
Abstract
Purpose:
To assess the prevalence and extent of irrigation fluid absorption during thulium laser vaporization of the prostate.
Material and Methods:
Fifty-four patients undergoing thulium laser vaporization of the prostate were prospectively included into the trial at a tertiary referral center. Isotonic saline containing 1% ethanol was used for intraoperative irrigation. Absorption of irrigation fluid was measured periodically during the operation using the expired breath ethanol technique. Among others, intra- and postoperative changes in biochemical and hematological laboratory findings were assessed.
Results:
Absorption of irrigation fluid was detected in 7 out of 54 (13%) patients with a median absorption volume of 265 mL (227–615). No significant differences of intra- and postoperative blood parameters were observed between absorbers and nonabsorbers. No risk factor (i.e., age, prostate size, surgery duration, applied energy, and amount of irrigation fluid) for the occurrence of fluid absorption could be identified.
Conclusion:
Absorption of irrigation fluid also occurs during thulium laser vaporization of the prostate and should be kept in mind, especially in patients at a high cardiovascular risk. However, compared with previously assessed resection and vaporization techniques, thulium vaporization might have a favorable safety profile regarding fluid absorption.
Introduction
I
Improved intraoperative safety 3,4 as well as functional results comparable to TURP 5 have been shown especially for the 532 nm GreenLight HPS Laser System.
In addition to a reduction of intraoperative bleeding due to the excellent coagulation properties of laser vaporization, transurethral resection syndrome (TUR syndrome) can be prevented as isotonic saline is used as intraoperative irrigation fluid. However, a relevant intraoperative absorption of irrigation fluid, putting patients at an increased risk of cardiopulmonary complications, has been demonstrated for several laser techniques recently. 6 –8
During the last decade, thulium:yttrium–aluminium–garnet (Tm:YAG) lasers have been increasingly used in the treatment of BPO. Due to their physical characteristics, they allow various operation techniques like Tm:YAG vaporization (ThuVAP), vaporesection, vapoenucleation, and enucleation of the prostate. 9 Besides excellent tissue ablation rates, 10 a favorable safety profile as well as comparable functional outcomes compared with TURP have been reported for Tm:YAG lasers. 11 –14 However, in contrast to other operation techniques recommended for high-risk patients, the risk of intraoperative fluid absorption has never been assessed for Tm:YAG lasers so far.
Therefore, the aim of our study was to investigate fluid absorption during ThuVaP using the expired breath ethanol test.
Materials and Methods
This prospective study was approved by the local ethics committee (EKSG 14/035) and performed in accordance with the World Medical Association Declaration of Helsinki
15
and the guidelines for GCP
16
at a tertiary referral center. Patients had to be candidates for ThuVaP (based on clinical assessment, comorbidities, medication, and patient's preference), older than 40 years, and provide a written informed consent for study inclusion. Exclusion criteria were mild symptoms (International Prostate Symptom Score [IPSS] <8), urethral stenosis, bladder diverticulum bigger than 100 mL, chronic liver disease, former alcoholism, or alcohol consumption within 24 hours before operation. The study protocol was registered in the database of
Preoperative assessment included patient's age, height, weight, free uroflowmetry, postvoid residual urine, comedication, IPSS, physical status score of the American Society of Anesthesiologists (ASA Score, determined by anesthesiologist during preoperative assessment), laboratory studies, and transrectal ultrasound of the prostate.
All operations were performed by surgeons that were experienced with ThuVaP and had performed more than 100 transurethral interventions. A thulium continuous wave laser (RevoLix DUO 120 W; LISA laser products OHG, Katlenburg, Germany) and a 24F continuous flow cystoscope (Karl Storz Endoskope; Anklin AG, Binnigen, Switzerland) with a 550 μm front-firing laser fiber were used for the procedure. The bladder neck was opened and the median lobe vaporized using 80 W. The lateral lobes were then vaporized until a working channel was created in the prostate. Subsequently, a power of 120 W was used to complete vaporization of the median and lateral lobes until a TURP-like cavity had been achieved. At the end of the procedure, a three-way 20F silicone urethral catheter was inserted and continuous bladder irrigation with saline solution was maintained. Surgery was performed under spinal or general anesthesia, according to anesthetist's and patient's preferences.
Intraoperative irrigation was performed using isotonic saline containing 1% ethanol (Somanol®; B. Braun Medical AG, Sempach, Switzerland), which was placed 80 cm above the level of the bladder. Endexpiratory ethanol concentrations were measured at the beginning of the operation and at regular 10-min intervals (5-min intervals if ethanol was detected) throughout the procedure using an electrochemical AlcoQuant 6020 Alcohol Breathalyzer (EnviteC GmbH, Wismar, Germany) like described in detail, before. 17 Hahn's mathematical formula was used for the quantification of the total absorption volume intraoperatively. 18
Surgeons were blinded to the results of the ethanol measurements and only informed by the anesthetist, if the critical absorption volume was exceeded. This limit was adopted before intervention according to the individual patient's health condition according to pre- and intraoperative recommendations by the anesthetist.
Additionally, hemoglobin, hematocrit, sodium, potassium, chloride, creatinine, and venous blood gas analysis were assessed at the beginning of the intervention, after 30 minutes, at the end of the intervention, and 24 hours afterward. Intraoperative complications (e.g., perforation of the prostatic capsule, venous sinusoid opening, bladder neck undermining) were documented by the surgeon.
A follow-up control was performed 12 weeks postoperatively, including free uroflowmetry, postvoid residual, and IPSS.
Sample size calculation was based on the findings by Wettstein and colleagues 6 and revealed that 50 patients had to be assessed. Absorption volume of irrigation fluid during ThuVap was defined as primary endpoint. For the endpoints with a continuous scale, the median and range, and for endpoints on a categorical scale, the proportions were reported. All analyses were carried out in the R programming language (Version 3.2.3; R Core Team, 2015).
Results
A total of 54 patients were included into the study. Median age was 71 years (45–93), 1.8% of the patients had ASA Score 1, 55.6% ASA Score 2, and 42.6% ASA Score 3. Median prostate volume was 42 mL (17–80).
Median operation time was 60 minutes (20–124) with a median need of 17.5 l irrigation fluid (1.9–40) and a median energy of 182 kJ (46–488). Among 395 ethanol measurements, based on 54 patients, only 14 measurements had a value larger than zero arising from 7 patients. In these seven patients, median fluid absorption was 265 mL (227–615). Figure 1 shows the trajectories during operation time for the calculated fluid absorption.
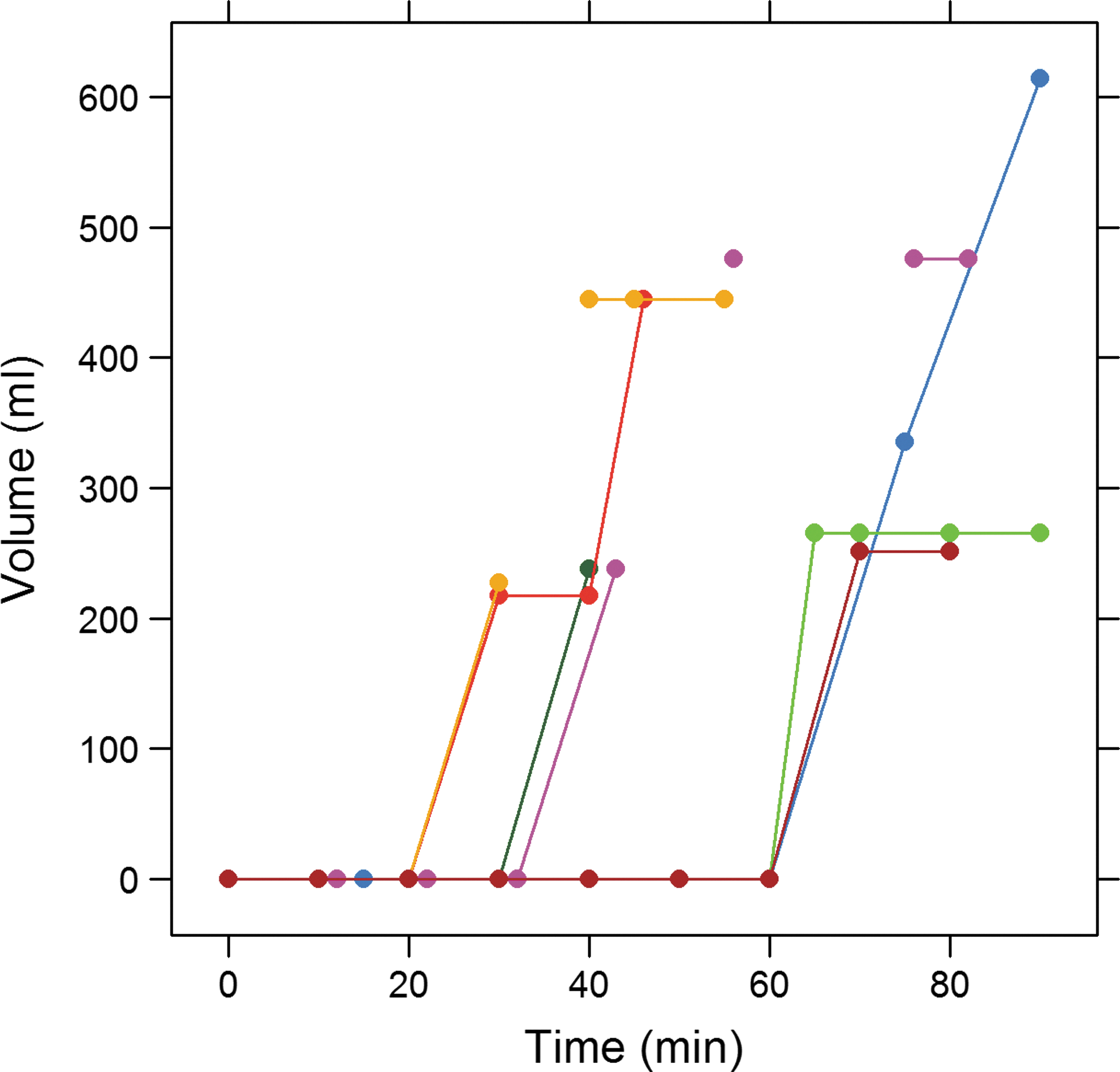
Calculated fluid absorption of absorbers during intervention (colored by patient).
Absorption volume was less than 500 mL in six patients. Only one patient had fluid absorption of 615 mL. In the majority of cases fluid absorption occurred in the second half of the intervention. Intraoperative complications were observed in two patients (venous sinusoid opening). Although both patients showed fluid absorption (251 and 615 mL, respectively), operation could be completed in both cases. No patient in the absorber group had clinical symptoms or cardiopulmonary problems intra- or postoperatively.
Comparing the absorber group with the nonabsorber group, patient age tended to be higher in the absorber group. However, this did not reach statistical significance and none of the assessed parameters could be identified as a risk factor for absorption of irrigation fluid (Table 1). Moreover, intra- and postoperative measurements of blood parameters showed no significant differences between the two groups. Median time to catheter removal postoperatively was 2 days (range 1.5–7 days) and the median postoperative hospital stay was 4 days (range 2–11 days). Table 2 shows the improvement of micturition parameters from baseline to 12-week follow-up.
IPSS = International Prostate Symptom Score.
Discussion
The aim of this study was to assess prevalence and extent of irrigation fluid absorption during ThuVaP. Thirteen percent (7/54) of our patients showed positive breath ethanol values indicating an absorption of irrigation fluid. The quantification of total fluid absorption with Hahn's mathematical formula showed a maximum absorption of 615 mL with a median amount of 265 mL (227–615). Only one patient showed fluid absorption higher than 500 mL and none of the operations had to be discontinued due to irrigation fluid absorption.
As venous sinusoid opening was only observed in two of the patients in the absorber group and no cases of capsule perforation or bladder neck undermining occurred, unnoticed opening of smaller venous sinusoids seems to be the most likely cause of fluid absorption in the remaining cases.
During the last decade, different techniques for transurethral resection, vaporization, or enucleation of the prostate have been developed and integrated into clinical routine. Most of these techniques can be performed using isotonic saline as irrigation fluid and, thus, are not associated with the risk of classical TUR syndrome. However, there is still a risk of absorption of irrigation fluid and absorbed volumes of more than 500 mL have been shown to be associated with an increased risk of myocardial infarction and neurological disturbances in patients with underlying cardiopulmonary disease. 7 This has to be considered all the more, as laser techniques are particularly used in frail patients at high risk for anesthesia, especially if anticoagulation cannot be stopped. 1 In accordance with that, only 1.8% of our patients were classified as ASA 1.
Occurrence and extent of irrigation fluid absorption has been proven for different laser techniques, previously. For example Shah and colleagues 7 found a mean fluid absorption of 459 mL (213–930) during holmium laser enucleation of the prostate. For pure transurethral bipolar plasma vaporization of the prostate, Hermanns and colleagues 19 reported on 16% of patients absorbing irrigation fluid with a median volume of 346 mL (138–2166).
Moreover, Hermanns and colleagues and Wettstein and colleagues 6 observed absorption of irrigation fluid in 44% and 41% of the patients during GreenLight laser vaporization with 120 W and 180 W, respectively. With a median of 725 mL (138–3452) and 950 mL (208–4579), respectively, absorbed fluid volume was remarkably high in both trials. All studies had a comparable sample size of about 50 patients.
Therefore, prevalence as well as extent of fluid absorption in our study are the lowest reported so far. In accordance with that, application of the thulium laser in the treatment of BPO has been shown to be a very safe procedure before, 11 especially due to its excellent hemostatic properties. 20
However, differences in the studies cited above must be interpreted with caution. On the one hand, a favorable safety profile of the thulium laser would be plausible considering its hemostatic properties and excellent visibility due to its continuous-wave mode, especially with the use of front-fire application.
On the other hand, absorption of irrigation fluid particularly occurs after venous sinusoid opening. Thus, the dimension of tissue vaporization, a factor that can be hardly standardized, seems to be crucial for the occurrence of fluid ingress. Therefore, the different techniques seem, if at all, only comparable within a randomized trial.
Our study had minor limitations: The amount of vaporized prostate tissue was not assessed in our study. In addition, no routine urodynamic examinations were performed pre- or postoperatively to support functional outcomes. However, the results of the 12-week follow-up controls indicate an appropriate functional outcome. The results of our study refer exclusively to ThuVaP. Therefore, no conclusions can be drawn for thulium vaporesection or enucleation of the prostate.
Study design and sample size of our study allowed only exploratory analyzes of potential risk factors for absorption and therefore no statistical inference was performed.
Conclusions
The risk of intraoperative absorption of irrigation fluid is also relevant in ThuVaP. Prevalence and extent of absorption in our study are the lowest reported for transurethral operation techniques so far. However, particularly in patients at a high cardiopulmonary risk, fluid absorption must be borne in mind and intraoperative monitoring using the expired breath ethanol technique should be performed in these patients.
Footnotes
Acknowledgment
The study was funded by the CTU commission of Cantonal Hospital St. Gallen (Nr. 14/08).
Author Disclosure Statement
No competing financial interests exist.