
Abstract
Objective:
To examine urine and stone bacteriology of struvite stone formers in a large cohort of patients undergoing percutaneous nephrolithotomy (PCNL).
Materials and Methods:
A total of 1191 patients, with stone and urine cultures, treated with PCNL for renal calculi were included in the study. Statistical differences were assessed using Mann–Whitney U and T-tests.
Results:
Stone cultures were positive in 72% of patients with struvite stones. Urea-splitting organisms accounted for only half of the positive stone cultures. Enterococcus (9/50, 18%), Proteus (9/50, 18%), and Escherichia coli (6/50, 12%) were the most commonly identified organisms. Notably, two-thirds of struvite formers with negative stone culture had at least one positive culture for a urea-splitting organism on urine culture going back 1 year from the time of surgery. A majority (67%) of struvite stone cultures were found to be resistant to first- and second-generation cephalosporins.
Conclusions:
The bacteriology of struvite stones has shifted away from traditional urea-splitting organisms and antibiotic coverage must be expanded to include organisms such as Enterococcus that do not respond to cephalosporins. Causative organisms may be found by going back in time to identify the initial organism that could have induced struvite stone formation to inform preventative therapy.
Introduction and Objective
K
Materials and Methods
We have maintained an institutional review board-approved database on all endourology patients since 2009 and identified all patients who underwent percutaneous nephrolithotomy (PCNL). The surgery was performed at two major medical centers in New York, but the surgical team was kept consistent and the same pre- and postoperative protocols were followed. Those who underwent PCNL for ureteral stones were excluded. Medical records from the two major New York healthcare systems, including outside medical records, were reviewed for culture results, use of antibiotics, and the presence of host-dependent urinary tract infection (UTI) risk factors, which were categorized as obstructive, neurogenic, foreign body, impaired host defense, and other.
Our routine protocol for antibiotic treatment before surgery was followed. We obtain preoperative urine cultures at least 10 days before surgery. If positive, antibiotics are selected according to sensitivities and given for 7 days, even if the patient is not demonstrating signs of infection (i.e., colonized, but not symptomatic), before the procedure. If the results are contaminated or multiple organisms grow, a repeat culture is performed with straight catheterization, especially in females, to get urine directly from the bladder particularly in cases where struvite stones are suspected. Generally, we withhold preoperative antibiotics if preoperative urine cultures are negative. However, in patients who have a history of infections, have had a recent UTI, or are suspected to have a struvite stone, a 5–7-day course of preoperative antibiotics is administered. Patients with active signs of infection (i.e., sepsis, fever) are treated first with a complete case of antibiotics before consideration for surgery. All patients, including those with prior negative cultures, receive dose-adjusted broad-spectrum intravenous antibiotics (generally ampicillin and gentamicin) within 1 hour of the procedure. PCNL was performed, and urine and stone cultures on all patients were collected according to our previously described protocol. 3 Briefly, we extract the urine from the renal pelvis by a retrogradely placed ureteral catheter before doing a retrograde pyelogram and place the urine into a sterile tube. When we extract the stone, we keep it sterile, wash it in saline, and then place it into a sterile tube where it is crushed into a slurry and sent for culture. The results of stone and urine cultures were reviewed.
Data were collected on urine cultures obtained intraoperatively, preoperatively, and within 12 months before PCNL. Patients with data outside of our two healthcare systems were requested to bring their medical records or provide the contact information of their primary healthcare facilities. Statistical Package for the Social Science was used for statistical analysis using Mann–Whitney U and T-tests.
Results
During the study period, 1191 patients underwent PCNL. After exclusions, a total of 50 struvite stones (>50% magnesium ammonium phosphate) were identified (Fig. 1). While there was no difference in mean age between struvite and nonstruvite formers, there was a statistically significant difference in gender distribution with predominance of females in the struvite group.
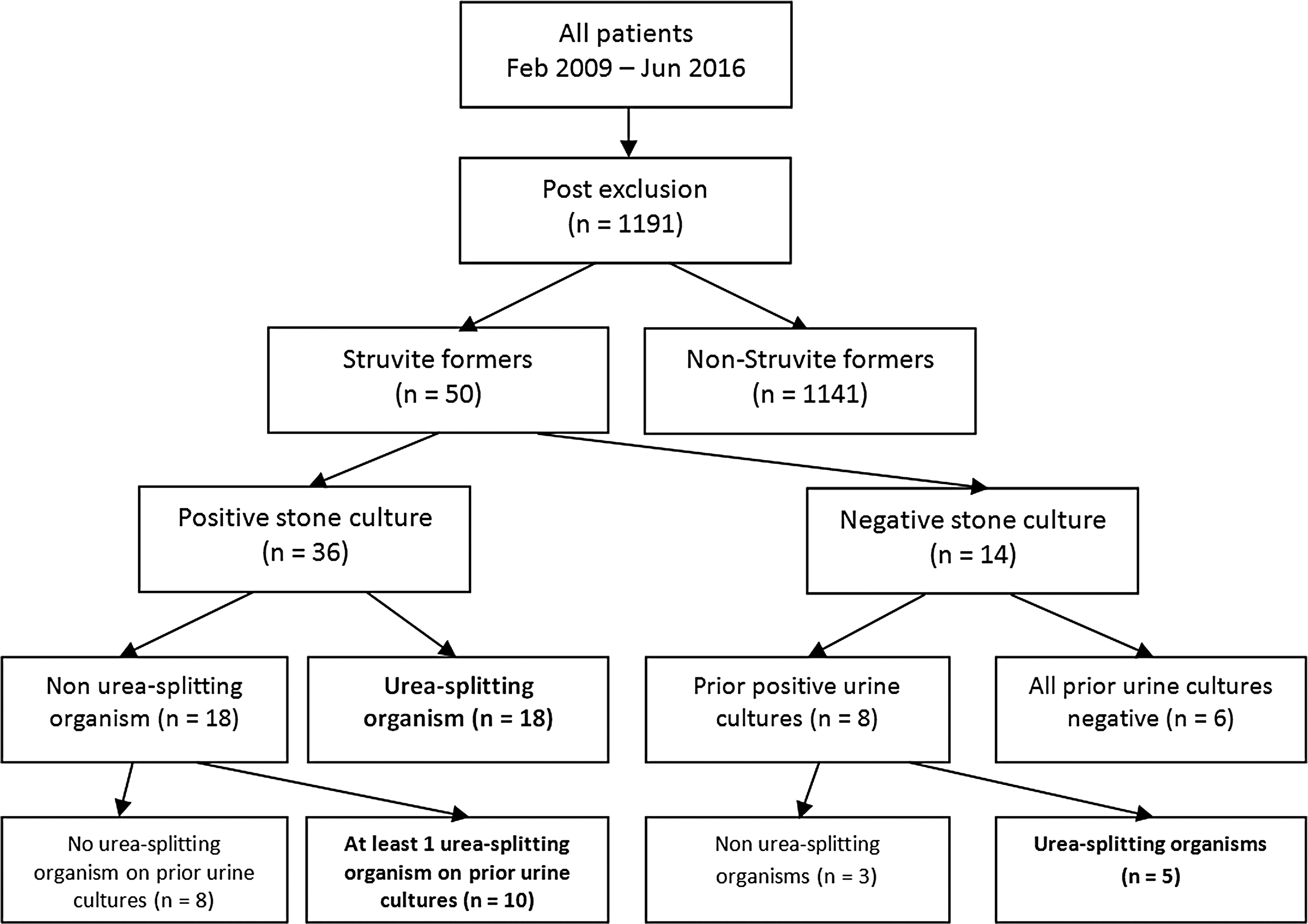
Flow diagram of study design and results.
Of the struvite stone formers, 66% (34/50) exhibited at least one UTI risk factor (Table 1) and 76% (38/50) had a history of recurrent UTI. A course of preoperative antibiotics was given to 90% (45/50) of eventual struvite patients based on preoperative urine cultures and/or suspicion of an infected stone being present.
DM = diabetes mellitus; HIV = human immunodeficiency virus; UPJ = ureteropelvic junction; VUR = vesicoureteral reflux.
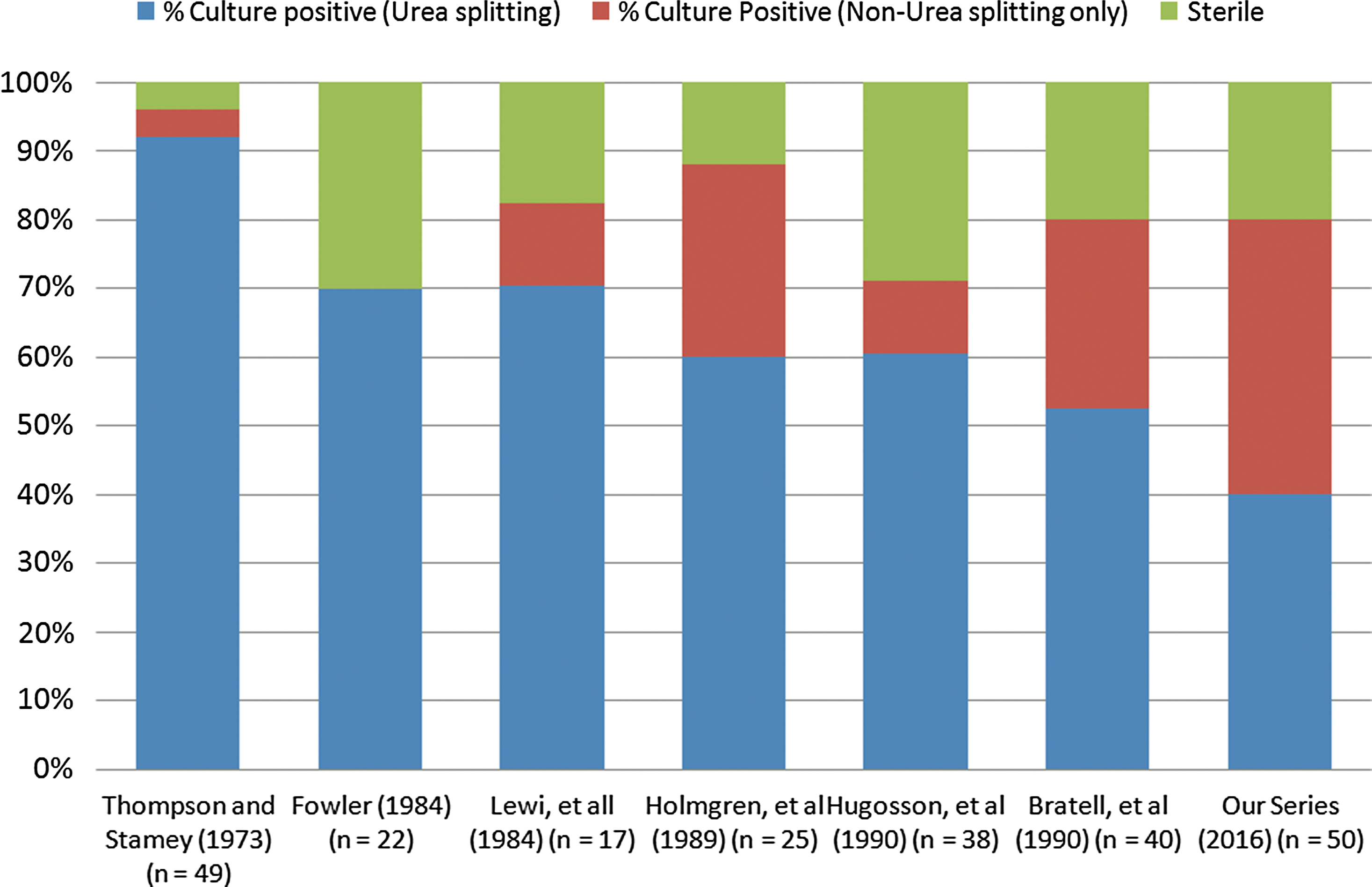
Bacteria grew from stone cultures in 72% of struvite patients compared to 23% in nonstruvite patients (p < 0.001) (Table 2). Twenty-eight percent of struvite stone cultures were sterile. One half of all positive struvite stone cultures grew traditional urea-splitting organisms, while the other half grew traditionally nonurea-splitting organisms (Fig. 2). A majority of struvite stone and urine cultures (67% and 53%, respectively) were found to be resistant to first- and second-generation cephalosporins. The most commonly identified organisms on stone cultures were Enterococcus (9/50, 18%), Proteus (9/50, 18%), and Escherichia coli (6/50, 12%) (Table 3). Interestingly, 66% of E. coli and 78% of Enterococcus patients, when going back in time, had a traditional urea-splitting organism on a prior urine culture within 12 months of PCNL.
Struvite stone culture results.
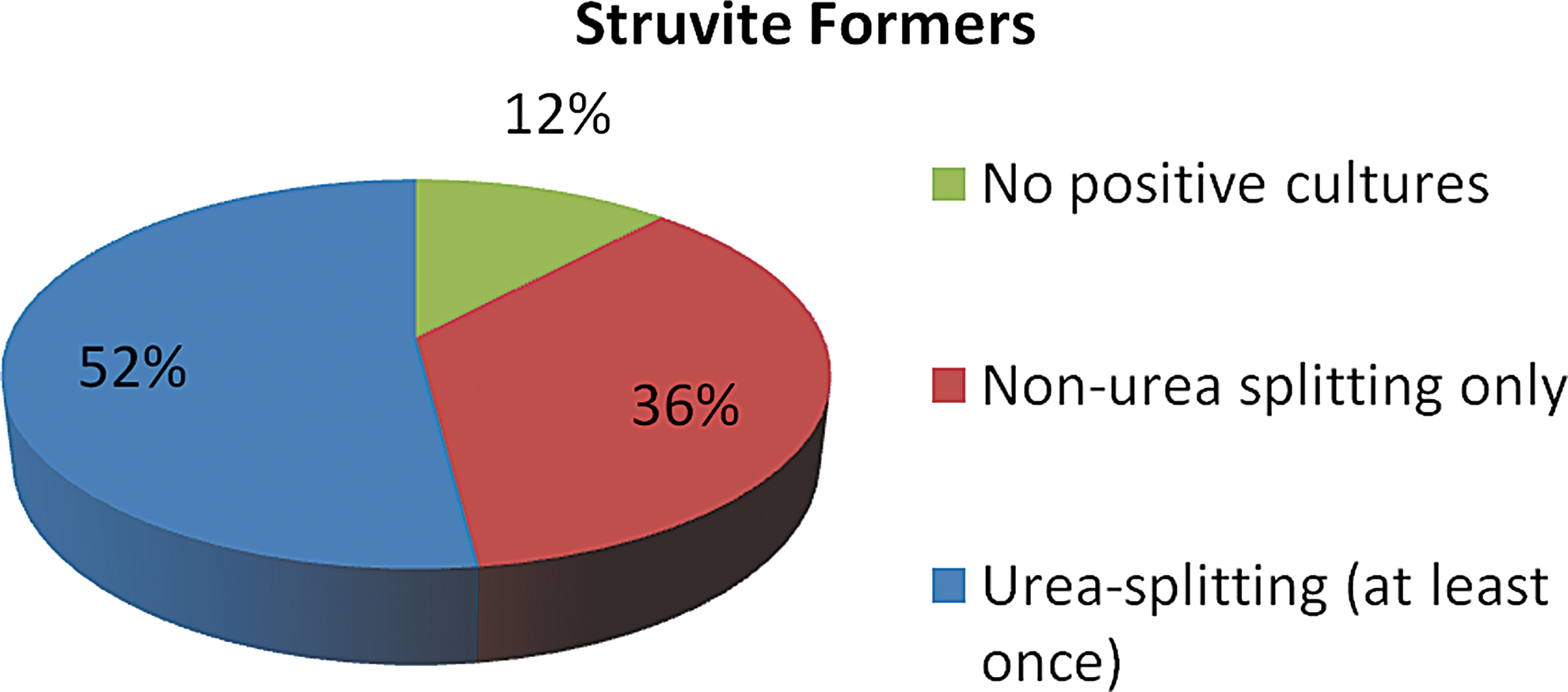
Overall, urine cultures from struvite formers were positive in 6% of intraoperative, 48% of preoperative, and 82% of patients collected during the 12 months before PCNL (Table 4). The most commonly identified organism on urine cultures were E. coli (33.3%), Proteus (27.3%), and Klebsiella (10.8%) (Table 5). Combining stone and urine culture data, 88% of struvite formers had at least one positive culture and 60% of those (52% of all struvite patients) had a urea-splitting organism grow on at least one culture (Fig. 3). The other 12% of struvite stone formers had no positive stone or urine cultures at all, even going back 1 year from the time of PCNL. The discordance between stone and urine cultures was 46%.
Stratification of all stone and urine culture results among struvite stone formers.
Discussion
Early studies identified that urease is produced predominantly by Proteus, Providencia, Klebsiella, Pseudomonas, and Staphylococcus species, indicating a strong causal relationship between struvite stones and urea-splitting organisms. 4 –7 The majority of studies from the 1990s, however, reported a notable decrease in the percentage of struvite stones associated with urea-splitting organisms (Fig. 2). 8 –10 Even though early studies demonstrated that only 1.4% of E. coli species produce urease, 5 Bratell and colleagues in 1990 found E. coli to be the predominantly isolated bacteria from cultures of struvite stones. 10 In addition, an increasing percentage of struvite stones have been sterile on stone culture. 8 –10
Our findings align with both these trends and also indicate a strong association of Enterococcus with struvite stones. In our series, only 36% of patients with struvite stones had a traditional urease-producing organism on stone culture. Also, 28% of all struvite patients had sterile stone cultures. A few factors may contribute to this observed shift in the bacteriology of struvite stones.
First, stones may be sterilized by preoperative antibiotics. 10 In our study, 8 of the 14 patients with negative stone cultures had positive urine cultures in the year before surgery. Five of these urine cultures yielded organisms known to be urease splitting (Fig. 1). Thus, appropriate preoperative therapy may eliminate or suppress bacterial proliferation to the point that no organism grows on stone culture.
Interestingly, 12% of struvite stone formers had completely negative stone and urine cultures up to 12 months before PCNL. Although one possible explanation for this phenomenon could be that our cultures are insensitive to detect all bacteria or that the bacteria get destroyed during processing of stones, our methodology for stone culture (crushing the stone in saline and creating a slurry that is then plated) is a standardized and validated technique that has been used by multiple authors. 3
In our series, a third of the patients had urine cultures that yielded bacterial species that are not typically urea splitting. This follows an interesting trend where a significant proportion of struvite stone cultures have yielded similar organisms. There are several possibilities that may explain these findings.
First, it is possible that the inciting organism for struvite lithogenesis is no longer present and that the nonurease-producing bacteria identified on stone culture represent secondary colonization. In this series, approximately half of the patients who had stone cultures with nonurease-producing organisms had a positive urine culture with a urease-producing organism in the year before surgery, lending credence to this possibility. A scientific explanation for this is that stone formation can occur either peri- or intrabacterially. 5 Intrabacterial formation of struvite crystals can cause bacteriolysis, rendering the stone free of its initial microorganisms. As stone propagation continues, the stone may then become secondarily infected with a different, nonurease-producing bacteria. 5 Therefore, identification of a urease-splitting organism, even if it is on a prior urine culture, should raise suspicion for a struvite stone.
Second, nonurea-splitting organisms can acquire the ability to produce urease. The urease enzyme is harbored on a plasmid that can be transferred between bacterial species through either genomic transformation or conjugation. 11,12 The alkaline environment that propagates growth of struvite stones is often a haven for multiple bacterial species, which presents ready opportunity for cross-species transfer of the urease-containing plasmid. Thus, our frequent identification of E. coli and Enterococcus as the dominant species on struvite stone cultures may be related to the horizontal gene transfer of the urease-encoding plasmid to these species. 13,14
Regardless of the etiology, the clinical implications of our findings are significant. Current American Urological Association guidelines recommend perioperative administration of a first- or second-generation cephalosporin for PCNL. 15 However, solely administering these drugs excludes coverage for Enterococcus, a predominant stone organism in our series. In addition, we found that 67% of the organisms were resistant to this recommended antibiotic regimen. This is important as appropriate antibiotic selection before the treatment of struvite stones is essential for the prevention of sepsis. Sepsis rates following PCNL have been reported as high as 7.6%. 16 These events prolong hospital stay and increase the morbidity of procedure recovery. As such, it is important for providers to consider the shifting trend in bacteriology of struvite stones, and treat the organism most likely to produce sepsis by including gram-positive bacterial coverage in perioperative antibiotic selection. Future guidelines should take into consideration these shifts in bacteriology for struvite stones.
It has been well established that preoperative urine cultures do not provide reliable prediction of the dominant organism on stone culture. A wide variability in concordance, ranging from 25% to 92.8%, has been reported. 4,17,18 In our study, we found a 46% discordance between urine and stone cultures. This underscores the importance of stone cultures in guiding antibiotic therapy, both to mitigate sepsis and to prevent recurrences. These cultures are usually available 24–48 hours after surgery and may allow one to tailor therapy to a particular organism. In our opinion, it is paramount for providers to obtain stone cultures if a struvite stone is suspected. It is also important in patients with suspected struvite stones to go back in time and review all prior cultures, at least within 12 months, to identify the specific organism likely responsible for the original stone formation, even if it means contacting providers and outside hospitals.
Two limitations of this present study must be considered. First, the sensitivity of our laboratory tests, despite using optimal methods for culturing stones, may make it difficult to detect less common organisms such as Ureaplasma urealyticum, Corynebacterium urealyticum, and fungi. 19 Second, significant geographic variation exists for antibiograms and colonization patterns. However, we believe our results to be generalizable as we are a tertiary care center accepting referrals all throughout the United States and abroad. In addition, our findings are consistent with studies from other parts of the world. 8 –10,20
Conclusion
Over the last few decades there has been a shift in the bacteriology of struvite stones. Our study confirms that traditionally nonurease-producing organisms are being identified with greater frequency on struvite stone culture. This includes E. coli and gram-positive organisms such as Enterococcus. These findings warrant consideration for updating guidelines to broaden prophylactic antibiotics before PCNL, especially in those patients at risk for harboring struvite stones, even if preoperative cultures are negative. Our study confirms recent literature suggesting the importance of conducting intraoperative stone cultures to identify causative organisms. In addition, physicians need to go back in time to identify the initial organism that could have induced struvite stone formation to inform preventative therapy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.