increased risk of systemic inflammatory response syndrome (SIRS) following percutaneous nephrolithotomy (PCNL).
Materials and Methods:
This is a retrospective study of patients who underwent PCNL at our institution between October 2012 and October 2013 when ESR and CRP levels were part of our standard preoperative order set. The primary endpoint was development of SIRS. Receiver operating characteristic curves were used to evaluate the discriminative ability of the test.
Results:
Among the 107 PCNLs performed during the study period, 35 (33%) patients had evidence of SIRS during the postoperative stay. Patients who experienced SIRS had a longer operative time (99 min vs. 85 min, p = 0.016), were more likely to have been transferred to the intensive care unit (ICU) (15% vs. 0%, p = 0.002), and experienced a longer length of stay (2 days vs. 1 day, p < 0.001). On multivariable analysis controlling for operative time and positive urine culture, ESR (odds ratio [OR] 1.32, 95% confidence interval [CI]: 1.01–1.72, p = 0.04) and CRP (OR 1.59; 95% CI: 1.07–2.37, p = 0.02) were associated with development of SIRS. Among patients without a positive urine culture, an ESR >6.5 mm/hr (AUC 0.62; 95% CI: 0.52–0.78) had sensitivity, specificity, and negative predictive value (NPV) of 70.4%, 61.5%, and 80.0%, respectively, for development of SIRS. Among all patients, a CRP >0.65 mg/dL (AUC 0.63; 95% CI: 0.51–0.74) had sensitivity, specificity, and NPV of 51.4%, 69.4%, and 74.6%.
Conclusions:
A preoperative blood test for ESR and CRP was predictive for the development of SIRS after PCNL. This knowledge could be used to risk stratify patients and guide duration of antibiotic prophylaxis before PCNL, particularly among those without a positive urine culture.
Introduction
S
Systemic inflammatory response syndrome (SIRS) is a condition closely associated with and has been part of the sepsis definition. 4,5 Due to this association as well as the clear and specific diagnostic criteria, SIRS serves as an important surrogate in the evaluation of infection-related complications following PCNL.
Several patient characteristics have been found to be associated with the risk of infection after PCNL, including positive preoperative urine culture, female gender, preoperative nephrostomy tube, presence of urinary diversion, stone size, hydronephrosis, and staghorn stone. 6 –10 Unfortunately, these risk factors have been inconsistent across studies. Even a positive preoperative urine culture, which urologists often rely on to perform sterilization and guide perioperative antibiotic selection, 11 was only shown to have a 15% positive predictive value for SIRS in one study. 12 This is likely because the mid-stream urine samples do not accurately represent infection present in the upper tracts. 13 Renal pelvic urine and stone cultures are better associated with the development of postoperative sepsis; unfortunately, their results are often not available preoperatively. 7
The inflammatory markers, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), are acute phase reactants, which are both inexpensive and noninvasive to measure. They have been utilized in orthopedic surgery to predict the diagnosis of infected implants. 14 In urologic literature, ESR and CRP have been shown to be helpful in distinguishing simple hydronephrosis from pyonephrosis. 15 We hypothesized that preoperative elevations in ESR and CRP may better reflect underlying infection in the upper tracts and therefore the development of postoperative infection. Using SIRS as a surrogate marker for infectious complications, we tested whether preoperatively elevated ESR or CRP is associated with an increased risk of SIRS after PCNL.
Materials and Methods
After obtaining institutional review board approval, we reviewed all adult patients who underwent PCNL at our institution between 10/2012 and 10/2013. During this time period, ESR and CRP levels were part of our standard preoperative order set. Informed consent was not required for this analysis of retrospective data. Second-look PCNLs were excluded from the study.
Patient demographics and preoperative variables were collected, including age, sex, height, weight, presence of diabetes, neurogenic bladder, anatomic abnormalities of the urinary tract, stone size, and presence of hydronephrosis. Preoperative laboratories collected ESR, CRP, white blood cell (WBC) count, urine analysis, and urine culture results. Serum WBC was only included if it was drawn within 1 week of CRP/ESR.
Plasma level of CRP was measured using turbidimetric immunoassay and ESR was determined by Westergren's method at the central laboratory in our institution. These markers were analyzed both as continuous variables and as high or normal using predefined cut points. A high CRP was defined as >1.0 mg/dL, and a high ESR was defined as >10.0 mm/hr—these were based on the laboratory reference range at our institution.
Operative time was measured as the time from incision (insertion of the cystoscope for retrograde access) to closing (placement of the urethral catheter). A positive preoperative urine culture was defined as culture showing growth >100,000 colony-forming units (CFUs) of a bacterial species. Stone burden was defined as the sum of maximal diameters of all stones present on the side of the PCNL as measured on axial and coronal views of computed tomography (CT) scan. Presence of a staghorn stone was also recorded. If the stone was sent for analysis, the primary component (≥50%) was recorded. All patients undergoing PCNL at our institution received antibiotic prophylaxis as per AUA best practice statement. 11 This typically involved cefazolin 1 g or ciprofloxacin 500 mg for penicillin allergic patients. Patients with a positive preoperative urine culture were treated with 1 week of antibiotic therapy before surgery. With regard to irrigation, PCNLs were performed with irrigant bags suspended 100 cm above the surgical table for a standard irrigation pressure. When needed, a pressure cuff was inflated to 150–300 mmHg to improve visualization; however, a 30F sheath was used for all cases to maintain low intrarenal pressure.
Endpoint
The primary endpoint for this study was the development of SIRS in the postoperative hospitalization stay. SIRS was defined as having two of the following: temperature ≥38°C or ≤36°C, heart rate >90 beats per minute, respiratory rate >20 breaths per minute, or WBC count >12,000 cells/μL or <4000 cells/μL. 16 At our institution, vitals were measured every 4 hours for the first 24 hours and every 6 hours thereafter.
Statistical analysis
Differences among those who experienced SIRS were compared with those who did not using the Wilcoxon rank sum test for continuous variables and the chi-square or the Fisher exact test (when counts <5) for categorical variables. Multivariable logistic regression was used to study the relationship between ESR level, CRP level, and the risk of developing SIRS. The model was adjusted for operative time and presence of a positive preoperative urine culture (yes or no) as these are common risk factors associated with post-PCNL infection. 17 Assessment of model fit was done using the le Cessie-van Houwelingen-Copas goodness of fit test. 18 We used receiver operating characteristic (ROC) curves to determine whether ESR or CRP could be used to identify patients at increased risk for developing SIRS. The area under the ROC curve (AUC) was calculated and their 95% confidence limits were computed according to the method established by DeLong. The optimal threshold was determined using the Youden Index, which maximizes the sum of sensitivity and specificity. All tests were performed at a significance level of 0.05. R Statistical Software v3.14 (Vienna, Austria) was used for all analysis. The pROC package was used for ROC analyses. 19
Results
Baseline characteristics
A total of 107 patients underwent 110 PCNLs during the study period. Three patients underwent staged bilateral PCNLs (>1-month interval) and each surgery was included as a separate data entry. Three procedures were excluded as the preoperative ESR or CRP was obtained more than 30 days before surgery. Of the remaining 107 PCNLs, 35 (33%) individuals experienced SIRS during the postoperative hospital stay. Of those patients who met SIRS criteria, the common reasons were for WBC changes (80%), heart rate changes (74%), temperature (40%), and respiratory rate (23%). Among those experiencing SIRS, 3 (9%) were diagnosed with sepsis. The median time between drawing of ESR and CRP and surgery was 8 days (IQR 4.5–25.0). Baseline characteristics of the patients are shown in Table 1. There were no significant differences in age, gender, BMI, stone burden, presence of hydronephrosis, and stone composition between those who experienced SIRS and those who did not (Table 1). None of our patients had a predominance of struvite (magnesium ammonium phosphate) composition, but two patients had a struvite component <20%. Patients who experienced SIRS had higher preoperative WBC count (8.5 k/μL vs. 7.4 k/μL, p = 0.02), a longer operative time (99 min [78–147] vs. 85 min [58–112], p = 0.02), were more likely to be have been transferred to the ICU postoperatively (14% vs. 0%, p = 0.003), and had a longer length of stay (median 2 days vs. 1 day, p < 0.001). Of the 5 people who required transfer to the ICU, the primary reasons for transfer were respiratory difficulty (n = 2), hypotension (n = 2), and stroke (n = 1).
Elevated CRP defined as >1.0 mg/dL.
Elevated ESR defined as >10.0 mm/hr.
A positive urine culture was defined as showing growth of >100,000 CFUs of at least one organism.
A complete microscopic urine analysis was only available for 88 patients.
Stone burden was defined as the sum (in mm) of all stones measured on axial CT.
For mixed stones, the type ≥50% was used. A stone composition was only available in 92 patients.
HPF, high-power field; Hb, hemoglobin; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; WBC, white blood cell; RBC, red blood cell; BMI, body mass index; IQR, interquartile range; ICU, intensive care unit; PCNL, percutaneous nephrolithotomy.
Association of ESR and CRP with SIRS
Preoperative CRP was significantly higher in patients who developed SIRS (0.7 mg/dL [0.2–1.4] vs. 0.3 mg/dL [0.1–0.8]; p = 0.028). Preoperative ESR was not significantly different between groups (8.0 mm/hr [4.5–24] vs. 5.5 mm/hr [2.0–13]; p = 0.07). Based on laboratory-defined cutoffs described previously, those patients who experienced SIRS were more likely to have a high CRP preoperatively (37% vs. 17%, p = 0.02), but there was no association with a high ESR (37% vs. 35%, p = 0.81). The combination of both high ESR and high CRP was not associated with SIRS (20% vs. 8%, p = 0.11). Likewise, having at least one high marker was not associated with SIRS (54% vs. 43%, p = 0.28). ESR (OR 1.04 per 1 mm/hr, 95% CI: 1.01–1.07; p = 0.006) was significantly associated with a positive preoperative urine culture, but preoperative CRP was not (OR 1.2, 95% CI: 0.94–1.60, p = 0.12).
We performed a subgroup analysis excluding people who had a positive preoperative urine culture (>100 k CFUs). This particular group was chosen to evaluate the value of ESR or CRP in a group without an active urinary tract infection as this would be expected to elevate reactive markers. A total of 27 (25%) patients had positive urine cultures and were excluded. Of the remaining 80 individuals, 27 (34%) experienced an SIRS event postoperatively. In this group, preoperative ESR (8 [4–21] mm/hr vs. 4 [1–10] mm/hr, p = 0.034) was significantly higher in patients who experienced SIRS. CRP was also higher, but did not reach statistical significance (0.5 [0.2–1.3] mg/dL vs. 0.2 [0.1–0.7] mg/dL, p = 0.068) (Table 2).
On multivariable analysis controlling for positive preoperative urine culture and operative time, both CRP (p = 0.023) and ESR (p = 0.044) were individually associated with the development of SIRS. Operative time remained significantly associated with development of SIRS in all models (Table 3).
Four multivariable logistic regression models were constructed, incorporating continuous and categorized values of ESR and CRP. Each model controlled for the presence of a positive urine culture (> 100 k CFUs) and operative time.
Goodness of Fit, p = 0.80.
Goodness of Fit, p = 0.40.
Predictive value of ESR and CRP
ROC analysis of ESR to discriminate between patients who developed and those who did not develop SIRS showed an AUC of 0.61 (95% CI: 0.49–0.72) (Fig. 1). The optimal threshold value for ESR was 6.5 mm/hr, which had a sensitivity, specificity, positive predictive value, and negative predictive value (NPV) of 71.4%, 51.4%, 41.7%, and 78.7%, respectively. When the 28 patients with positive urine cultures were excluded, the AUC improved to 0.62 (95% CI: 0.52–0.78). The sensitivity remained similar at 70.4%, specificity increased to 61.5%, positive predictive value increased to 48.7%, and NPV increased to 80.0%.
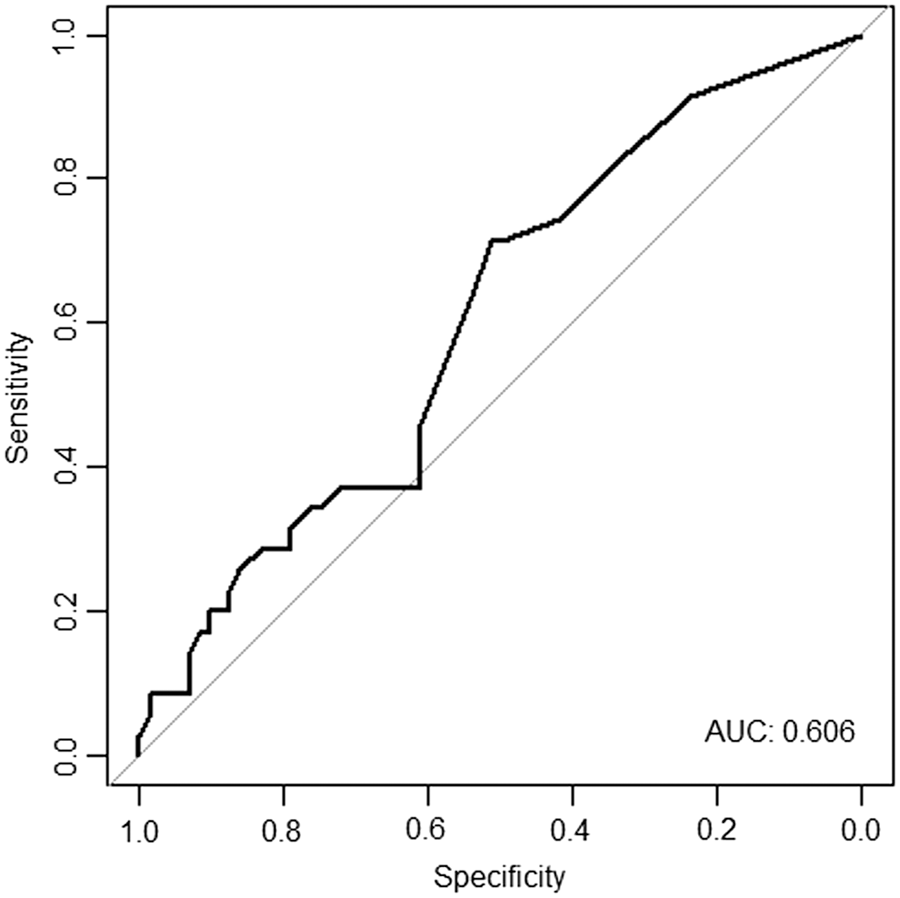
ROC curve for ESR for predicting SIRS after PCNL. ESR, erythrocyte sedimentation rate; PCNL: percutaneous nephrolithotomy; ROC, receiver operating characteristic; SIRS, systemic inflammatory response syndrome.
ROC analysis of CRP to discriminate between patients who developed SIRS and those who did not showed an AUC of 0.63 (95% CI: 0.51–0.74) (Fig. 2). The optimal threshold of 0.65 mg/dL had a sensitivity, specificity, positive predictive value, and NPV of 51.4%, 69.4%, 45.0%, and 74.6%, respectively. When 28 patients with a positive urine culture were excluded, the AUC remained similar 0.63 (95% CI: 0.50–0.76). The sensitivity decreased to 44.4%, specificity increased to 73%, positive predictive value remained similar at 46.2%, and NPV decreased to 71.7%.
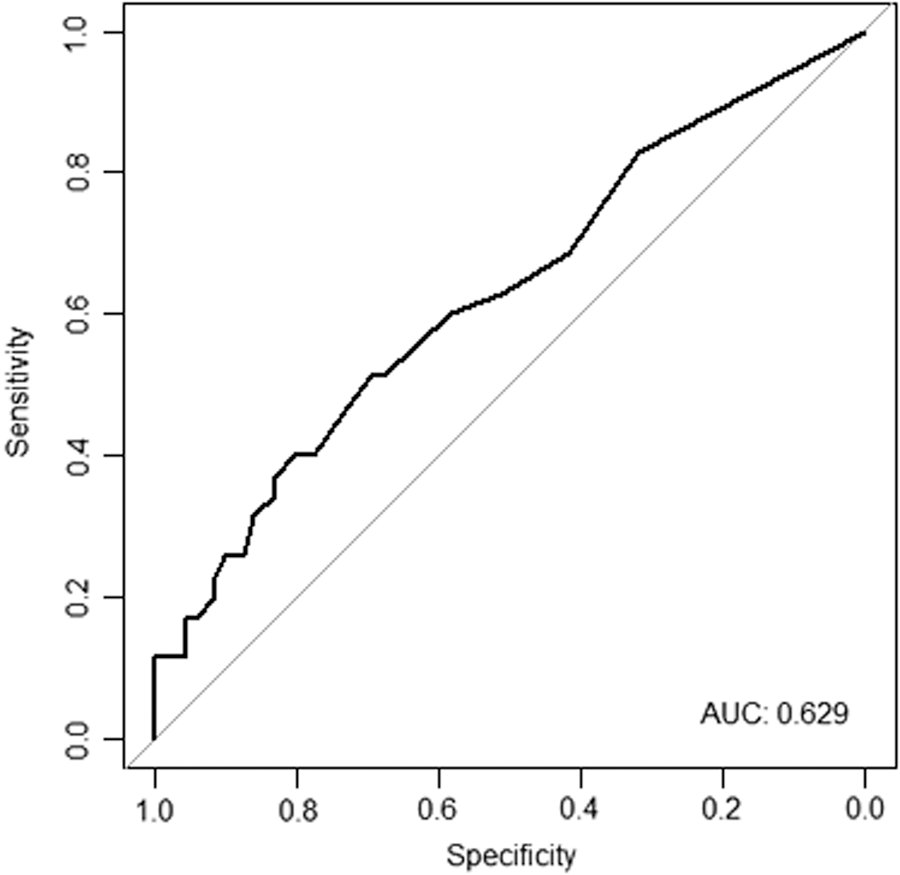
ROC curve for CRP predicting SIRS after PCNL. CRP, C-reactive protein.
Among all patients, the combination of a high ESR and CRP using thresholds of 6.5 mm/hr for ESR and 0.65 mg/dL for CRP had a lower sensitivity at 31% and higher specificity at 78%, with similar positive and NPV of 41% and 70%.
Discussion
In this retrospective study among patients undergoing PCNL over a one-year time period, we found that a preoperative ESR (in patients without a positive urine culture) and CRP (in all patients) were predictive for the development of SIRS postoperatively. A further finding of our study was that a cutoff value of ESR of 6.5 mm/hr optimally discriminated between patients who experienced SIRS and those who did not with an NPV of 80.0%. Likewise, an optimal cutoff value of CRP of 0.65 mg/dL demonstrated an NPV of 71.7%.
Postoperative fever, urinary tract infection, and sepsis are common complications after PCNL that can lead to longer hospital stays, ICU stays, and need for additional antibiotics. Sepsis remains the most common perioperative cause of death. 2 Given the poor predictive value of a preoperative voided urine culture, there is a dire need for a preoperative predictor that identifies patients at higher risk who could then be monitored more carefully or be provided with additional antibiotic coverage.
To our knowledge, this is the first study to evaluate the utility of preoperative ESR and CRP as markers to predict postprocedural SIRS. In our study, 33% of patients experienced an SIRS event, which is within the range of what has been reported in other series, 11.2%–37%. 9,12,20
Several studies have investigated preoperative and intraoperative risk factors for the development of SIRS after PCNL. In a retrospective study of 209 patients, Chen and colleagues found that significant risk factors included stone size, presence of hydronephrosis, staghorn stone, longer operative time, multiple punctures, and need for blood transfusion. 9 Mariappan and colleagues found the presence of purulent material obtained on puncture, a positive renal pelvic urine culture, and a positive stone culture as significant risk factors. 21 Draga and colleagues found that paraplegia, prior PCNL, or stones in caliceal location were risk factors. 20
In our series, longer operative time was a significant risk factor for development of SIRS on multivariable analysis. This supports previous studies that have found operative time to be associated with SIRS, 9 septic shock, 10 and postoperative fever. 22
Both ESR and CRP are markers of inflammation. ESR, defined as the rate at which erythrocytes fall through plasma when placed in a vertical tube, is an indirect measurement of inflammation. 23 A variety of conditions unrelated to inflammation can increase the ESR. These include increased age and female gender, 24 obesity, 25 and renal disease. 26 CRP is a sensitive acute-phase reactant and a marker of cytokine-mediated inflammation. Its level in the plasma can rise hundred times the normal during bacterial infections. 27 It is more specific than ESR and can also be elevated in a variety of noninfectious conditions such as obesity, low levels of physical activity, aging, obstructive sleep apnea, depression, and diabetes. 28,29
In the overall cohort, ESR was not significantly associated with development of SIRS. However, in a subgroup analysis, excluding patients with a positive urine culture, those who developed SIRS had a significantly higher preoperative ESR. It suggests that among patients without an active urinary tract infection, ESR might have value in identifying those at a higher risk for postoperative infectious complications. Similarly, increasing CRP was independently associated with increased odds of developing SIRS postoperatively after controlling for operative time and the presence of a positive urine culture. Taken together, these findings suggest that elevations in ESR and CRP may reflect quiescent infection in the upper tracts, which may otherwise not be seen in the preoperative urine culture.
Numerous studies have investigated potential risk factors for the development of infectious complications following PCNL. Adding to these findings, our study shows that measurement of a preoperative inflammatory biomarker, CRP, with a cutoff of 0.65 mg/dL or ESR with a cutoff of 6.5 mm/hr has value in predicting SIRS after PCNL. Implications of this finding can help in decisions of timing and duration of antibiotic prophylaxis before PCNL, as well as need for closer monitoring in higher acuity bed postoperatively. Best practice policy statements 11 and guidelines 30 recommend prophylaxis with a single perioperative dose of antibiotic, with an increased duration for those at higher risk. Thus, patients with a negative urine culture, but elevated CRP or ESR, could be targeted for a longer duration of preoperative antibiotics.
In addition to ESR and CRP, another emerging marker of inflammation is procalcitonin. Procalcitonin is a precursor of calcitonin, which is released by cells in response to bacterial toxins. In a meta-analysis of nine observational studies, Wu and colleagues found that procalcitonin had a similar sensitivity to CRP for identifying bacterial infection (75% vs. 77%), but a much higher specificity (90% vs. 56%). 31 Given the findings of this study, procalcitonin may be an additional marker to evaluate as a predictor of infectious complications following PCNL.
There are several limitations of our study. Because ESR and CRP are nonspecific inflammatory markers, they can be elevated by factors other than infection. Second, ESR and CRP measurements were drawn at the time of the preoperative visit within the month before surgery (median 8 days prior). This leads to varying lengths of time between the laboratory draw and the PCNL and may not reflect their true risk of infection close to the day of surgery. Third, the retrospective design is a limitation, in that we can analyze only data that were important enough to be recorded at the time these patients underwent surgery. Fourth, pain, analgesia, and medications such as beta-blockers are factors that could impact the endpoint of the study by altering heart and/or respiratory rate. This was a nonspecific, but potentially confounding, factor we did not evaluate. Finally, while we found an association between these laboratory markers and SIRS, this does not necessarily mean it will be predictive of sepsis.
Conclusions
In conclusion, the present study showed that a preoperative blood test for ESR and CRP was predictive for the development of SIRS after PCNL. This knowledge could be used to risk stratify patients and guide duration of antibiotic prophylaxis before PCNL.
Footnotes
Acknowledgments
This article will be presented at the AUA Annual Meeting and has been published as conference proceedings in abstract format in the Journal of Urology.
Author Disclosure Statement
The authors report no conflicts of interest.